
Estrogen Receptor Signaling and Enclomiphene: How ER and LH Pathways Inform Male Endocrine Research
Male testosterone levels have declined measurably across populations over the past several decades, yet the molecular machinery governing male hormone regulation remains underappreciated outside specialist circles. At the center of this biology sits a counterintuitive truth: estrogen receptors are not just a female concern. Estrogen receptor signaling and enclomiphene — and how ER and LH pathways inform male endocrine research — represent one of the most productive intersections in modern reproductive endocrinology.
Key Takeaways
- Estrogen receptors ERα and ERβ both play active roles in male hormonal regulation, particularly within the hypothalamic-pituitary-gonadal (HPG) axis.
- Enclomiphene is the trans-isomer of clomiphene citrate and functions as a selective estrogen receptor modulator (serm) that blocks hypothalamic ERα to stimulate LH and FSH release.
- Clinical data show enclomiphene raises testosterone comparably to clomiphene while producing significantly lower estradiol increases and fewer side effects.
- Membrane-localized estrogen receptor 1 (mESR1) has a distinct, nongenomic role in male fertility that is separate from classical nuclear ER signaling.
- Research on enclomiphene provides a practical model for studying selective ER modulation without suppressing the HPG axis.
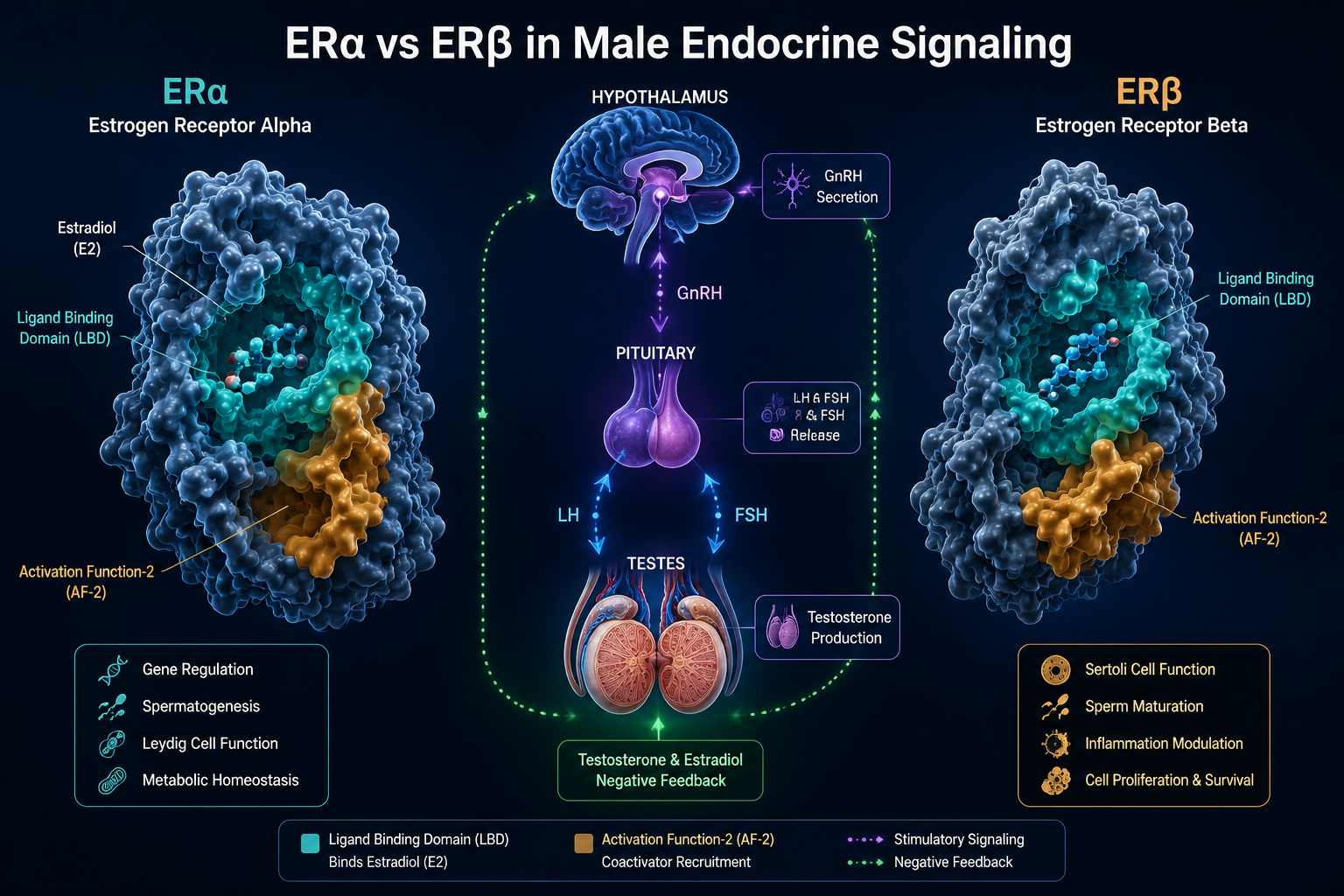
ERα and ERβ: The Two Receptors Driving Male Hormonal Balance
Estrogen actions in males are mediated by two primary receptor subtypes: ERα (encoded by the ESR1 gene) and ERβ (encoded by ESR2). These receptors differ in ligand binding affinity, tissue distribution, and transcriptional output.
