Enclomiphene vs Clomiphene: Estrogen Receptor Signaling, LH/FSH Response, and Research Use Cases
{"cover":"Professional landscape format (1536×1024) hero image with bold text overlay: 'Enclomiphene vs Clomiphene' in extra large 72pt white sans-serif font with dark semi-transparent overlay box, centered upper third. Background shows a split-panel scientific illustration: left side depicts molecular estrogen receptor binding diagram in deep teal, right side shows a stylized pituitary-hypothalamus axis with LH/FSH hormone cascade arrows in amber. Color scheme: deep navy, clinical white, amber accents. Magazine cover aesthetic, editorial quality, high contrast.","content":["Detailed landscape format (1536×1024) scientific infographic showing a side-by-side molecular comparison of enclomiphene trans-isomer and zuclomiphene cis-isomer chemical structures rendered in 3D ball-and-stick models against a dark navy background. Arrows indicate estrogen receptor binding sites on hypothalamic tissue cross-section. Color-coded labels highlight serm activity zones. Clean clinical aesthetic with white annotation text, teal and amber color accents, editorial research illustration style.","Landscape format (1536×1024) data visualization showing dual bar charts comparing LH and FSH hormone response levels between enclomiphene and clomiphene treatment groups. Chart includes testosterone ng/dL increase annotations (166 vs 98 ng/dL), estradiol pg/mL delta markers, and a timeline axis showing 2-4 week onset. Background is a soft gradient from white to light blue suggesting a clinical research environment. Bold sans-serif axis labels, color-coded bars in teal versus amber, clean medical data aesthetic.","Landscape format (1536×1024) editorial research scene showing a laboratory bench with open scientific journals, molecular model kits, and a digital tablet displaying a fertility preservation diagram with sperm viability graphs. A gloved researcher hand points to a hypothalamic-pituitary-gonadal axis flowchart pinned to a corkboard. Warm lab lighting, shallow depth of field, teal and amber accent colors, professional research environment aesthetic with subtle text overlay reading 'Research Use Cases: Secondary Hypogonadism'."]
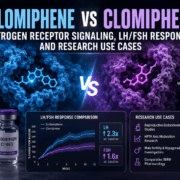
Only 38% of clomiphene citrate is the isomer actually responsible for driving testosterone production. That single pharmacological fact is at the center of the growing scientific conversation around enclomiphene vs clomiphene: estrogen receptor signaling, LH/FSH response, and research use cases — and it explains why researchers and clinicians are increasingly treating these two compounds as distinct tools rather than interchangeable options.
Key Takeaways
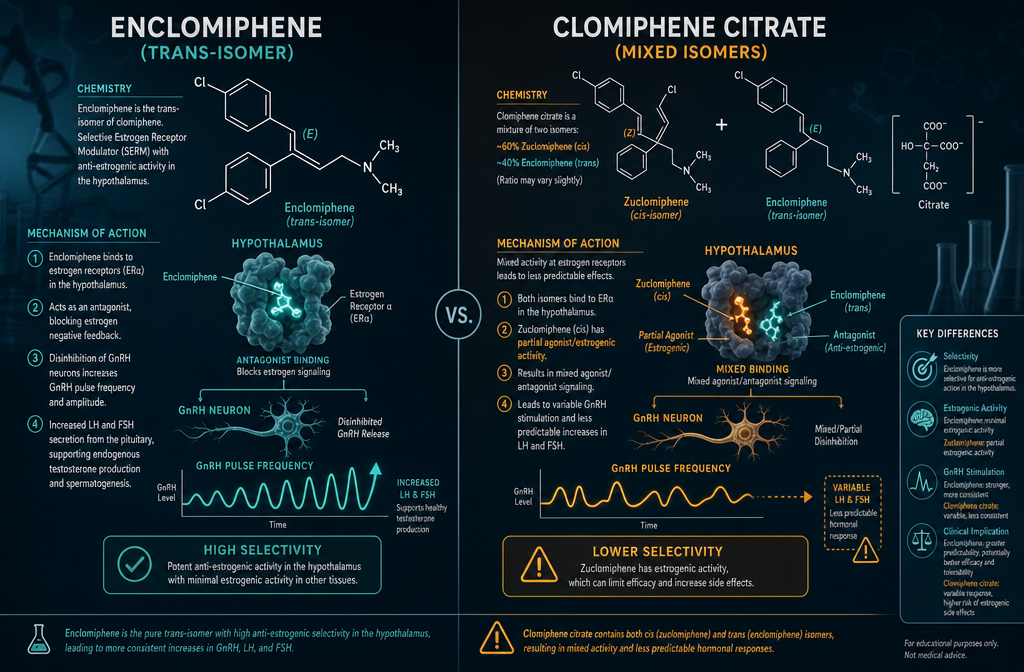
- Clomiphene is a mixture of two isomers; enclomiphene is the isolated trans-isomer responsible for anti-estrogenic, testosterone-stimulating activity.
