

GLP-3 Retatrutide Mechanism of Action Explained: Triple Agonism, Appetite Signaling, and Energy Expenditure
Forty-five percent of participants in a landmark 2026 obesity trial lost more than 30% of their body weight from a single weekly injection, a result previously reserved for bariatric surgery. That compound is retatrutide, and its extraordinary performance comes down to a precise molecular strategy: simultaneous activation of three metabolic receptors. Understanding the GLP-3 Retatrutide mechanism of action explained through triple agonism, appetite signaling, and energy expenditure is essential for researchers, clinicians, and anyone tracking the frontier of metabolic science.
Key Takeaways
- Retatrutide activates GLP-1, GIP, and glucagon receptors simultaneously, producing effects no single or dual agonist can replicate.
- Glucagon receptor activation is the distinguishing feature that drives enhanced energy expenditure and fat oxidation beyond appetite suppression alone.
- In the TRIUMPH-1 trial, participants on 12 mg lost an average of 70.3 lbs (28.3% of body weight) over 80 weeks.
- The peptide's fatty acid side chain enables albumin binding, supporting a convenient once-weekly dosing schedule.
- Beyond weight loss, retatrutide shows clinically meaningful improvements in type 2 diabetes, sleep apnea, and osteoarthritis pain.
The Structural Foundation Behind Triple Agonism
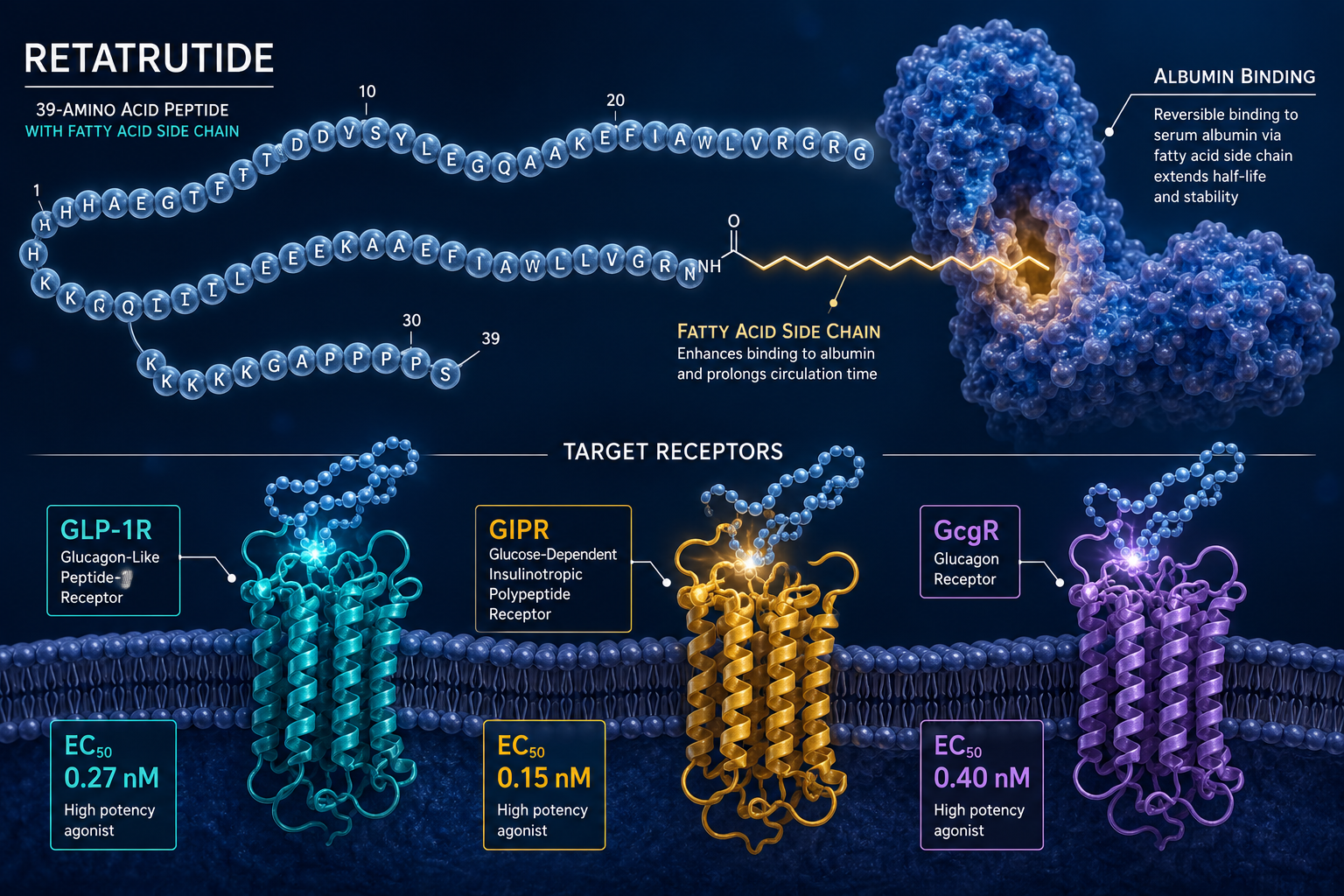
Retatrutide is a 39-amino acid peptide engineered with a fatty acid side chain. That side chain binds to albumin in the bloodstream, extending the compound's half-life to approximately six days. The practical result is once-weekly dosing, a significant advantage for sustained research protocols and patient adherence.