| Receptor | Primary Male Tissue Sites | Key Function |
|---|---|---|
| ERα | Hypothalamus, bone, liver | Negative feedback on GnRH/LH release |
| ERβ | Testis, epididymis, prostate | Local spermatogenesis support |
In the hypothalamus, ERα is the dominant subtype mediating estradiol's negative feedback on gonadotropin-releasing hormone (GnRH) pulsatility. When circulating estradiol binds ERα, it suppresses GnRH release, which in turn reduces pituitary output of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Less LH means less Leydig cell stimulation and lower endogenous testosterone production.
Beyond classical nuclear signaling, research published in 2024 identified membrane-localized estrogen receptor 1 (mESR1) as a separate and critical player. Male mice lacking mESR1 developed progressive infertility due to testicular and reproductive tract abnormalities, even when nuclear ERα signaling remained intact. This finding points to a nongenomic signaling layer that standard receptor models do not fully capture.
Researchers exploring broader endocrine signaling networks — including those studying GLP-1 and dual receptor agonism — recognize that receptor subtype specificity has major implications for how compounds are designed and interpreted.
Enclomiphene Mechanism: Selective ER Blockade and the LH Pathway
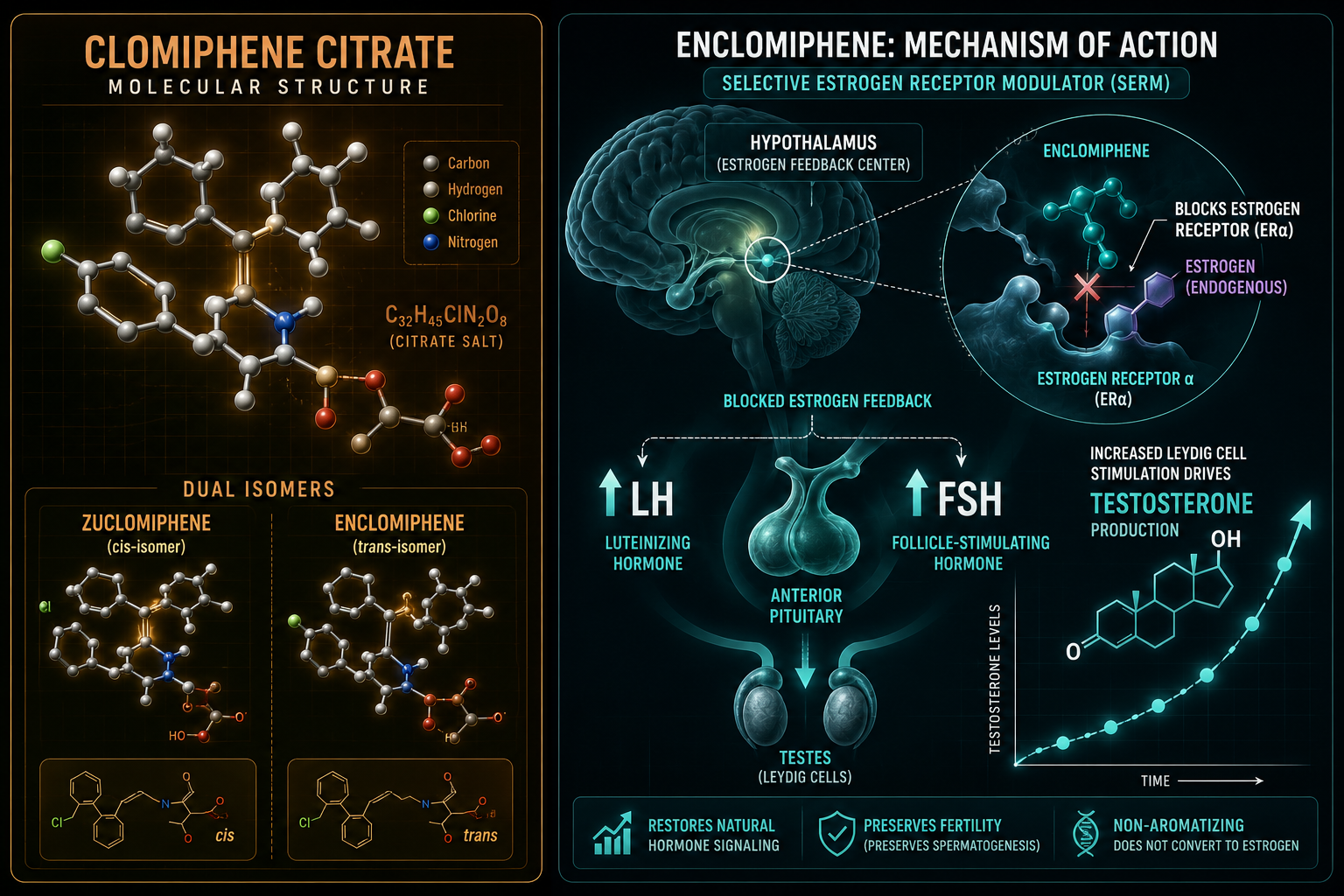
Enclomiphene is the trans-isomer of clomiphene citrate. Its counterpart, zuclomiphene (the cis-isomer), has estrogenic properties and a much longer half-life. By isolating the trans-isomer, researchers gain a cleaner pharmacological tool for studying selective ER modulation in male subjects.
How enclomiphene works:
- Binds competitively to ERα in the hypothalamus
- Blocks estradiol from suppressing GnRH pulsatility
- GnRH pulses increase, driving pituitary LH and FSH secretion
- Elevated LH stimulates Leydig cells to produce testosterone
- The HPG axis remains intact and functional throughout