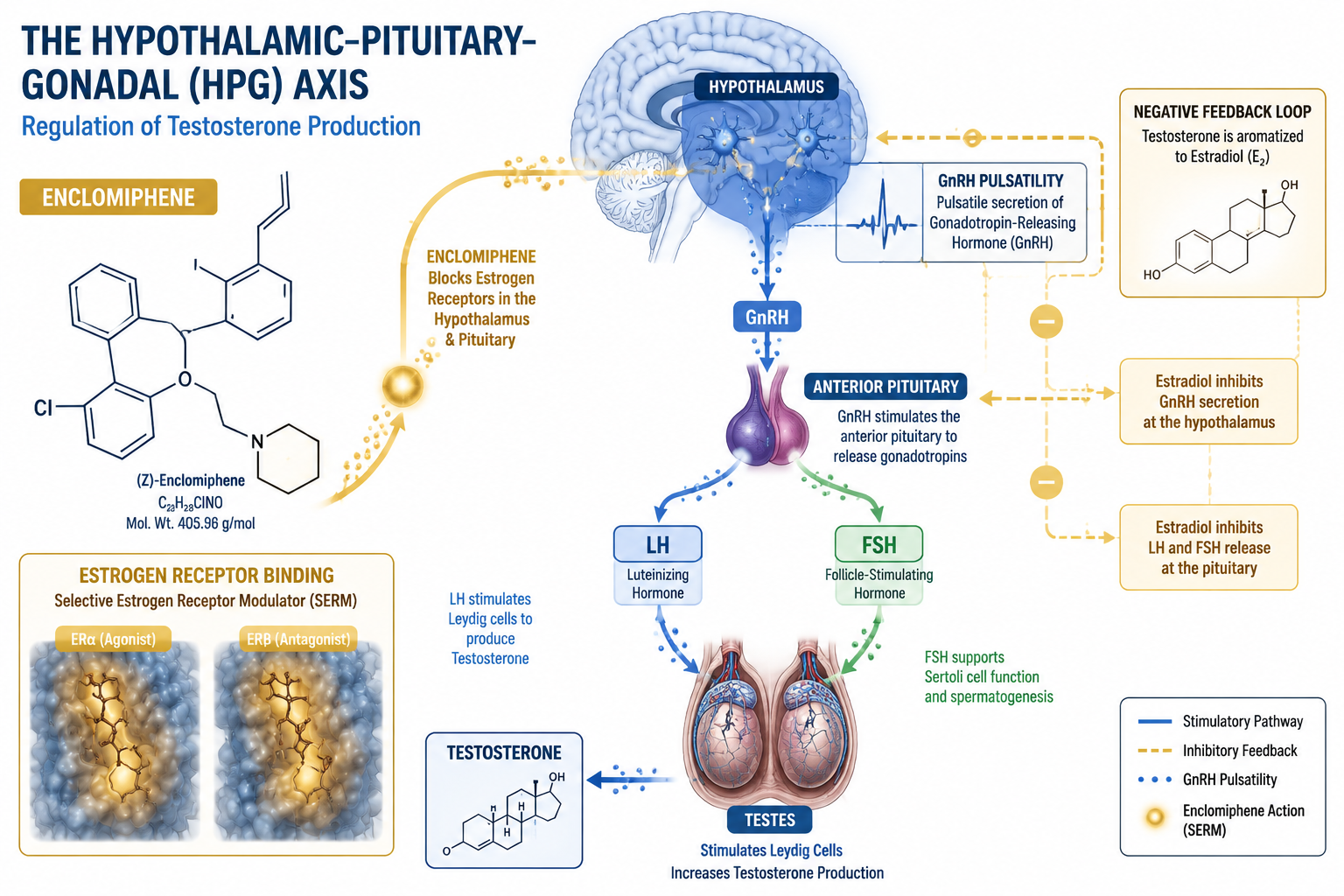
- Both compounds block estrogen receptors in the hypothalamus, triggering GnRH release and downstream LH/FSH stimulation.
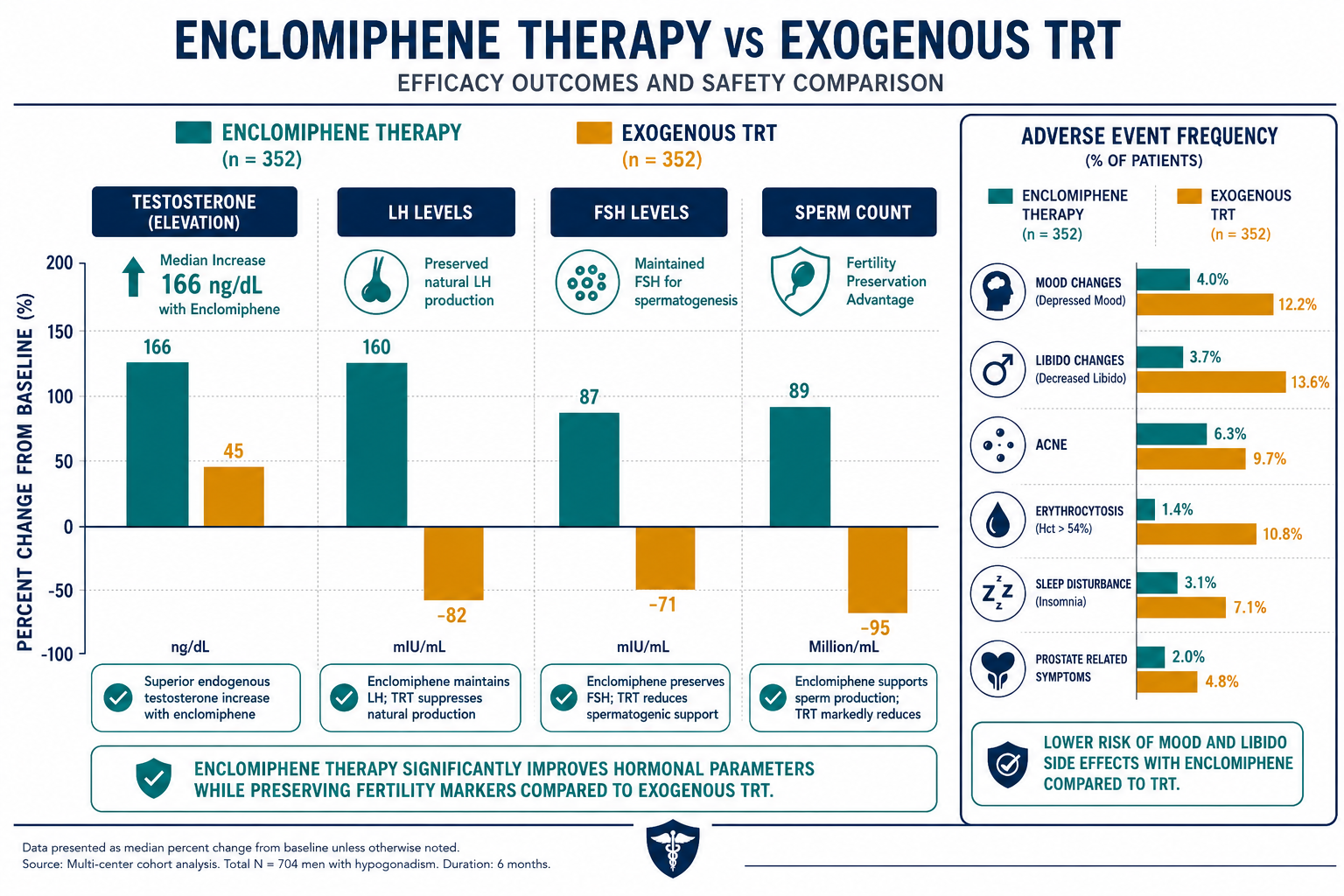
