Enclomiphene Alternatives in Hormone Research: How It Compares With serms and Estrogen-Signaling Models
Fewer than 15% of men with secondary hypogonadism who seek hormone optimization are offered a fertility-preserving option before starting exogenous testosterone. That gap is exactly why researchers and clinicians are scrutinizing enclomiphene alternatives in hormone research: how it compares with serms and estrogen-signaling models has become one of the most practically important questions in modern endocrine science.
Key Takeaways
- Enclomiphene is the pure estrogen-receptor antagonist isomer of clomiphene, stimulating endogenous testosterone without suppressing fertility.
- Compared to full clomiphene and other serms like tamoxifen, enclomiphene produces fewer mixed estrogenic side effects.
- Gonadorelin operates downstream of enclomiphene in the HPG axis and requires more frequent dosing with less predictable outcomes.
- As of 2026, enclomiphene lacks FDA approval for male hypogonadism despite completing Phase III trials.
- Researchers evaluating estrogen-signaling models benefit from understanding where each serm sits within the hypothalamic-pituitary-gonadal (HPG) axis.
Understanding Enclomiphene Within the serm Landscape
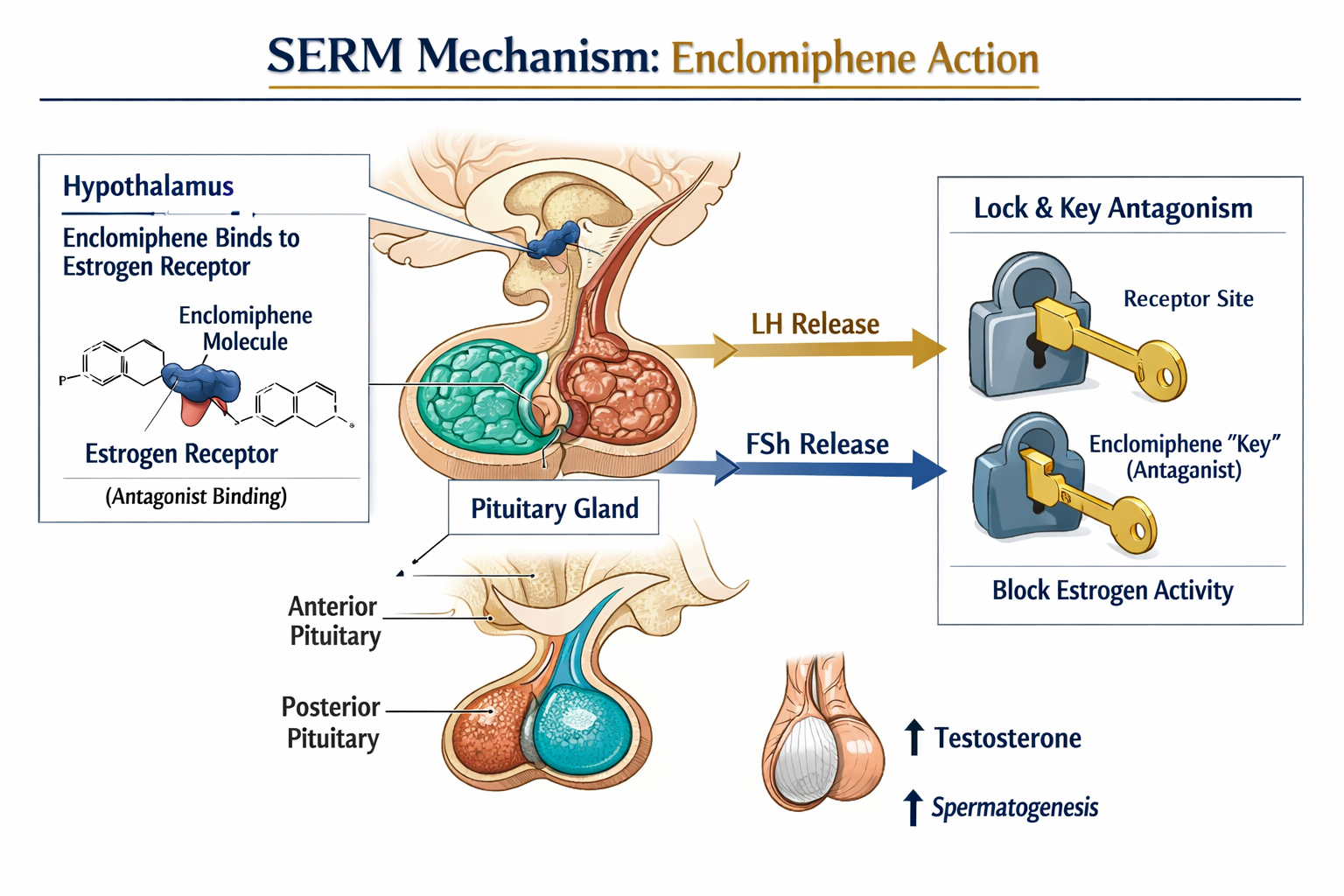
Enclomiphene is the trans-isomer of clomiphene citrate. Its defining feature is pure estrogen receptor antagonism at the hypothalamus and pituitary. By blocking estrogen's negative feedback signal at those sites, it disinhibits GnRH pulse generation, which in turn raises LH and FSH. Elevated gonadotropins then drive testicular Leydig cells to produce more testosterone and Sertoli cells to support spermatogenesis.
