CJC-1295 With Ipamorelin: Why Researchers Pair Them, What Pulsatile GH Signaling Looks Like, and What to Measure
{"cover":"Professional landscape format (1536×1024) hero image with bold text overlay: 'CJC-1295 With Ipamorelin: Pulsatile GH Signaling Explained' in extra large 72pt white bold sans-serif font with deep shadow and semi-transparent dark overlay bar, centered upper-third composition. Background shows a dramatic close-up of a molecular double-helix structure transitioning into a glowing pituitary gland cross-section rendered in deep teal and electric blue tones, with subtle waveform graphs suggesting hormonal pulse patterns. Color palette: deep navy, teal, white accents. Magazine cover aesthetic, editorial quality, high contrast.","content":["Detailed landscape format (1536×1024) scientific illustration showing two distinct molecular receptor pathways side by side — one labeled GHRH receptor pathway glowing in blue, the other labeled GHSR ghrelin receptor pathway glowing in amber — converging at a central pituitary gland diagram. Molecular peptide chain structures of CJC-1295 and Ipamorelin float near their respective receptors. Clean white lab background with subtle grid lines, annotated arrows showing signal amplification, professional research diagram aesthetic, high contrast, editorial quality.","Detailed landscape format (1536×1024) data visualization showing a stylized oscilloscope-style waveform graph representing pulsatile GH secretion over a 24-hour period, with clearly labeled amplitude peaks marked 'Combined CJC-1295 + Ipamorelin' in teal versus a lower flatter line labeled 'Baseline' in gray. The graph