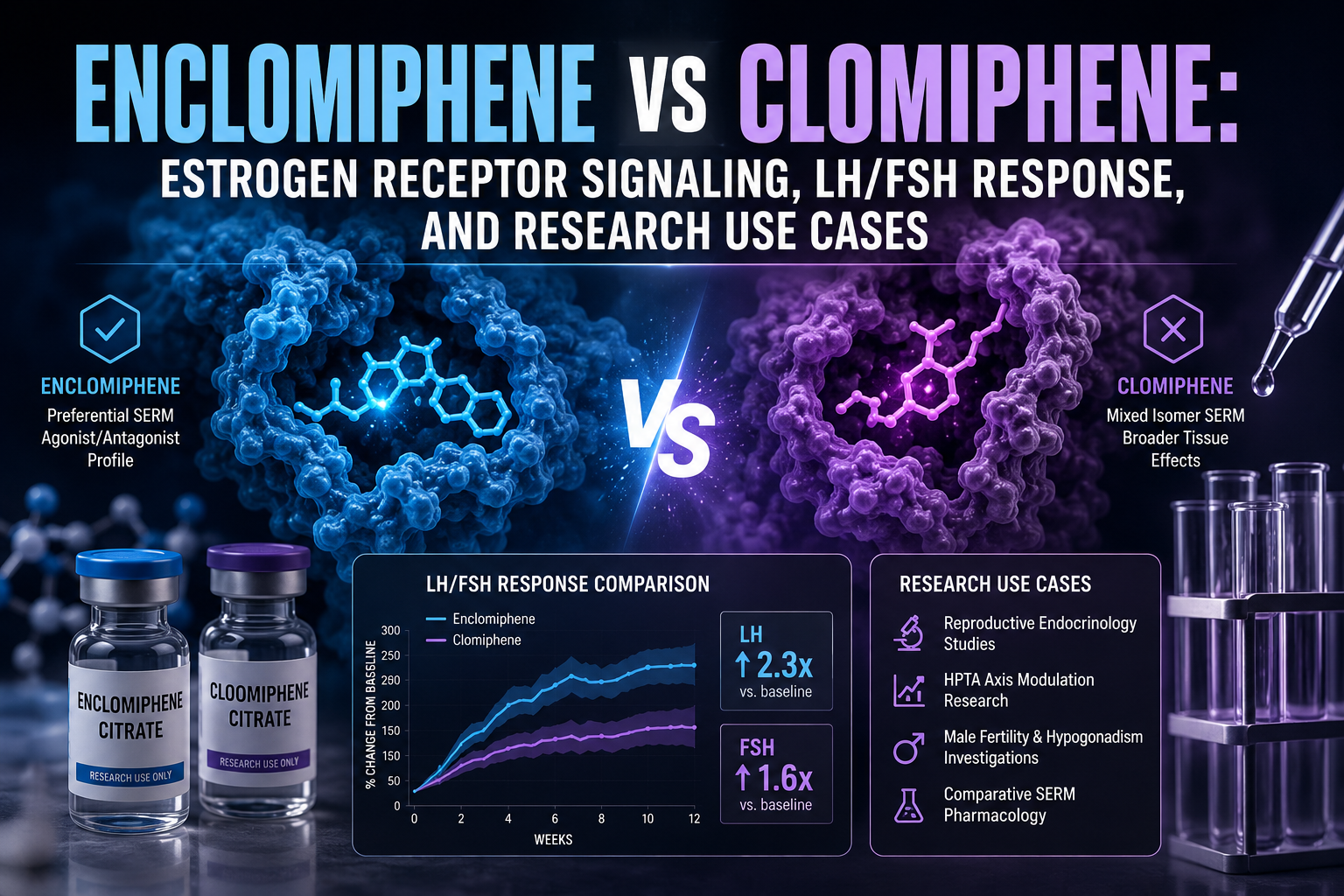
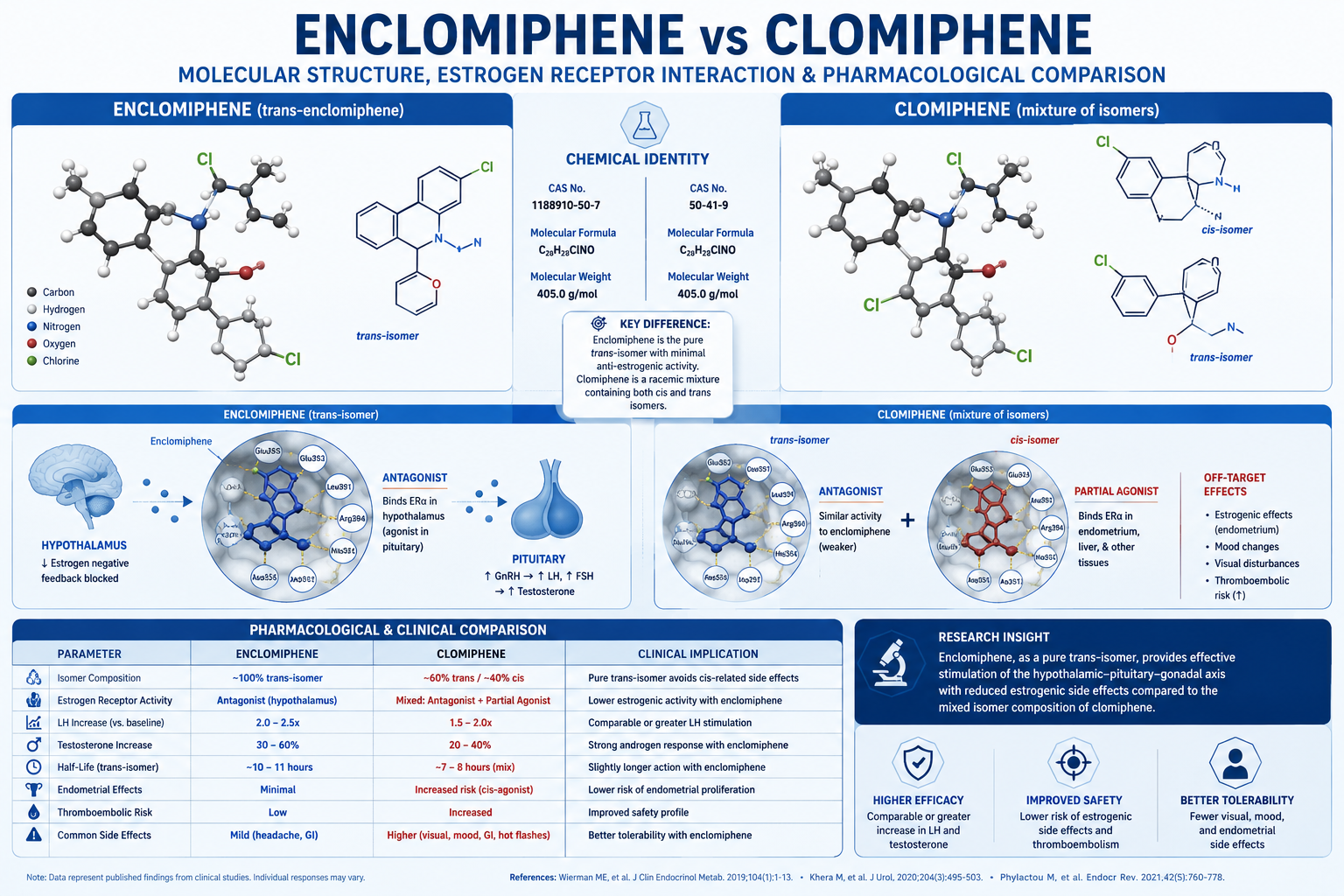
- Enclomiphene produces a greater median testosterone increase (166 ng/dL vs. 98 ng/dL) with a more favorable side effect profile.