This mechanism places enclomiphene firmly within the serm class, yet it behaves differently from its closest relatives:
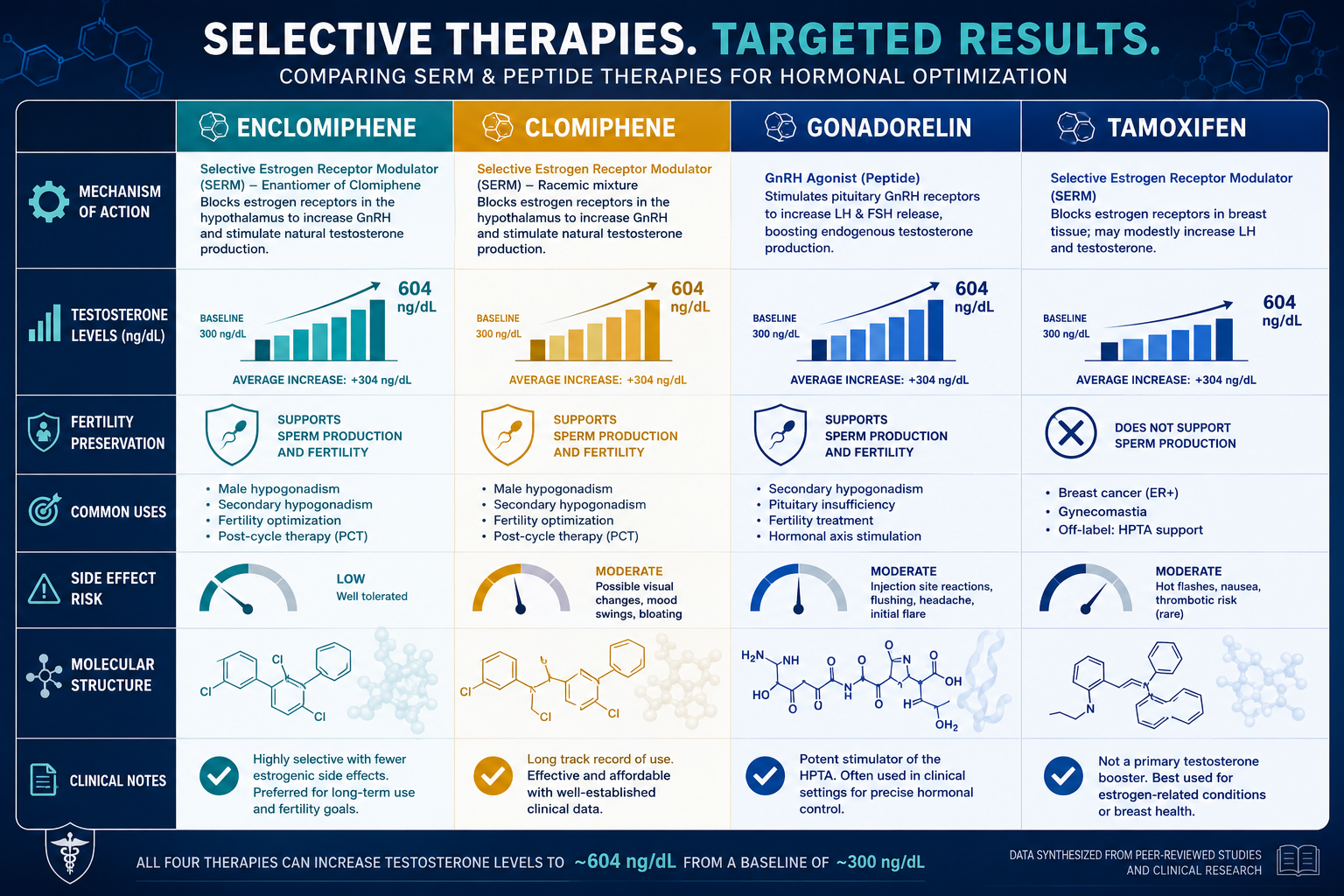
| Compound | Receptor Action | Fertility Impact | Oral Dosing |
|---|---|---|---|
| Enclomiphene | Pure antagonist (hypothalamus/pituitary) | Preserved or enhanced | Once daily |
| Clomiphene (mixed) | Antagonist + agonist (zuclomiphene component) | Generally preserved | Once daily |
| Tamoxifen | Tissue-selective antagonist/agonist | Variable | Once daily |
| Gonadorelin | GnRH agonist (pituitary direct) | Preserved | Multiple daily injections |
Clomiphene citrate contains both enclomiphene and zuclomiphene. The zuclomiphene isomer carries mixed agonist/antagonist activity and a longer half-life, which can produce residual estrogenic effects. Enclomiphene isolates the beneficial antagonism while eliminating that estrogenic noise — a meaningful distinction in research models focused on clean receptor-pathway analysis.