What sets retatrutide apart structurally is its receptor potency profile:
| Receptor | EC50 (nM) | Primary Effect |
|---|---|---|
| GIP Receptor (GIPR) | 0.0643 | Insulin secretion, fat metabolism |
| GLP-1 Receptor (GLP-1R) | 0.775 | Appetite suppression, glucose control |
| Glucagon Receptor (GcgR) | 5.79 | Energy expenditure, fat oxidation |
The compound shows the highest potency at the GIP receptor, followed by GLP-1, then glucagon. This gradient is intentional. GIP and GLP-1 agonism work synergistically on insulin release and satiety, while glucagon agonism, typically avoided in metabolic drugs due to hyperglycemia risk, is carefully balanced to drive thermogenesis without destabilizing blood glucose.
Researchers exploring related metabolic peptide pathways can find additional context in the metabolic modulation research lines overview, which covers complementary compounds under active investigation.
How Appetite Signaling and Energy Expenditure Work Together
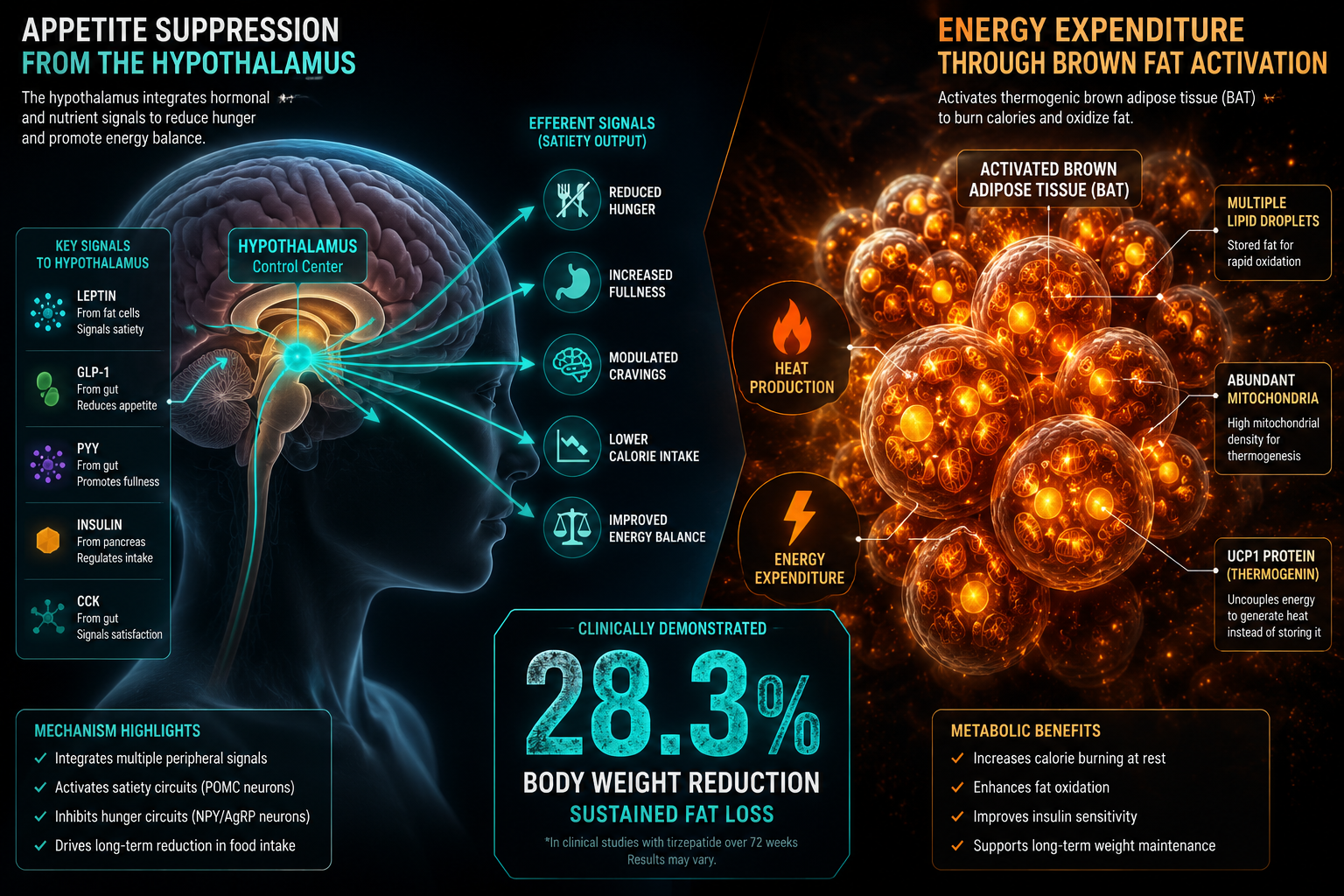
The GLP-3 Retatrutide mechanism of action explained through appetite signaling begins in the hypothalamus. GLP-1 receptor activation slows gastric emptying and signals satiety centers in the brain, reducing caloric intake. GIP receptor activation amplifies insulin secretion in a glucose-dependent manner, lowering postprandial glucose spikes while also modulating fat storage in adipose tissue.
The glucagon component is where retatrutide diverges from its predecessors.
"The addition of glucagon receptor activation may play a key role in enhancing weight loss beyond what GLP-1 and GIP agonism achieve alone."