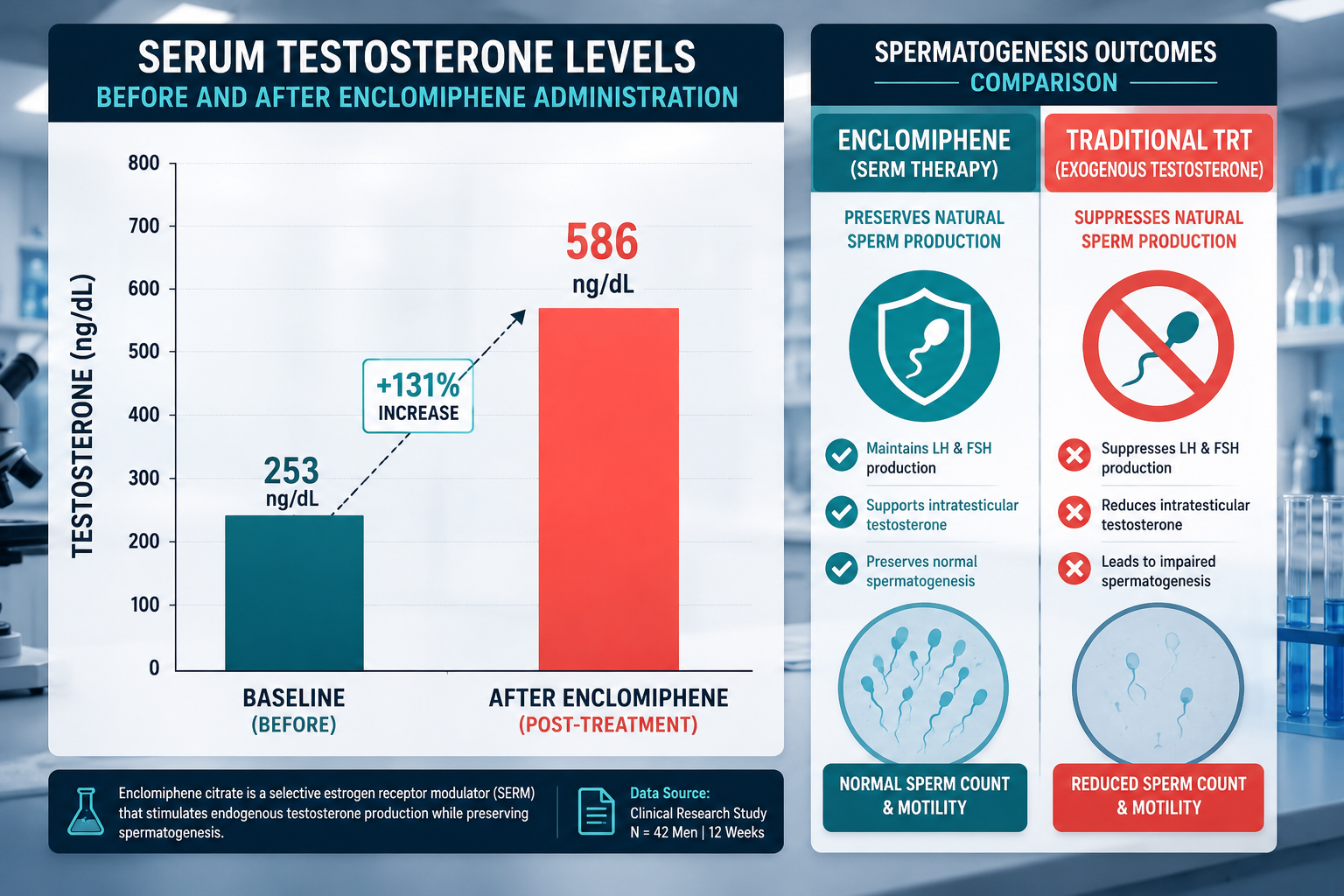
- Unlike exogenous testosterone therapy, both compounds preserve the hypothalamic-pituitary-gonadal (HPG) axis and support fertility.