Tamoxifen is another well-studied serm. While it shares the ability to raise gonadotropins, its tissue-selective profile differs substantially. A 2023 systematic review found that serm-based estrogen-receptor modulation significantly raised total testosterone in men with androgen deficiency while preserving gonadotropin output — validating the broader class but not distinguishing individual agents.
For researchers studying growth hormone and metabolic signaling alongside HPG-axis dynamics, AOD9604 metabolic research themes offer a complementary perspective on peptide-level hormonal modulation.
Comparing Enclomiphene Alternatives in Hormone Research: How It Compares With serms and Estrogen-Signaling Models
When researchers map enclomiphene against other endocrine tools, three dimensions matter most: axis entry point, receptor selectivity, and downstream fertility effects.
Gonadorelin: Downstream but Demanding
Gonadorelin acts directly on the pituitary rather than at the hypothalamic level. It stimulates LH and FSH release without requiring the hypothalamic GnRH step that enclomiphene unlocks indirectly. However, gonadorelin demands multiple daily injections and shows variable efficacy depending on pituitary reserve — a significant limitation in longitudinal research protocols.
"Enclomiphene's oral once-daily dosing and single-point HPG intervention make it a more tractable tool for controlled research designs than pulsatile GnRH analogues."
Dosage and Measurable Outcomes
Clinical trials have studied enclomiphene at 6.25 mg to 25 mg daily. A 25 mg dose raised total testosterone to approximately 604 ng/dL at six weeks — comparable to testosterone gel — while maintaining sperm parameters. That dual endpoint (testosterone plus fertility preservation) is rarely achievable with exogenous hormone replacement.
Researchers working with peptide-based hormonal tools can find adjacent data in CJC-1295 with DAC research and ipamorelin versus tesa comparisons, which illustrate how axis-entry point shapes downstream hormone profiles.
Regulatory Context in 2026
Despite completing Phase III trials with positive results, enclomiphene remains unapproved by the FDA for male hypogonadism. It is available through compounding pharmacies, which introduces variability in purity and dosing — a critical consideration for research reproducibility. This regulatory gap distinguishes it from clomiphene, which holds FDA approval for female infertility.
For broader context on peptide purity and sourcing standards, the complete guide to peptide therapy addresses quality benchmarks relevant to any research compound.