sits on a dark navy background with glowing neon-teal pulse lines, subtle clock icons at the x-axis, and a secondary smaller IGF-1 rise curve in amber. Scientific infographic style, professional, high contrast, editorial quality.","Detailed landscape format (1536×1024) flat-lay laboratory bench scene photographed from directly above showing research measurement tools: a serum IGF-1 ELISA assay plate, printed GH pulse amplitude data charts, a digital caliper, a body composition DEXA scan printout, and a researcher's gloved hand annotating results with a red pen. Warm clinical white lighting, organized composition, subtle teal and navy color accents on printed materials, research laboratory aesthetic, editorial quality, high contrast."]
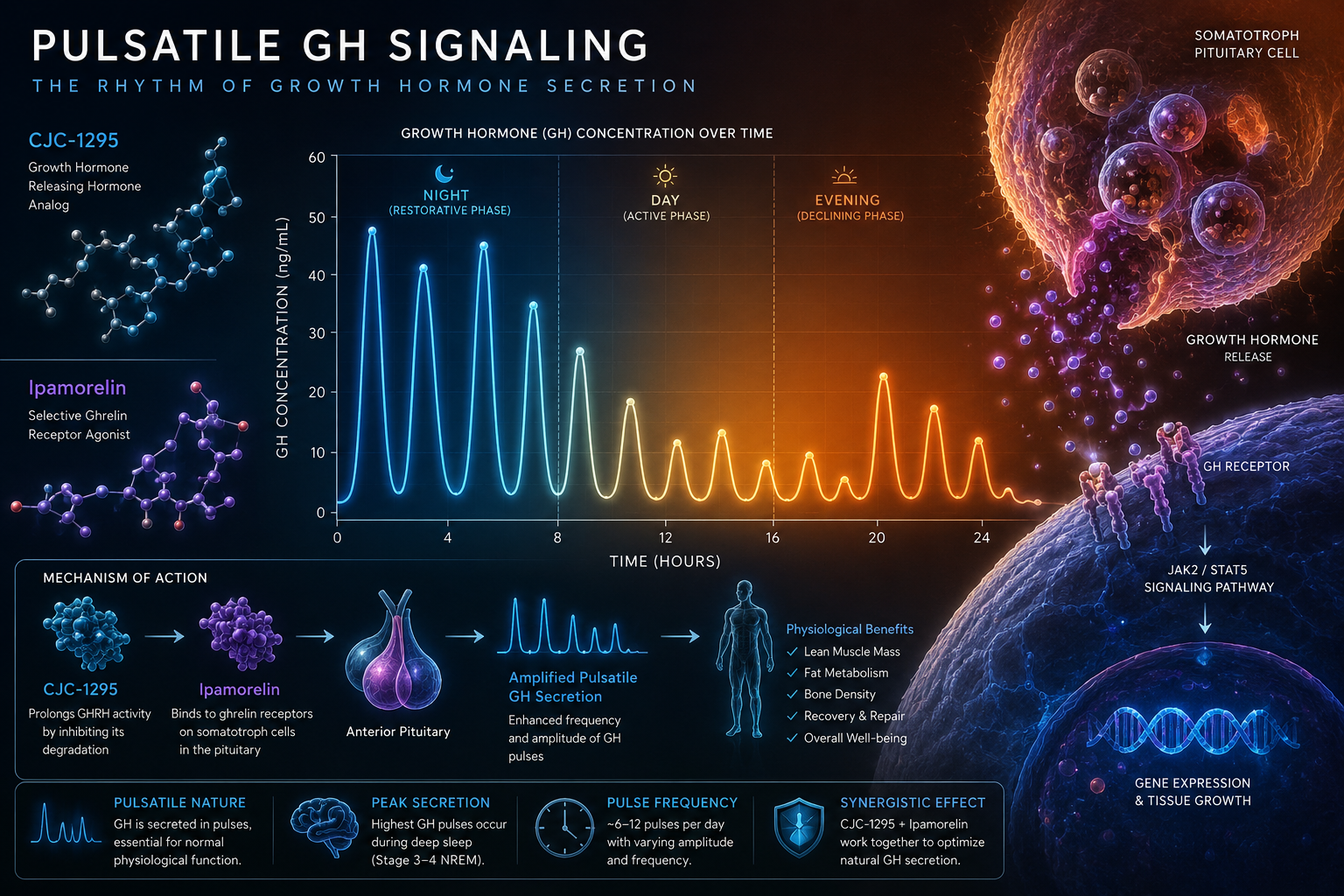