Glucagon receptor activation increases hepatic glucose output under fasting conditions, but more critically for obesity research, it stimulates thermogenesis in brown adipose tissue and promotes fatty acid oxidation. This creates a dual-pathway effect: the body consumes fewer calories through appetite suppression while simultaneously burning more through elevated energy expenditure.
This mechanism contrasts with earlier GLP-1 generation drugs. For a deeper look at how incretin-based therapies have evolved, the generations of GLP-1 differences resource provides useful comparative context.
Researchers studying overlapping metabolic pathways may also find value in reviewing 5-Amino-1MQ, a NNMT inhibitor that targets fat cell metabolism through a distinct but complementary mechanism.
Clinical Evidence: What the Data Shows in 2026
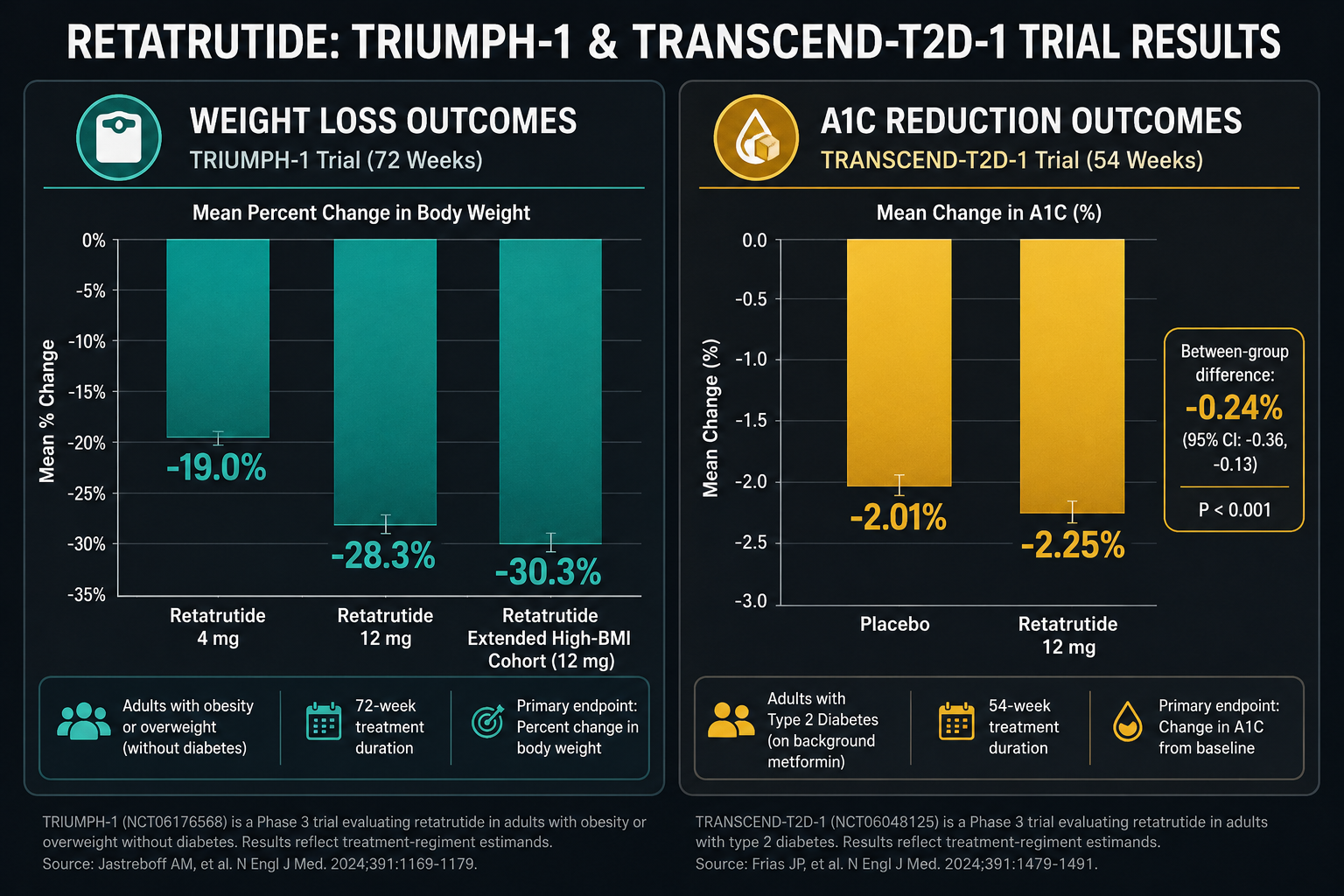
The TRIUMPH-1 Phase 3 trial delivered the most compelling data yet. Participants receiving 12 mg of retatrutide lost an average of 70.3 lbs (28.3% of body weight) over 80 weeks. Among those with a baseline BMI of 35 or higher who continued into a study extension, average weight loss reached 85.0 lbs (30.3%) at 104 weeks.
Even the lower 4 mg dose produced meaningful results: an average of 47.2 lbs (19.0%) lost over 80 weeks, with a favorable discontinuation profile compared to placebo.
The TRANSCEND-T2D-1 trial, reported in March 2026, showed retatrutide achieving A1C reductions of up to 2.0% and weight loss of up to 36.6 lbs (16.8%) at 40 weeks in adults with type 2 diabetes. Up to 46% of participants reached normal A1C levels.
Beyond metabolic markers, retatrutide reduced knee osteoarthritis pain by up to 73.1% and decreased obstructive sleep apnea severity by up to 60.6 events per hour, outcomes that reflect the systemic reach of triple receptor agonism.
Common side effects include nausea, vomiting, and dysesthesia. Some participants discontinued due to rapid weight loss, underscoring the importance of careful monitoring.
