

Last updated: April 21, 2026
Quick Answer
GLP-1 retatrutide is a triple-agonist investigational peptide that activates GLP-1, GIP, and glucagon receptors simultaneously. Unlike single- or dual-agonist incretins, this three-pronged mechanism has shown notable body weight reduction and metabolic effects in clinical trials. It remains under investigation and is not yet approved for therapeutic use, but it has become one of the most discussed compounds in peptide research circles.
Key Takeaways
- Triple agonist: GLP-1 retatrutide targets three receptors (GLP-1, GIP, and glucagon) rather than one or two.
- Phase 2 data: Eli Lilly’s phase 2 trial (published in NEJM, 2023) reported up to 24.2% mean body weight reduction at the highest dose over 48 weeks.
- Not FDA-approved: As of 2026, retatrutide has not received regulatory approval for clinical use.
- Research peptide: Available through research suppliers for investigational purposes only.
- Distinct from tirzepatide: Tirzepatide is a dual agonist (GLP-1 + GIP); retatrutide adds glucagon receptor activation.
- Glucagon component: The glucagon receptor agonism may contribute to increased energy expenditure and hepatic fat reduction based on preclinical models.
- Side effect profile: Gastrointestinal effects (nausea, diarrhea, vomiting) were the most commonly reported adverse events in trials.
- Dosing is dose-dependent: Observed effects scaled with dose in clinical data, with 12 mg weekly showing the strongest outcomes.
What Is GLP-1 Retatrutide and How Does It Work?
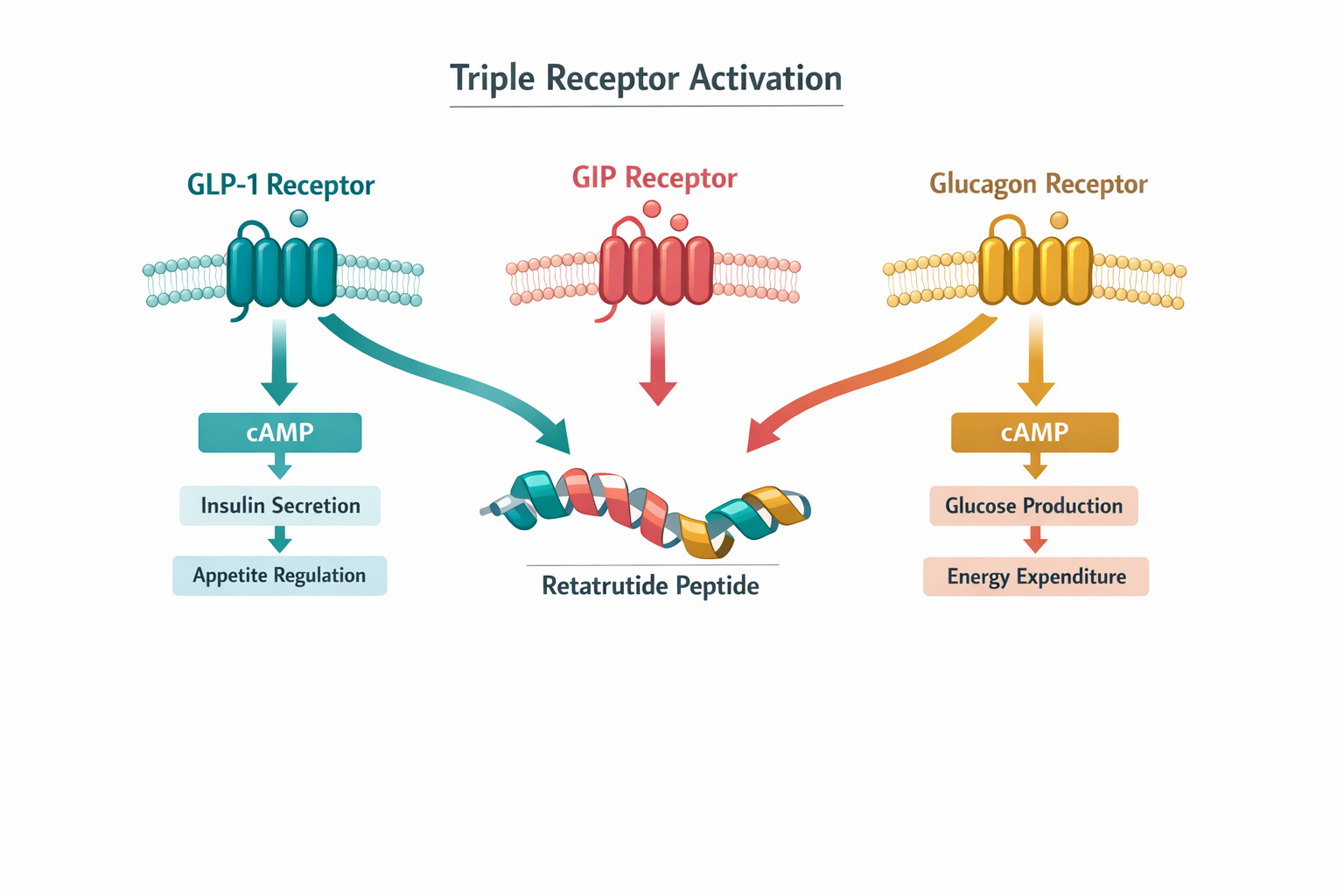
GLP-1 retatrutide (also known as LY3437943) is a single peptide molecule engineered to activate three distinct hormone receptors: GLP-1 (glucagon-like peptide-1), GIP (glucose-dependent insulinotropic polypeptide), and the glucagon receptor. This triple-agonist design sets it apart from every other incretin-based compound currently in development or on the market.