This mechanism preserves the body's own hormonal feedback loop — a meaningful distinction from exogenous testosterone replacement, which suppresses the HPG axis and reduces endogenous production.
Enclomiphene has a half-life of approximately 10 to 15 hours and is typically studied at oral doses ranging from 12.5 to 25 mg per day. One study demonstrated measurable testosterone increases within just 14 days of administration, underscoring the speed of HPG axis responsiveness when hypothalamic ER blockade is applied.
This targeted approach to endocrine modulation parallels research on other selective compounds. For example, serm stack research explores how combining receptor-selective agents can produce synergistic hormonal outcomes. Similarly, researchers working with ipamorelin as a GHRH secretagogue are familiar with the principle of stimulating endogenous hormone release rather than replacing it directly.
Clinical Research Findings: What the Data Show in 2026
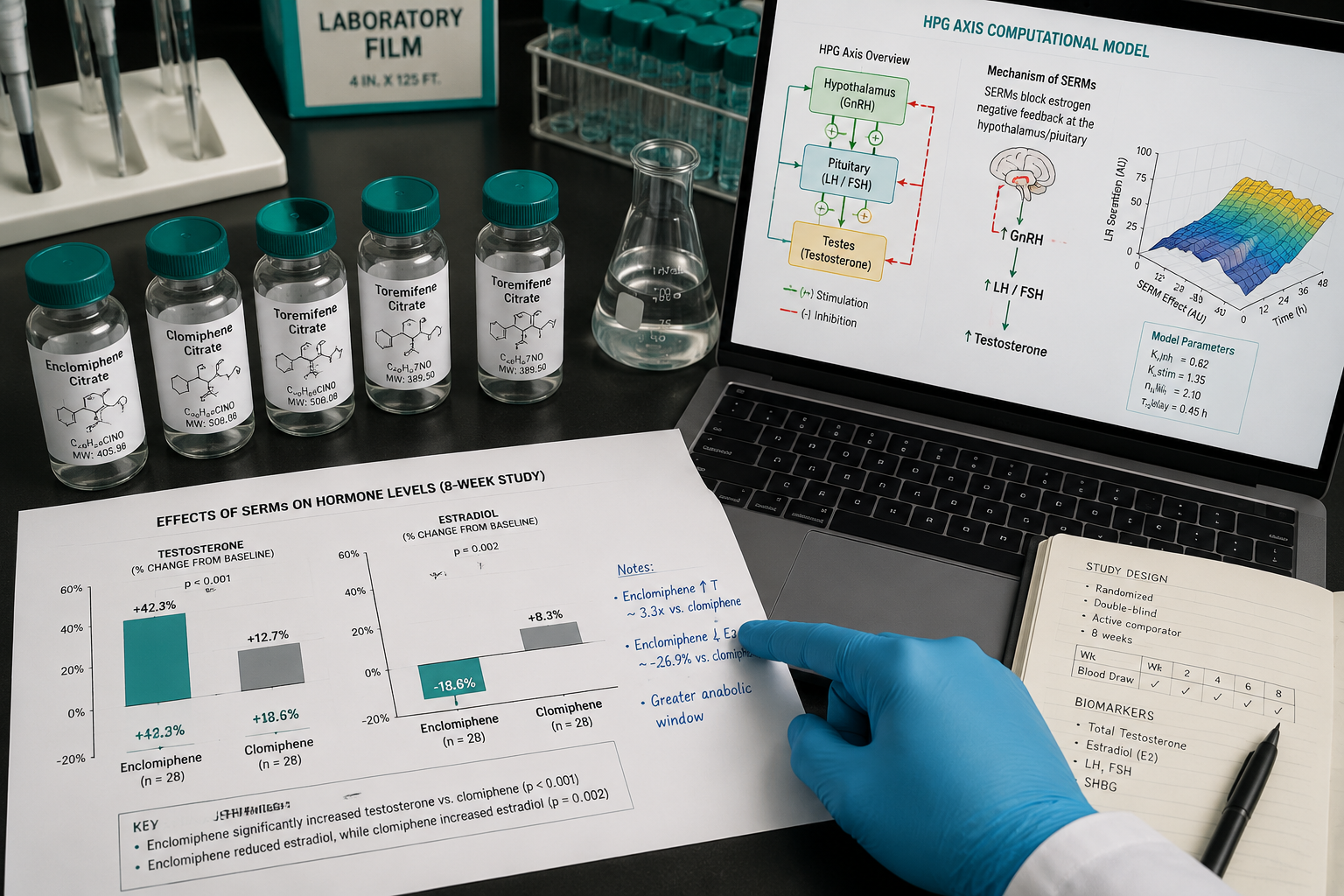
The clinical picture for enclomiphene in male hypogonadism research has sharpened considerably. A retrospective cohort study found that both enclomiphene and clomiphene significantly increased testosterone, with a mean rise of approximately 210 ng/dL across groups. The two compounds showed no statistically significant difference in testosterone outcomes.
Where enclomiphene diverges from clomiphene:
- Estradiol increase: Enclomiphene produced a significantly lower estradiol rise (approximately -5.92 pg/mL vs. +17.50 pg/mL for clomiphene, P=0.001)
- Side effect profile: Fewer reports of decreased libido, reduced energy, and mood changes with enclomiphene
- Median testosterone gain: Approximately 166 ng/dL in comparative studies
The lower estradiol elevation seen with enclomiphene is directly attributable to the absence of zuclomiphene, which carries estrogenic activity. This makes enclomiphene a more precise research instrument when the goal is to study LH-driven testosterone stimulation without confounding estrogenic effects.