Eli Lilly is conducting additional late-stage trials with potential FDA approval sought by end of 2026.
For researchers working with GLP-based compounds, the GLP-3 for sale: triple agonist research planning and catalog navigation page offers practical sourcing and protocol guidance. Those seeking specific product details can also review the GLP-3 Retatrutide research catalog entry directly.
Researchers interested in how growth hormone-related peptides interact with metabolic outcomes may also find the Tesamorelin body composition research themes page a useful adjacent resource.
Conclusion
Retatrutide's triple agonism, targeting GLP-1, GIP, and glucagon receptors with precision-tuned potency, represents a genuine leap in metabolic research. The mechanism is not simply additive; the glucagon component introduces an energy expenditure dimension that earlier incretin therapies could not access. Combined with appetite suppression and improved insulin dynamics, this produces weight loss outcomes that rival surgical intervention.
Actionable next steps for researchers:
- Review the receptor potency profile carefully when designing dosing protocols; GIP receptor sensitivity is highest and may drive early responses.
- Monitor for nausea and dysesthesia, particularly during dose escalation phases.
- Consider how triple agonism data intersects with other metabolic modulators in your research stack.
- Consult the Retatrutide GLP-3 research overview for updated sourcing, purity standards, and protocol references before initiating any study.
The science behind retatrutide is still unfolding, but the 2026 clinical data makes one thing clear: three receptors, activated together, can accomplish what none could achieve alone.