Here’s how each receptor contributes based on published research:
- GLP-1 receptor: Slows gastric emptying, promotes satiety signaling in the brain, and supports insulin secretion in a glucose-dependent manner.
- GIP receptor: Works alongside GLP-1 to enhance insulin response and may influence fat tissue metabolism. For more on GIP receptor significance, see our detailed overview.
- Glucagon receptor: Increases hepatic energy expenditure and may promote fat oxidation in the liver, a mechanism absent in GLP-1-only or dual-agonist peptides.
The combination of all three pathways in a single molecule is what makes GLP-1 retatrutide a subject of intense research interest, particularly among those studying metabolic health and body composition.
Common mistake: Confusing retatrutide with tirzepatide. Tirzepatide activates only GLP-1 and GIP receptors. Retatrutide adds the glucagon receptor, which is a fundamentally different pharmacological profile.
What Does the Clinical Research Say About GLP-1 Retatrutide?
The most cited data comes from Eli Lilly’s phase 2 randomized controlled trial, published in the New England Journal of Medicine in June 2023. That study enrolled 338 adults with obesity and tested multiple dose levels of retatrutide against placebo over 48 weeks.
Key findings from the trial:
| Dose Level | Mean Weight Reduction at 48 Weeks |
|---|---|
| 1 mg weekly | ~8.7% |
| 4 mg weekly (escalated) | ~17.1% |
| 8 mg weekly (escalated) | ~22.8% |
| 12 mg weekly (escalated) | ~24.2% |
| Placebo | ~2.1% |
Source: Jastreboff et al., NEJM, 2023
These figures represent some of the largest weight reductions observed in any incretin-class trial to date. However, phase 2 trials are smaller and designed primarily to assess dosing and safety, not to confirm efficacy at scale. Phase 3 trials are ongoing.
For researchers tracking the evolution of GLP-1 compounds, retatrutide represents what some call the “third generation” of incretin-based peptides.
Also worth exploring: our broader look at GLP-1 generational differences for context on how single, dual, and triple agonists compare across research timelines.
How Does GLP-1 Retatrutide Compare to Other Incretin Peptides?