- Enclomiphene is not FDA-approved as a standalone agent but is available through compounding pharmacies and is actively studied for secondary hypogonadism.
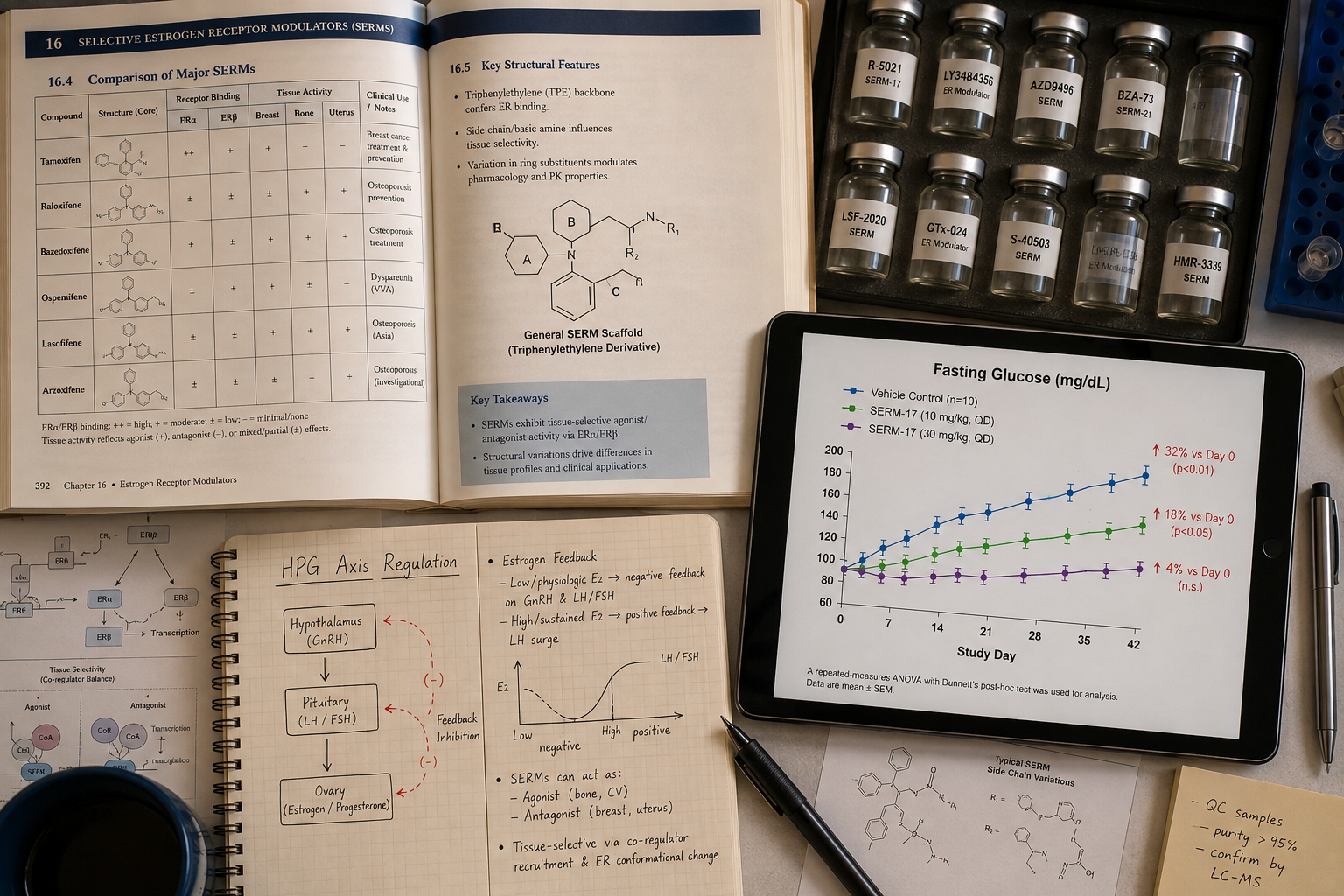
How Estrogen Receptor Signaling Differs Between the Two Compounds
Clomiphene citrate is not a single molecule. It is a racemic mixture composed of approximately 62% zuclomiphene (the cis-isomer) and 38% enclomiphene (the trans-isomer). These two isomers behave very differently at the estrogen receptor level.