Growth hormone secretion is not continuous — it fires in discrete pulses, and that architecture matters enormously for how researchers design experiments. Understanding CJC-1295 with Ipamorelin: why researchers pair them, what pulsatile GH signaling looks like, and what to measure starts with a single insight: these two peptides activate entirely different receptor classes, and combining them produces a synergistic amplification that neither achieves alone.
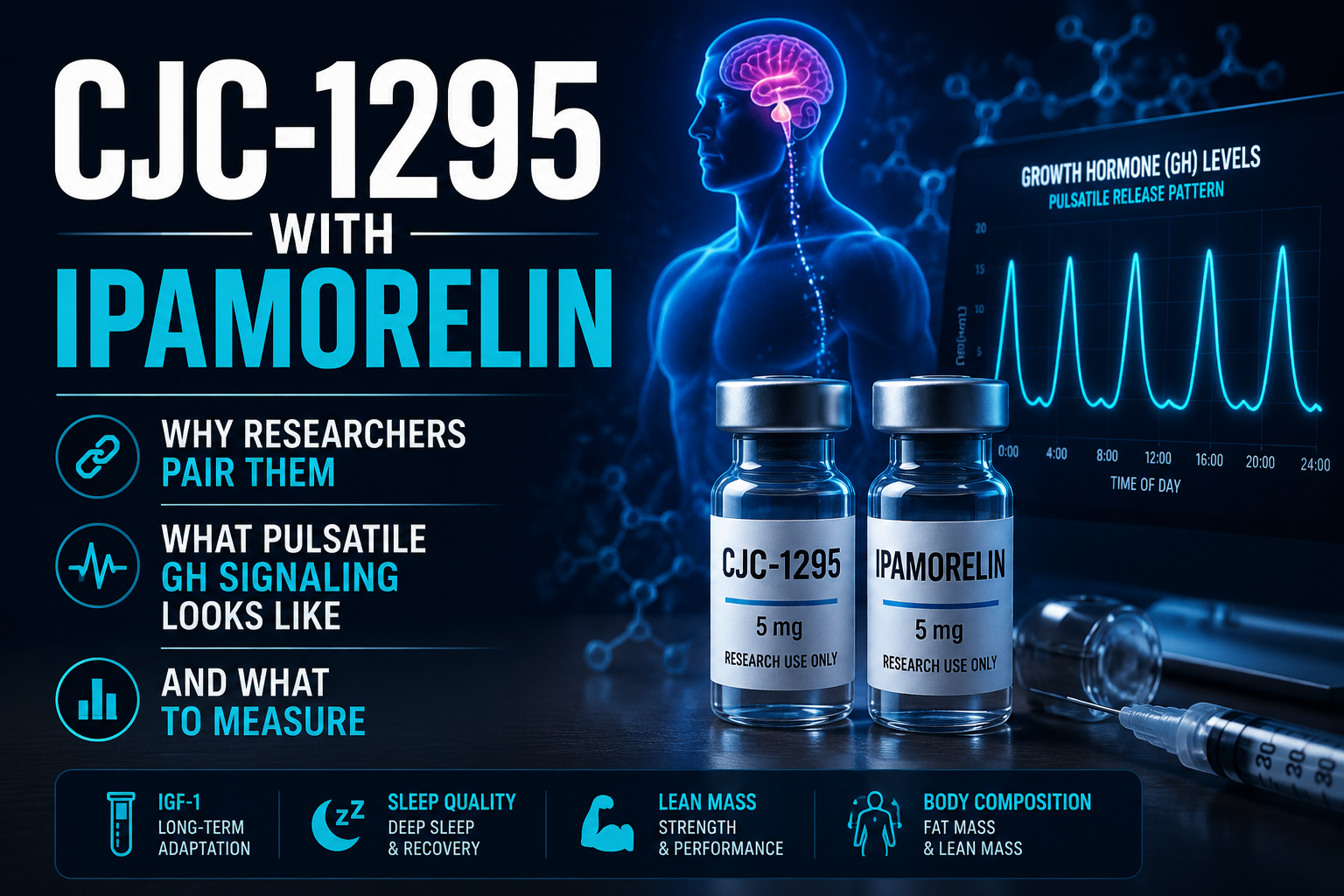
Key Takeaways
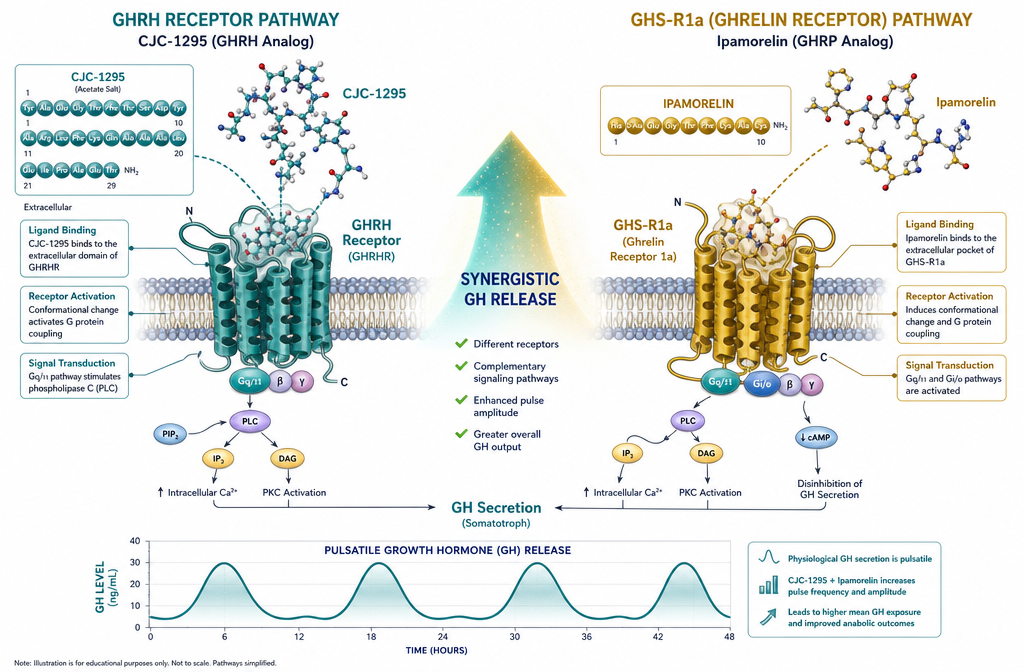
- CJC-1295 acts on GHRH receptors; Ipamorelin acts on GHSR (ghrelin) receptors — two distinct pathways.
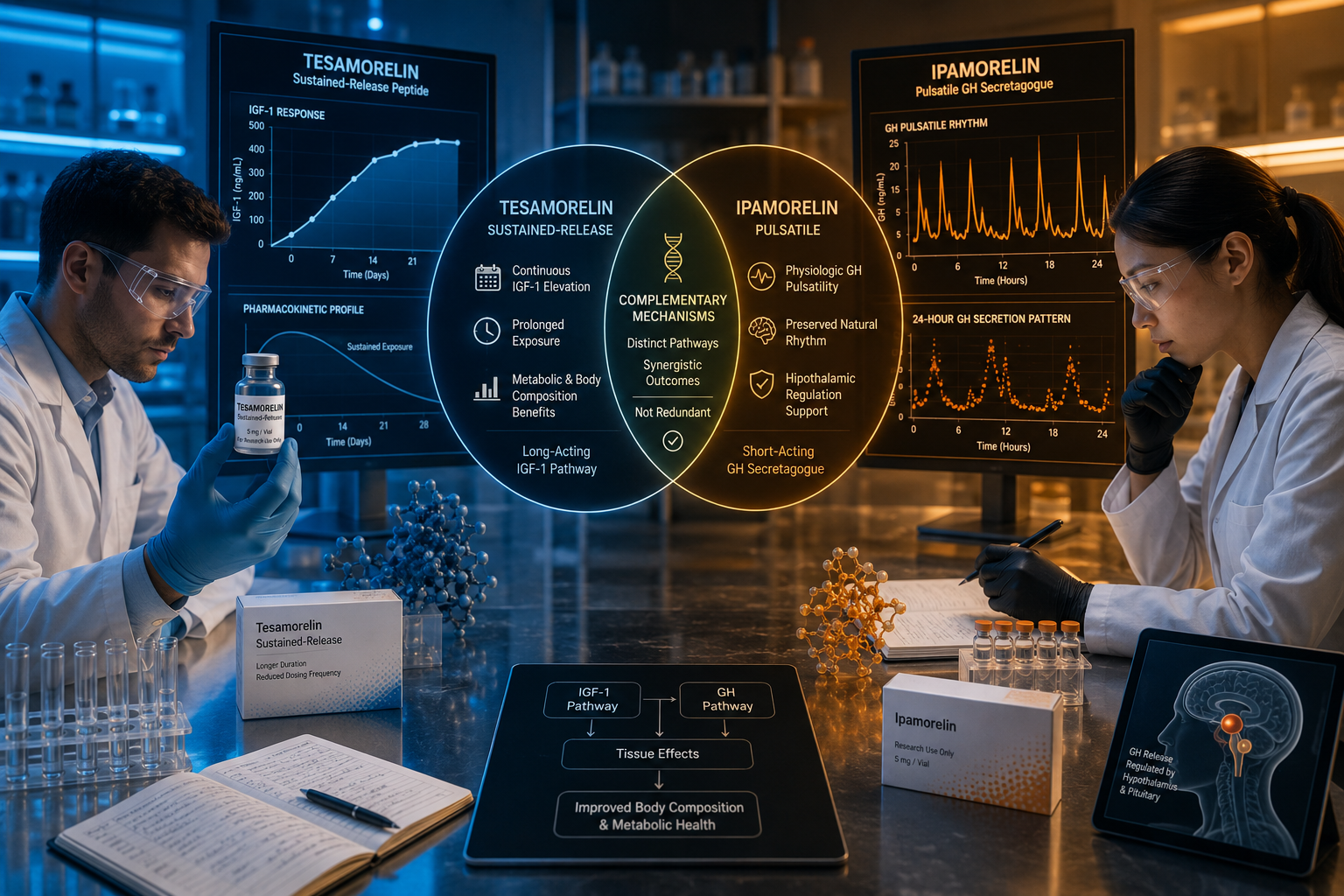
- Combining them amplifies GH pulse amplitude more than additive effects would predict.
- Pulsatile GH output preserves downstream receptor sensitivity in a way that continuous infusion does not.