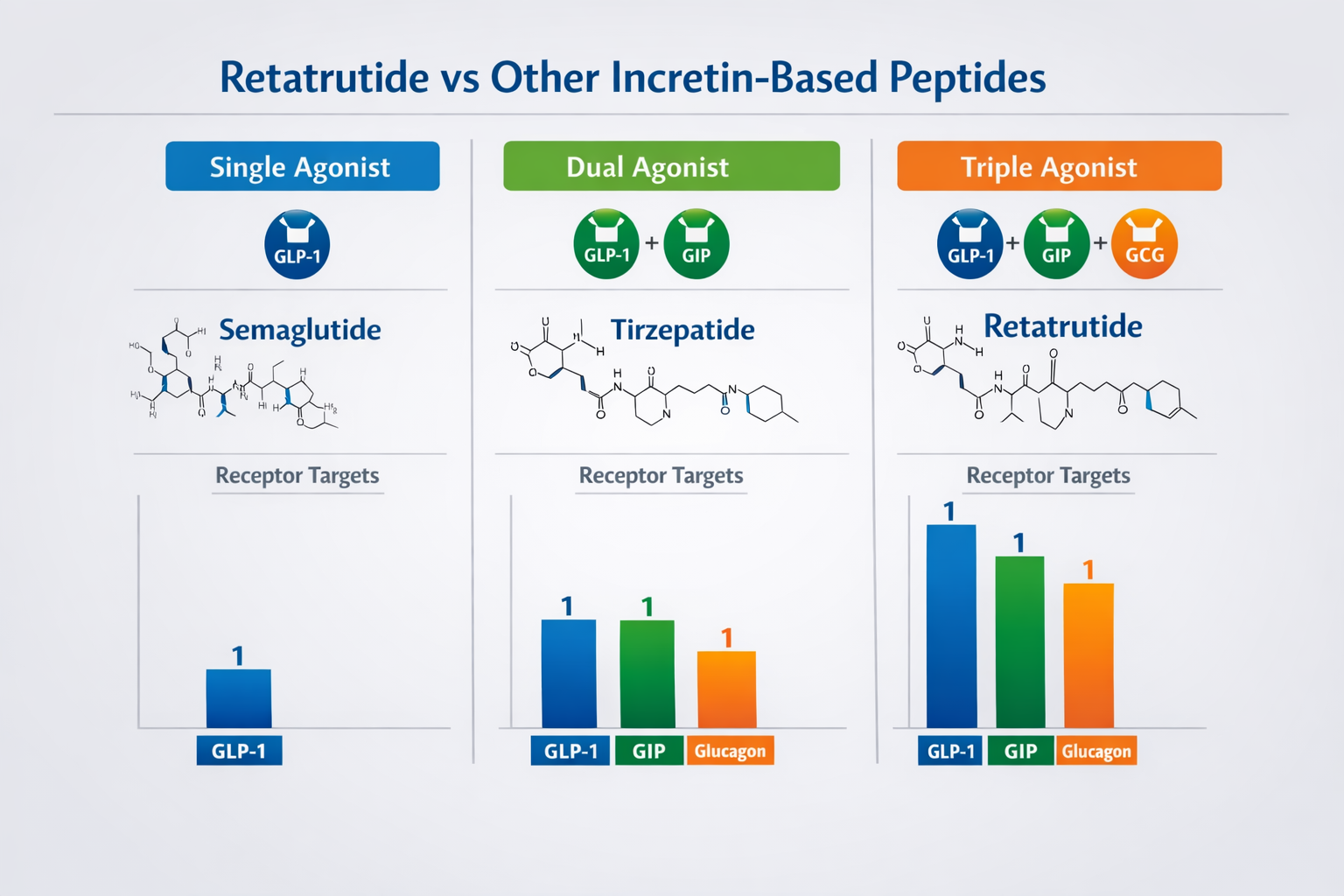
GLP-1 retatrutide differs from semaglutide and tirzepatide primarily in receptor coverage. The table below summarizes the key distinctions:
| Feature | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|
| Receptor targets | GLP-1 only | GLP-1 + GIP | GLP-1 + GIP + Glucagon |
| FDA approved | Yes | Yes | No (as of 2026) |
| Max observed weight loss (trials) | ~16% (STEP trials) | ~22.5% (SURMOUNT-1) | ~24.2% (Phase 2) |
| Glucagon-driven energy expenditure | No | No | Yes (proposed mechanism) |
| Administration | Weekly injection | Weekly injection | Weekly injection |
Choose retatrutide research if: The glucagon receptor component is specifically relevant to the study design, such as investigations into hepatic lipid metabolism or energy expenditure pathways.
Choose tirzepatide or semaglutide research if: Approved compounds with larger safety databases are preferred, or if the research question focuses on GLP-1 or GLP-1/GIP mechanisms alone.
For a deeper dive, see our resource on incretin research themes.
Browse our most popular research products for additional peptide options used in metabolic studies.
What Are the Reported Side Effects of GLP-1 Retatrutide?
Gastrointestinal side effects were the most common adverse events in the phase 2 trial. These are consistent with the known effects of GLP-1 receptor activation across the incretin class.
Reported side effects included:
- Nausea (most frequent, especially during dose escalation)
- Diarrhea
- Vomiting
- Constipation
- Decreased appetite (which overlaps with the intended mechanism)
Dose escalation protocols in the trial were designed to reduce GI tolerability issues. Higher doses (8 mg and 12 mg) used slower titration schedules, which appeared to mitigate some of the early-onset nausea.