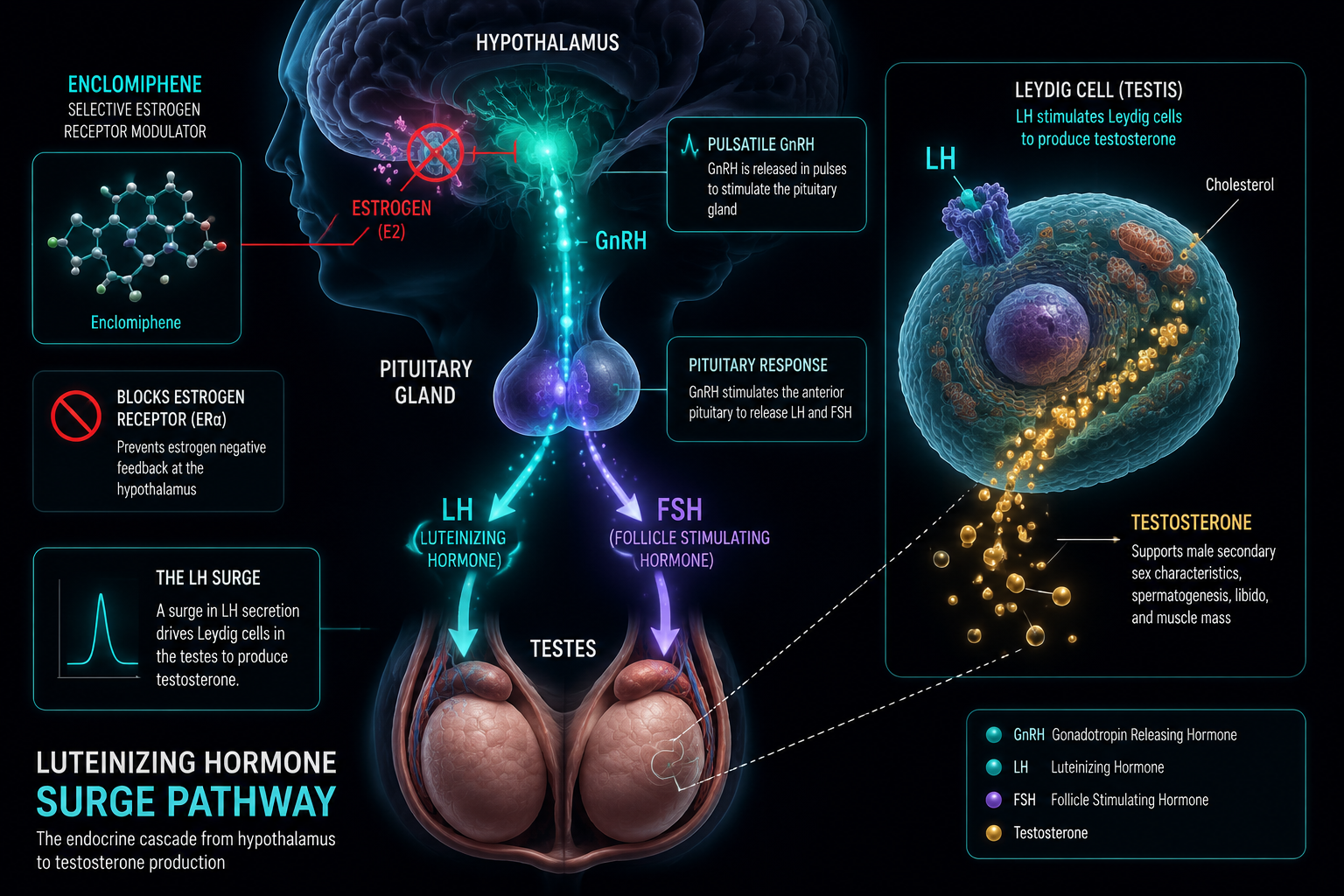
Enclomiphene acts as a pure estrogen receptor antagonist in the hypothalamus. By occupying estrogen receptors without activating them, it removes the negative feedback signal that estrogen normally sends to the brain. The hypothalamus responds by increasing gonadotropin-releasing hormone (GnRH) pulse frequency.
Zuclomiphene, in contrast, carries weak estrogenic activity and has a significantly longer half-life. It can linger in circulation for weeks, contributing to the mood changes, visual disturbances, and libido complaints that some users associate with clomiphene therapy.
"Isolating the active isomer removes the pharmacological noise introduced by zuclomiphene, giving researchers a cleaner signal at the receptor level."
This distinction is central to understanding the enclomiphene vs clomiphene estrogen receptor signaling debate. When the two isomers are separated, the mechanism becomes more predictable and the side effect profile narrows considerably.