- Primary research readouts are serum GH pulse amplitude, IGF-1 levels, and body composition markers.
- Regulatory status for these peptides has tightened in several jurisdictions since the mid-2020s; researchers must verify local compliance before sourcing.
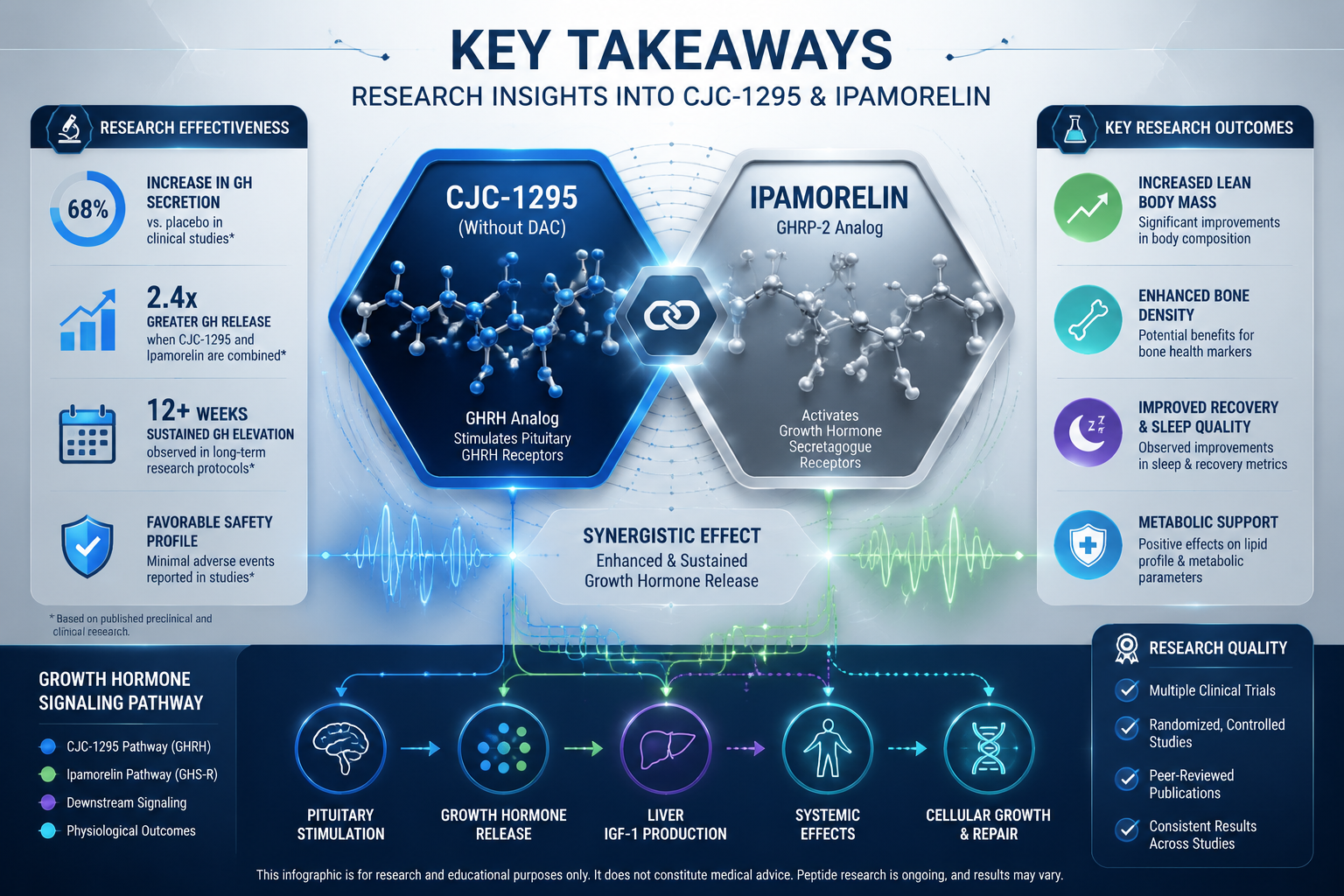
The Dual-Pathway Rationale Behind Pairing CJC-1295 With Ipamorelin
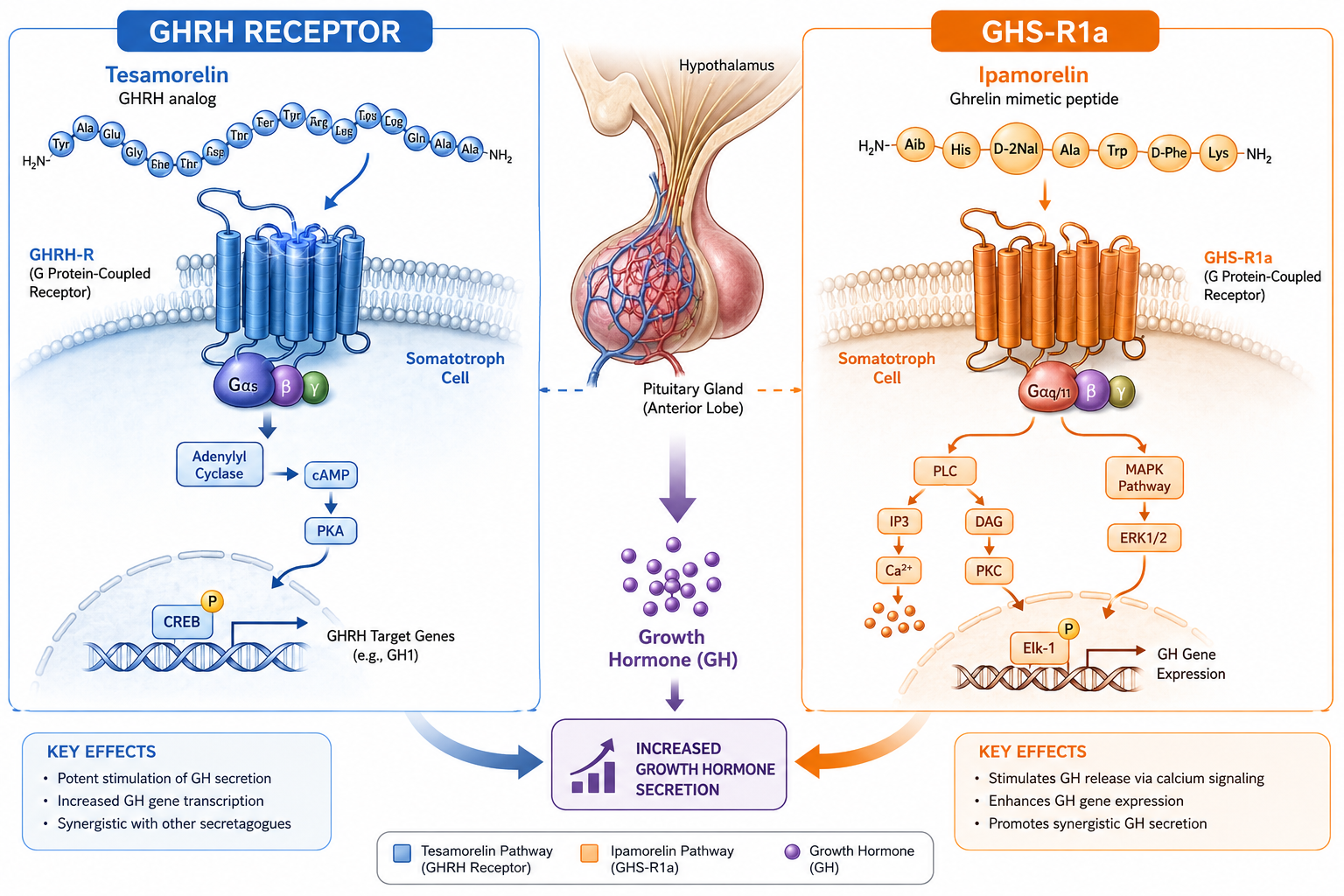
The pituitary releases growth hormone through two primary input signals. The first is growth hormone-releasing hormone (GHRH), which binds to GHRH receptors on somatotroph cells and drives GH synthesis and release. The second is ghrelin, which binds to the growth hormone secretagogue receptor (GHSR-1a) and independently stimulates GH release through a separate intracellular cascade.