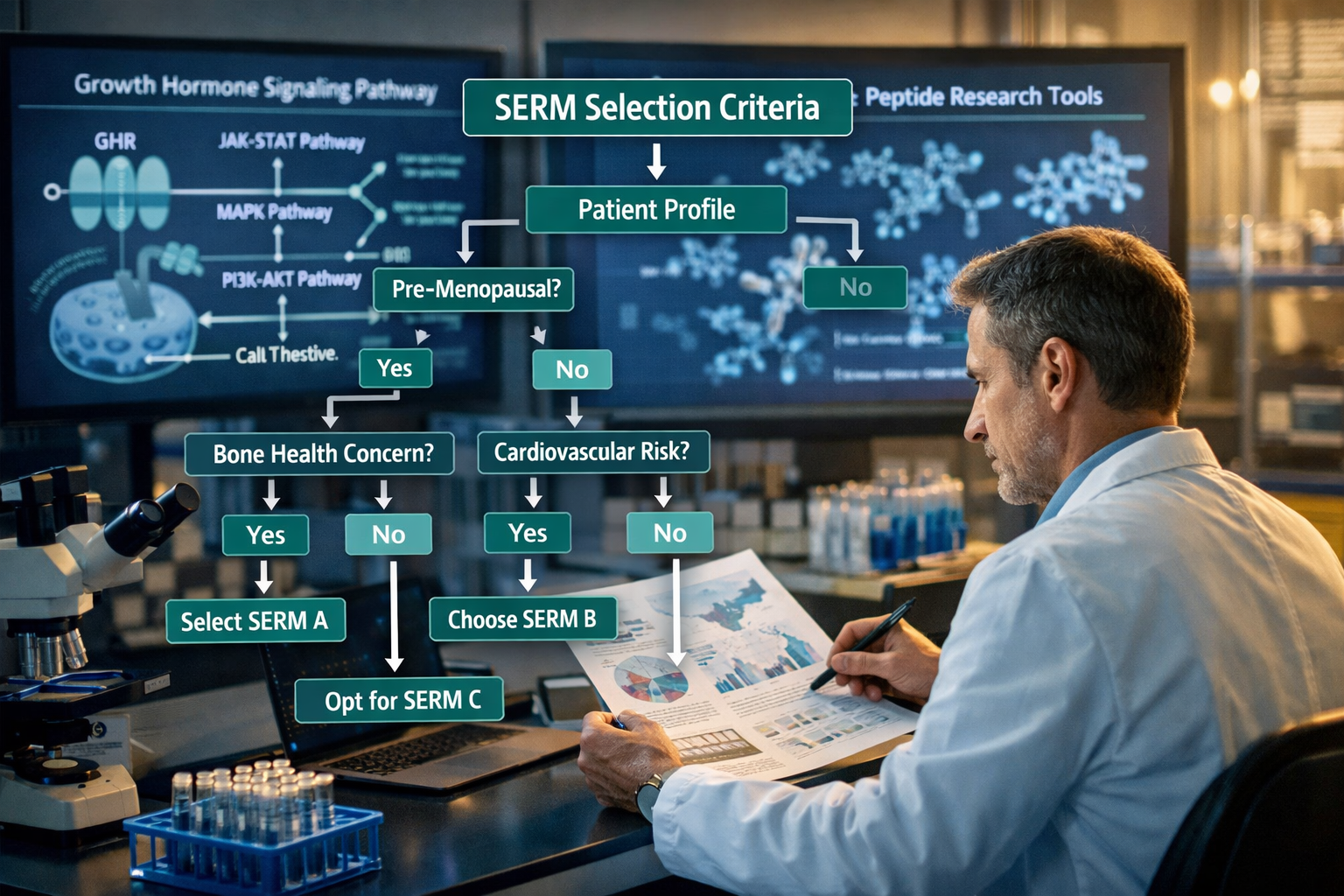
Practical Decision Framework for Researchers
When selecting between enclomiphene and its alternatives, the following criteria help structure the comparison:
- Axis entry point: Hypothalamic (enclomiphene, tamoxifen) vs. pituitary-direct (gonadorelin)
- Receptor purity: Pure antagonism (enclomiphene) vs. mixed activity (clomiphene)
- Dosing complexity: Once-daily oral (enclomiphene, tamoxifen) vs. multiple injections (gonadorelin)
- Fertility preservation: Critical for male reproductive research models
- Side effect profile: Enclomiphene is generally well-tolerated; reported effects include visual disturbances, headaches, and mood changes
Researchers also exploring cellular protection and longevity signaling alongside hormonal axes may find value in GHK-Cu longevity research themes and MOTS-c mechanism and research, which intersect with mitochondrial and metabolic hormone pathways.
For those comparing epigenetic and telomere-related signaling tools, Epithalon vs NAD evidence provides a useful parallel framework for evaluating competing research compounds.
Conclusion
Enclomiphene alternatives in hormone research — how it compares with serms and estrogen-signaling models — is not a theoretical exercise. It is a practical decision that shapes research design, data quality, and translational relevance. Enclomiphene's pure antagonism, oral convenience, and fertility-preserving profile give it a distinct position within the serm class, even as its lack of FDA approval in 2026 creates sourcing challenges.
Actionable next steps for researchers:
- Map your research question to the specific HPG-axis node you need to modulate before selecting a compound.
- Evaluate receptor selectivity data for each serm candidate, not just testosterone-elevation endpoints.
- Prioritize sourcing from suppliers with documented purity testing to ensure reproducible outcomes.
- Cross-reference findings with adjacent peptide signaling research to build a fuller hormonal picture.