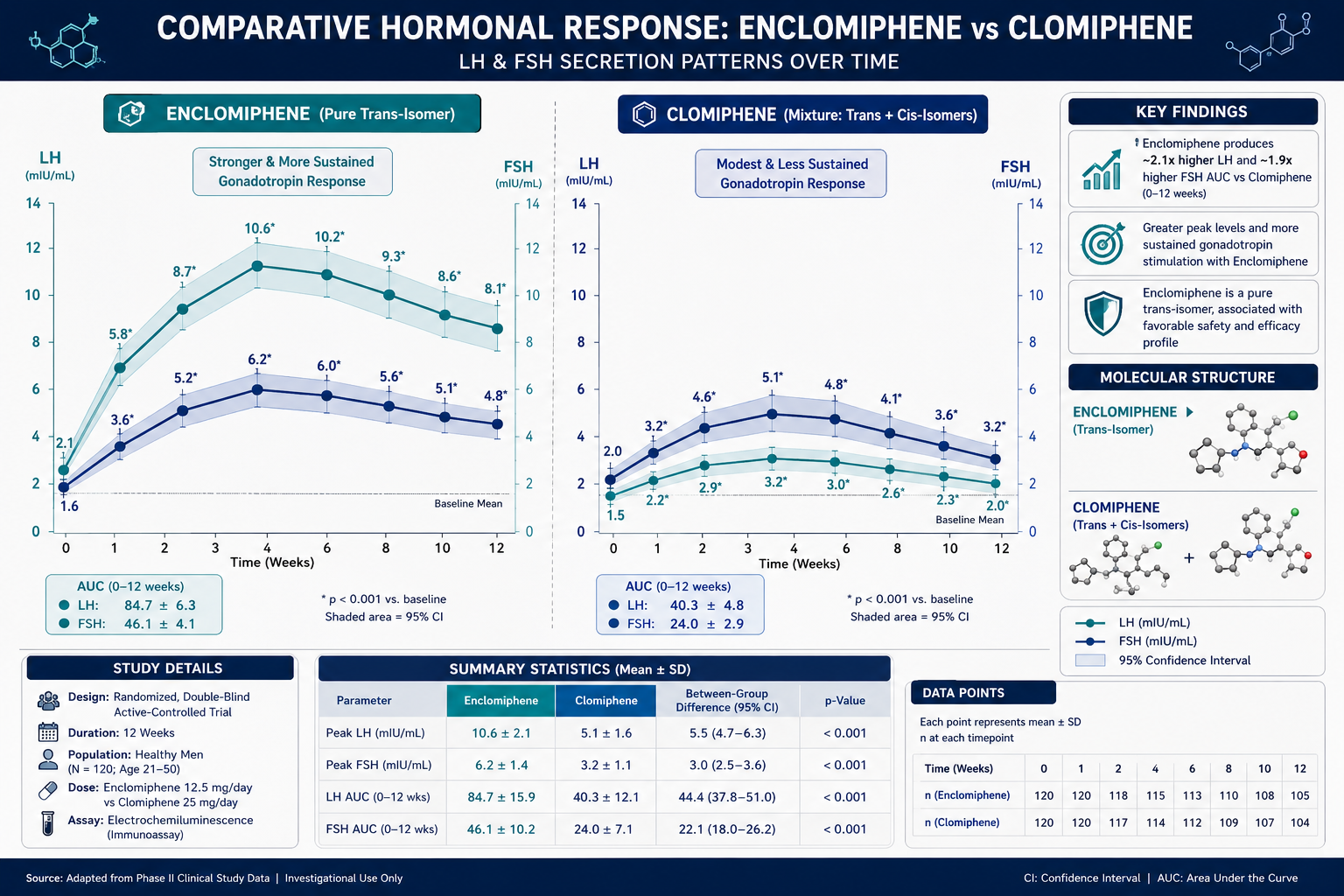
LH/FSH Response and Hormonal Outcomes: What the Data Show
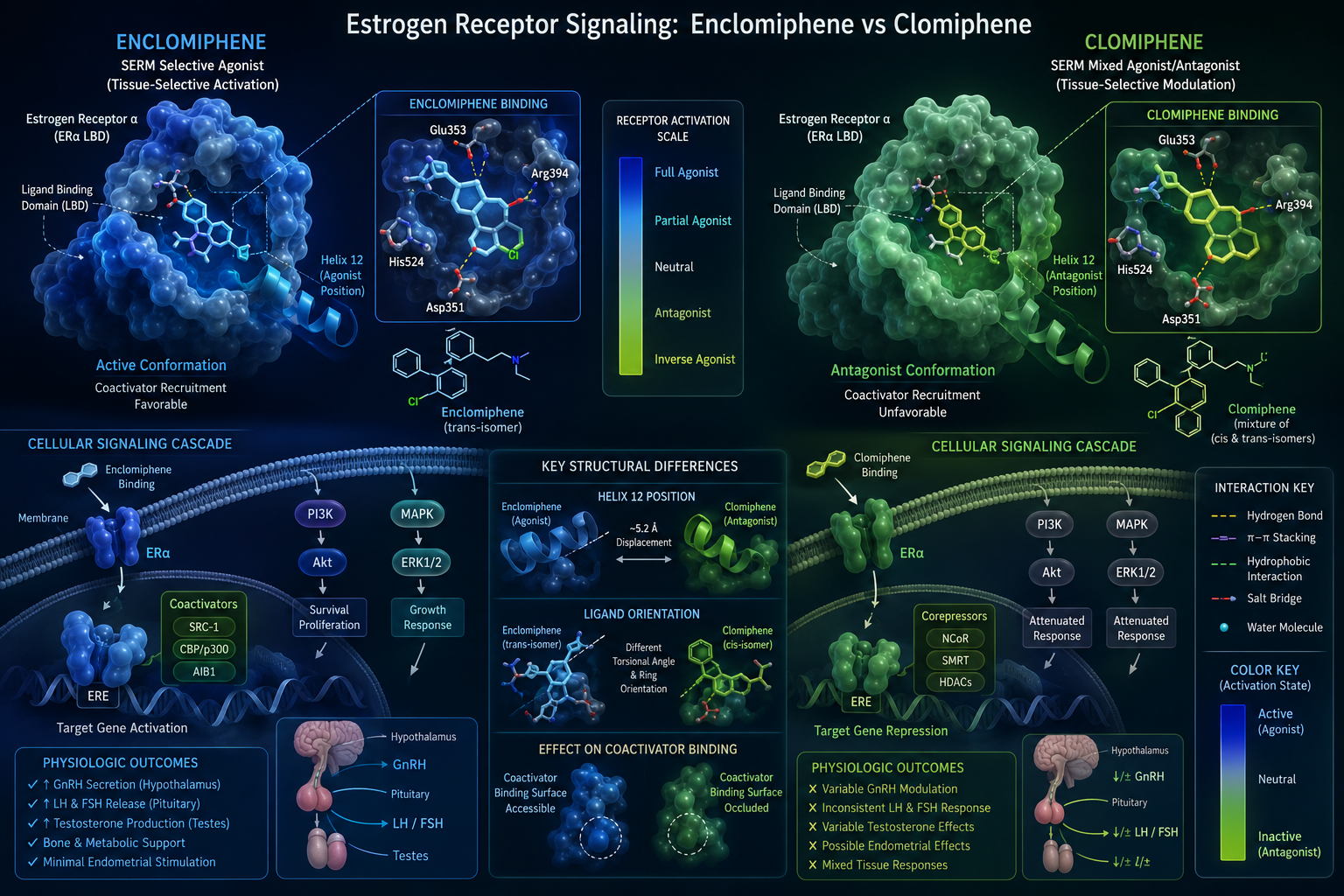
Both compounds stimulate the pituitary gland through the same upstream pathway: hypothalamic GnRH release drives luteinizing hormone (LH) and follicle-stimulating hormone (FSH) secretion, which in turn signals the testes to produce testosterone. The difference lies in the magnitude and cleanliness of that signal.