A 2025 systematic review and meta-analysis further evaluated serms against testosterone gel, human chorionic gonadotropin (hCG), anastrozole, and placebo in men with baseline testosterone at or below 300 ng/dL. As of 2026, enclomiphene has accumulated over 190 indexed citations including clinical trials, randomized controlled trials, and meta-analyses — a growing evidence base for a compound that was once considered a secondary isomer.
Researchers interested in how metabolic and hormonal pathways intersect may also find value in reviewing muscle and fat research themes related to ipamorelin and AOD9604 metabolic research, both of which touch on endocrine-metabolic crosstalk. Computational modeling advances have also improved understanding of pituitary gonadotropin signaling dynamics within the HPG axis, offering new tools for interpreting serm research data.
For those tracking broader developments in the field, the latest peptide research updates provide relevant context on how receptor-targeted compounds continue to evolve.
Conclusion
Estrogen receptor signaling and enclomiphene — and how ER and LH pathways inform male endocrine research — offer a precise window into the HPG axis that few other research tools match. The distinction between ERα and ERβ, the newly recognized role of mESR1 in nongenomic male fertility signaling, and enclomiphene's clean pharmacological profile collectively make this an area of high research value.
Actionable next steps for researchers:
- Prioritize ERα-specific assays when studying hypothalamic feedback in male subjects
- Use enclomiphene as a mechanistic comparator to isolate LH-driven testosterone responses from estrogenic confounders
- Track estradiol alongside testosterone in any serm-related endocrine study to capture the full hormonal picture
- Consult the growing meta-analytic literature to benchmark expected testosterone and estradiol response ranges
- Consider how nongenomic ER signaling (mESR1) may require separate experimental models beyond standard nuclear receptor assays