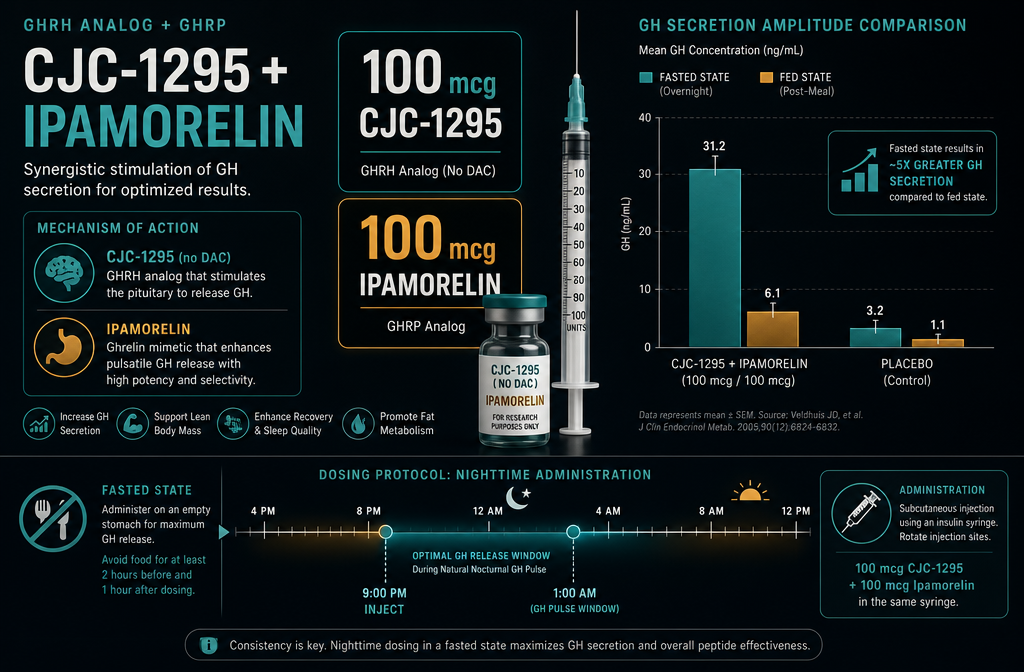
CJC-1295 is a modified GHRH analogue. The version without a Drug Affinity Complex (DAC) produces a shorter, cleaner pulse, making it the preferred form in most research designs. For a deeper look at how this analogue behaves in isolation, the CJC-1295 no-DAC research themes overview covers the mechanistic literature in detail.
Ipamorelin is a selective GHSR agonist. It is considered one of the cleaner secretagogues because it produces minimal cortisol or prolactin co-release — a significant confound in earlier ghrelin-mimetic research. The Ipamorelin muscle and fat research themes page summarizes its downstream metabolic effects.
"Two keys, one lock system" is a useful mental model: CJC-1295 primes the somatotroph cell while Ipamorelin simultaneously triggers it through a separate gate. The result is a GH pulse that is substantially larger than either peptide produces independently.
This synergistic amplification has been documented in human pharmacokinetic data for CJC-1295, where mean GH peak concentrations rose several-fold above baseline. When a GHSR agonist is added, the amplitude rises further because both intracellular pathways converge on the same exocytotic machinery.