A retrospective study comparing 66 patients found that enclomiphene produced a median testosterone increase of 166 ng/dL, compared to 98 ng/dL with clomiphene. Enclomiphene also resulted in a statistically lower rise in estradiol and fewer adverse effects including reduced libido, low energy, and mood disturbances.
A separate analysis of 72 patients on enclomiphene and 861 on clomiphene over 12 months found both groups achieved significant increases in testosterone, estradiol, FSH, and LH — with no statistically significant difference between the two therapies at the population level. This suggests enclomiphene is a clinically viable alternative, not merely a theoretical upgrade.
Enclomiphene vs Clomiphene: Key Hormonal Comparison
| Parameter | Clomiphene | Enclomiphene |
|---|---|---|
| Median testosterone increase | ~98 ng/dL | ~166 ng/dL |
| Estradiol increase | Higher | Lower |
| LH/FSH stimulation | Yes | Yes |
| Visual disturbance risk | Present (zuclomiphene) | Minimal |
| Oral bioavailability | Yes | Yes |
| Half-life concern | Zuclomiphene accumulates | Short, clean clearance |
Phase III clinical trials for enclomiphene (marketed as Androxal) showed a mean testosterone increase from 232 to 525 ng/dL at a 12.5 mg/day dosage, supporting its potency as a standalone HPG axis stimulator.
For researchers exploring the GH axis alongside gonadotropin signaling, resources like the CJC-IPA GH axis research overview provide useful context on how different endocrine axes interact in research models.
Research Use Cases: Secondary Hypogonadism, Fertility, and Beyond
The primary research application for both compounds centers on secondary hypogonadism — a condition where the testes are functional but the HPG axis fails to send adequate stimulation. Unlike primary hypogonadism, this form responds well to upstream signaling interventions.
Fertility Preservation
Exogenous testosterone therapy suppresses spermatogenesis by shutting down endogenous LH and FSH. Both enclomiphene and clomiphene avoid this problem by stimulating natural production rather than replacing it. Enclomiphene is increasingly studied as a preferred option for men with secondary hypogonadism who wish to preserve sperm production.
Comparison with hCG in Research Protocols
Human chorionic gonadotropin (hCG) is another compound used to support fertility during testosterone replacement. The key differences in research context:
- Enclomiphene acts at the pituitary level, stimulates both LH and FSH, is taken orally, and has minimal estradiol impact.
- hCG acts directly on testicular Leydig cells, requires injection, and can elevate estradiol.
This distinction matters when designing protocols that target specific nodes of the HPG axis.
Metabolic and Body Composition Research Intersections
Testosterone levels intersect with body composition, metabolic rate, and mitochondrial function. Researchers studying these connections may find value in reviewing related work on MOTS-c and mitochondrial longevity research or TESA body composition research themes, which explore adjacent endocrine and metabolic pathways.
For those examining peptide-based approaches to recovery and tissue biology, the recovery and tissue biology overview provides relevant mechanistic context. Similarly, researchers interested in multi-pathway signaling models may find the KLOW blend multipathway research a useful reference point for understanding how compounds interact across systems.
Enclomiphene vs clomiphene: estrogen receptor signaling, LH/FSH response, and research use cases is a topic that also connects to broader questions about how serms interact with metabolic peptides — a growing area of interest in 2026 research literature. Those exploring peptide synergies in endocrine research can also reference the SLU-PP-332 metabolic research overview for complementary data on receptor-level signaling.
Conclusion
The comparison between enclomiphene and clomiphene is fundamentally a story about pharmacological precision. Clomiphene delivers its effects through a mixture of isomers with competing receptor activities. Enclomiphene isolates the trans-isomer responsible for clean hypothalamic estrogen receptor blockade, producing stronger LH/FSH stimulation, a larger testosterone increase, and a narrower side effect profile.
Actionable next steps for researchers and clinicians:
- When reviewing HPG axis studies, distinguish whether the protocol used racemic clomiphene or isolated enclomiphene — the distinction changes interpretation of receptor-level data.
- For fertility-preserving protocols, enclomiphene's dual LH/FSH stimulation makes it a mechanistically superior candidate compared to hCG in oral-administration models.
- Cross-reference enclomiphene data with adjacent endocrine research, including metabolic peptide work, to build a more complete picture of hormonal axis interactions.
- Consult compounding pharmacy resources and current regulatory guidance, as enclomiphene's legal status as a non-FDA-approved standalone agent affects study design and sourcing decisions.
The science is clear: understanding the isomer distinction is not a minor detail — it is the foundation of accurate hormone-axis research language.