No serious safety signals unique to GLP-1 retatrutide were identified in phase 2 data, but the sample size was limited. Phase 3 trials with larger populations will provide a clearer safety picture.
Edge case to watch: The glucagon receptor component theoretically could affect blood glucose in the opposite direction of GLP-1 (glucagon raises blood glucose). In the trial, this did not appear to cause clinically significant hyperglycemia, likely because the GLP-1 and GIP components counterbalanced it. But this remains an area of active investigation.
Who Is Researching GLP-1 Retatrutide and Why?
Interest in GLP-1 retatrutide spans several research communities:
- Metabolic researchers studying obesity, insulin resistance, and body composition changes
- Hepatology researchers investigating non-alcoholic fatty liver disease (NAFLD/MASH), where the glucagon component may offer liver-specific benefits
- Peptide science investigators comparing multi-agonist approaches to single-target therapies
- Biohackers and longevity enthusiasts tracking next-generation metabolic peptides for future applications
The compound is particularly interesting for researchers who want to study the additive or synergistic effects of activating three metabolic pathways at once, rather than sequentially or in isolation.
For those also exploring body composition research peptides, our overview of tesa and body composition research provides complementary context on GH-related pathways.
Where Can Researchers Source GLP-1 Retatrutide?
As a research peptide, GLP-1 retatrutide is available through specialized peptide suppliers for investigational use. When selecting a source, researchers should verify:
- Third-party testing: Look for suppliers that provide certificates of analysis (COA). See our COA documentation page for an example of what proper testing looks like.
- Purity standards: Research-grade peptides should meet a minimum of 98% purity by HPLC.
- Proper storage and handling: Lyophilized peptides require specific storage conditions (typically -20°C) to maintain stability.
- Clear labeling: The product should be labeled for research use only, not for human consumption.
Explore our retatrutide product listings for available options with full COA documentation.
Check out our most popular products page for a broader view of research peptides currently in demand.
What Questions Should Researchers Ask Before Starting a Retatrutide Study?
Before incorporating GLP-1 retatrutide into a research protocol, consider these practical questions:
- What is the specific research question? Triple agonism is only relevant if the study design benefits from glucagon receptor activation alongside GLP-1 and GIP.
- What comparators are appropriate? If comparing to approved drugs, semaglutide or tirzepatide may serve as relevant controls.
- Is the peptide sourced with verifiable purity? Without a valid COA, results may not be reproducible.
- What dose escalation protocol will be used? The phase 2 trial used specific titration schedules that researchers should review before designing their own protocols.
- Are there institutional review requirements? Depending on the research setting, ethics board or institutional approval may be necessary.
Frequently Asked Questions
Is GLP-1 retatrutide FDA-approved?
No. As of 2026, retatrutide has not received FDA approval. It remains an investigational compound in clinical trials sponsored by Eli Lilly.
How is retatrutide different from semaglutide?
Semaglutide activates only the GLP-1 receptor. GLP-1 retatrutide activates three receptors: GLP-1, GIP, and glucagon.
What was the maximum weight loss observed in trials?
The phase 2 trial reported a mean reduction of 24.2% body weight at the 12 mg dose over 48 weeks (Jastreboff et al., NEJM, 2023).
Is retatrutide the same as tirzepatide?
No. Tirzepatide is a dual agonist (GLP-1 + GIP). Retatrutide is a triple agonist that also activates the glucagon receptor.
What are the main side effects?
Nausea, diarrhea, vomiting, and constipation were the most commonly reported adverse events in clinical trials.
Can I buy retatrutide for personal use?
Retatrutide is sold as a research peptide only. It is not approved for therapeutic or personal use. Browse available research peptides for investigational purposes.
Does the glucagon component raise blood sugar?
In the phase 2 trial, the GLP-1 and GIP components appeared to counterbalance glucagon’s glucose-raising effect. No clinically significant hyperglycemia was reported, but this remains under study.
How often is retatrutide administered?
In clinical trials, it was administered as a once-weekly subcutaneous injection.
When might retatrutide receive FDA approval?
Phase 3 trials are ongoing. No specific approval timeline has been confirmed by Eli Lilly as of early 2026.
Conclusion
GLP-1 retatrutide stands out in the incretin peptide space because of its unique triple-agonist mechanism. The phase 2 clinical data is compelling, but it remains investigational. For researchers, biohackers, and longevity enthusiasts tracking the next wave of metabolic peptides, retatrutide is worth following closely.