What Pulsatile GH Signaling Looks Like in This Research Context
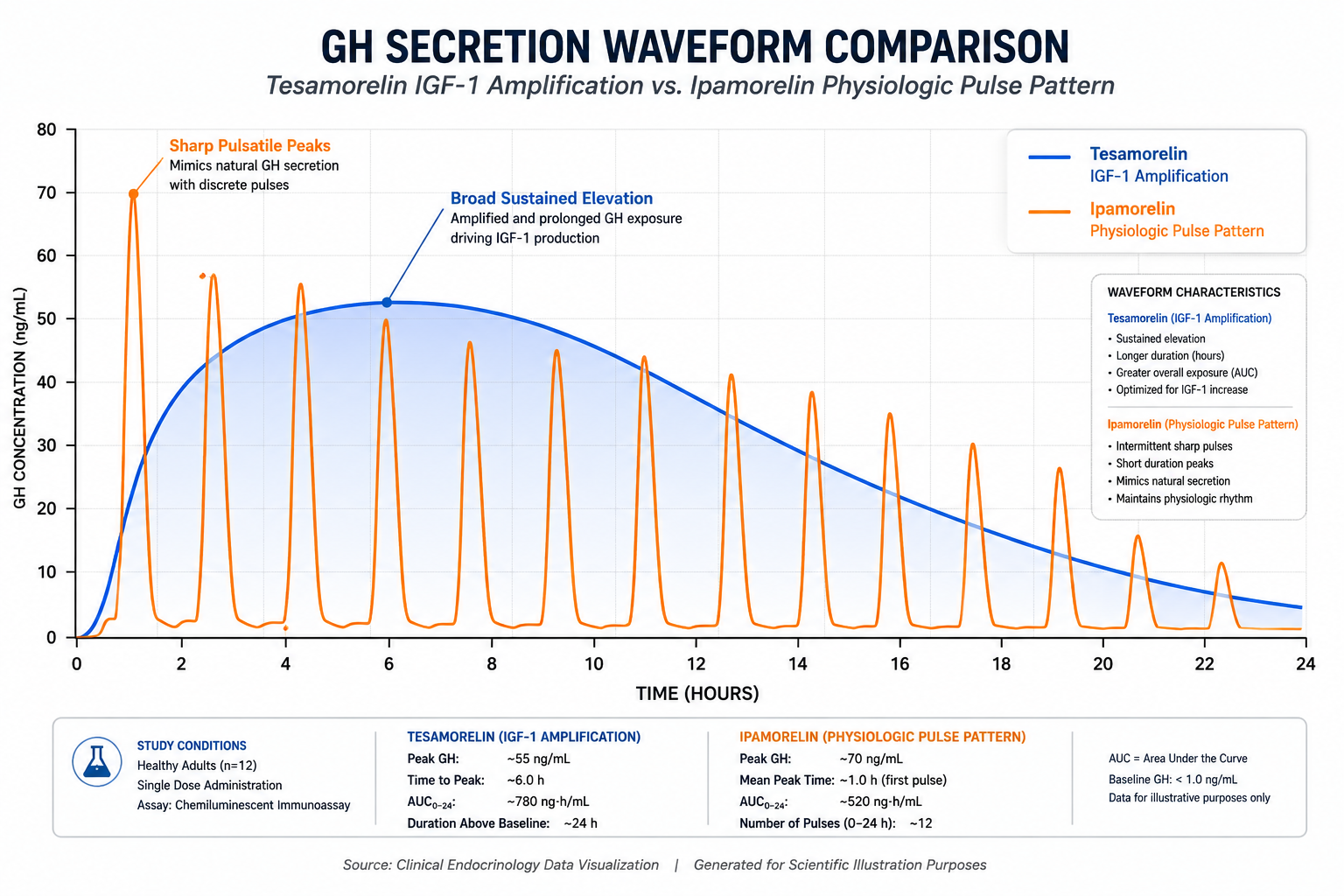
Normal physiological GH secretion occurs in roughly 6-12 pulses per 24 hours, with the largest pulse occurring during slow-wave sleep. Between pulses, serum GH falls to near-undetectable levels. This on-off pattern is not incidental — it is the mechanism that keeps GH receptors sensitive.
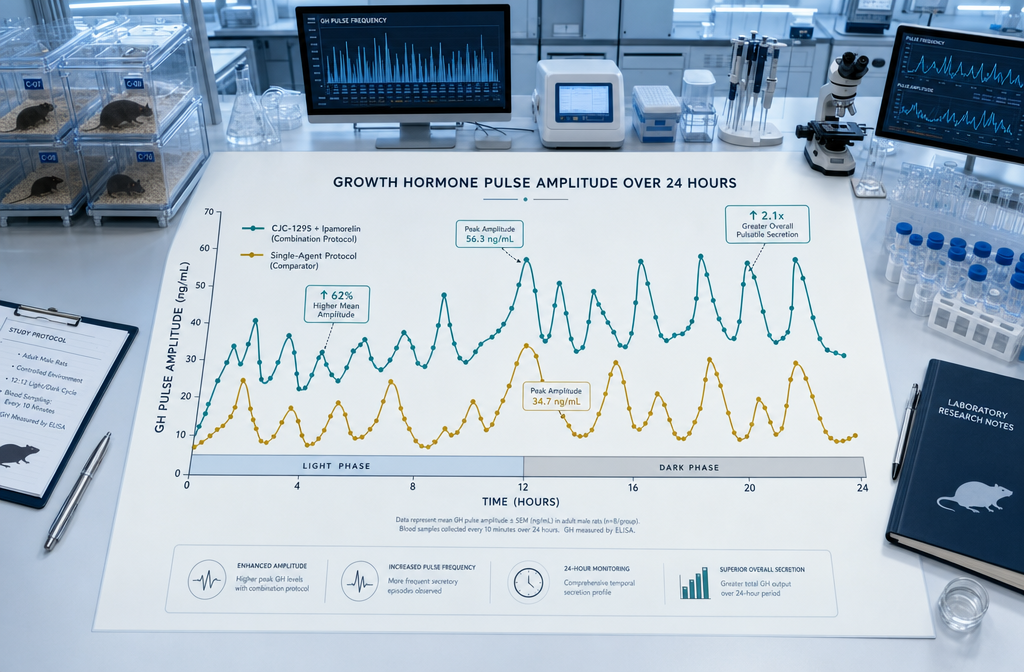
When CJC-1295 with Ipamorelin are administered together, the resulting GH pulse mimics this natural architecture rather than producing a sustained elevation. The key features researchers observe are:
- Higher peak amplitude — the combined pulse reaches concentrations that single-agent protocols rarely achieve
- Normal inter-pulse trough — GH returns toward baseline between doses, preserving receptor sensitivity
- Downstream IGF-1 rise — hepatic IGF-1 production responds to the amplified pulses, with measurable increases appearing within days to weeks of consistent dosing
This is the fundamental reason the combination is preferred over continuous GHRH infusion in research models. Sustained GH elevation causes receptor downregulation; pulsatile delivery avoids it.
For researchers considering how this combination fits within a broader GH-axis research framework, the GH axis product line overview and the CJC-IPA GH axis research page provide useful context.
What to Measure: Key Readouts for CJC-1295 With Ipamorelin Research
Selecting the right endpoints is as important as the pairing rationale itself. Researchers working with this combination in 2026 typically track the following:
| Readout | Method | Typical Timeframe |
|---|---|---|
| Serum GH pulse amplitude | Serial blood sampling + ELISA | Acute (hours post-dose) |
| Serum IGF-1 | Single fasting blood draw | 2-6 weeks of dosing |
| Lean mass / fat mass | DEXA scan | 8-16 weeks |
| Fasting glucose and insulin | Standard metabolic panel | Ongoing |
| Sleep architecture | Polysomnography or actigraphy | 4-8 weeks |
IGF-1 remains the most practical chronic marker because it integrates GH pulsatility over days rather than requiring timed serial sampling. Emerging 2025 human-oriented data suggest modest improvements in lean body mass and reductions in visceral fat with combined secretagogue protocols, though evidence quality remains low-to-moderate and most studies are small.
Sleep-stage data are increasingly included in research designs because GH pulse amplitude during slow-wave sleep is a sensitive indicator of somatotroph responsiveness. Blunted nocturnal GH is one of the earliest measurable signs of somatopause, making it a meaningful endpoint in aging-focused studies.
For researchers planning assay selection and sourcing logistics, the CJC-1295 Ipamorelin assay planning and sourcing checklist is a practical starting resource. Those evaluating dosing frameworks can also review the Sermorelin, Ipamorelin, and CJC-1295 dosage research guide for comparative context.
Regulatory and Safety Considerations in 2026
Regulatory scrutiny of peptide secretagogues has intensified. Several major jurisdictions, including the United States and Australia, have moved to restrict or reclassify compounded GHRH analogues and GHSRs since the mid-2020s. Researchers must confirm current local regulatory status before sourcing. Purity verification through third-party analytical testing — including HPLC and mass spectrometry — is a non-negotiable step in any credible research protocol.
Conclusion
The logic behind pairing CJC-1295 with Ipamorelin is mechanistically sound: two distinct receptor pathways converge to produce a GH pulse that is larger, cleaner, and more physiologically faithful than either agent generates alone. For researchers, the actionable next steps are straightforward. First, confirm that the research design requires pulsatile GH amplification rather than sustained elevation. Second, select the right biomarkers — IGF-1 for chronic tracking, serial GH sampling for acute pharmacokinetic work, and body composition endpoints for longer studies. Third, verify peptide purity and local regulatory compliance before any experiment begins. Researchers interested in how this combination compares to other secretagogue options can explore the Tesamorelin vs Ipamorelin comparison or review CJC-1295 plus Ipamorelin combination research for additional design considerations. The science is compelling; the rigor of execution determines whether the data are meaningful.