Peptides and Polypeptides in Endocrine Research: Linking Estrogen Receptor Signaling to Enclomiphene and GLP-3 Retatrutide Models
Fewer than three decades ago, the estrogen receptor was considered a single, well-understood target. Today, researchers recognize at least three distinct receptor subtypes — ERalpha, ERbeta, and the G protein-coupled estrogen receptor (GPER) — each capable of driving separate downstream cascades. That complexity is precisely why the field of peptides and polypeptides in endocrine research: linking estrogen receptor signaling to enclomiphene and GLP-3 retatrutide models has become one of the most active areas of translational biology in 2026.
Key Takeaways
- Estrogen receptors are not monolithic; GPER mediates rapid non-genomic signaling distinct from classical nuclear ER pathways.
- Enclomiphene acts as a selective estrogen receptor modulator (serm) at the hypothalamus, restoring endogenous testosterone without suppressing the HPG axis.
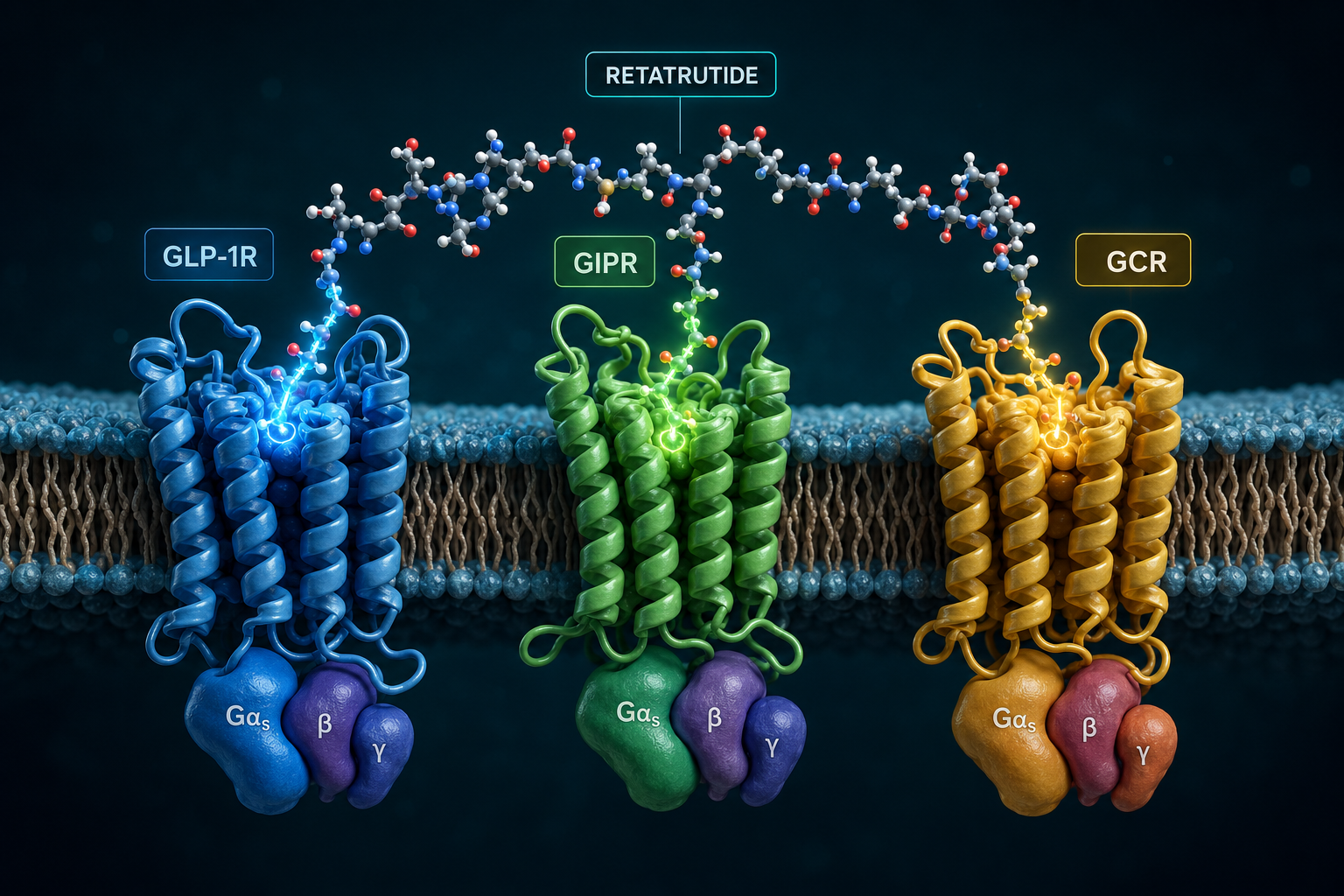
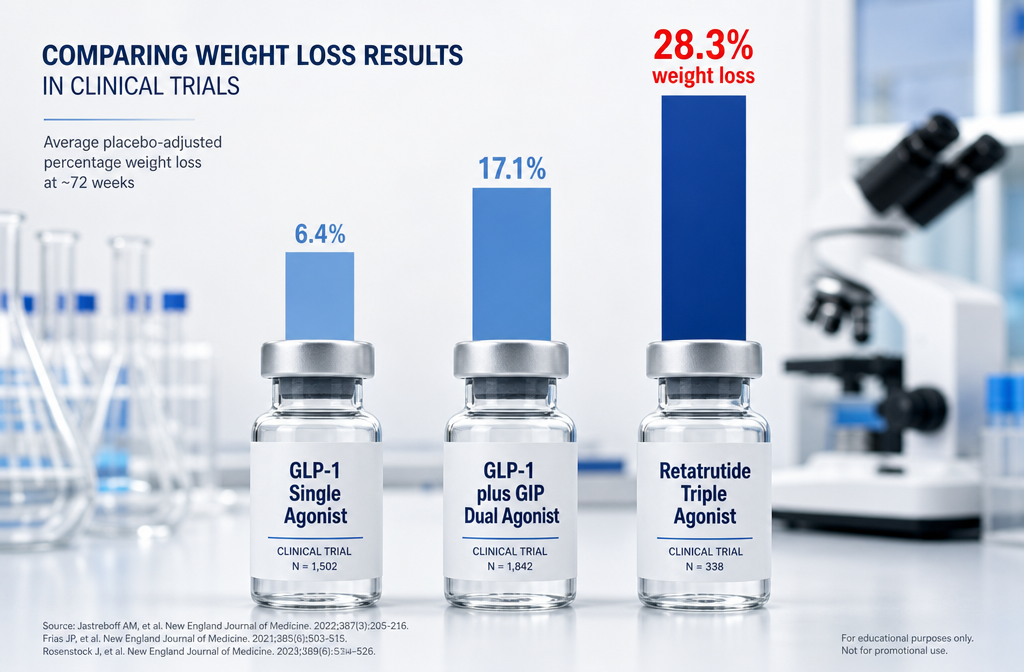
- Retatrutide is a synthetic 39-amino-acid polypeptide that simultaneously activates GLP-1R, GIPR, and GCGR — a triple-agonist profile unmatched by earlier metabolic peptides.
- Cross-talk between peptide growth factors and estrogen receptor systems creates layered regulatory complexity relevant to drug design.
- Both enclomiphene and retatrutide illustrate how modern endocrine research moves beyond single-target pharmacology toward systems-level modulation.
Estrogen Receptor Biology: The Foundation for Peptide Cross-Talk
Classical endocrinology framed estrogen signaling as a nuclear event: ligand binds receptor, receptor binds DNA, gene transcription changes. GPER challenged that model by demonstrating that estrogens also trigger acute, non-genomic responses through G protein-coupled pathways — activating cAMP, mobilizing intracellular calcium, and phosphorylating kinase cascades within minutes rather than hours.
This dual-mode signaling matters for peptide researchers because peptide growth factors and estrogen receptors actively cross-talk. Insulin-like growth factors, epidermal growth factor, and related polypeptides can transactivate ERalpha without a classical estrogen ligand. Conversely, estrogen receptor activity can sensitize cells to peptide growth factor signals. Understanding this bidirectional regulation is foundational to interpreting how newer research compounds interact with hormonal physiology.
"Estrogen receptor cross-talk with peptide signaling systems is not a side effect — it is a core feature of endocrine architecture."
For researchers exploring metabolic and longevity-related peptides, resources such as the MOTS-C metabolic flexibility research overview and the GIP receptor importance guide provide useful context on how peptide signals intersect with broader hormonal networks.
Enclomiphene as a Case Study in Receptor-Selective Endocrine Modulation
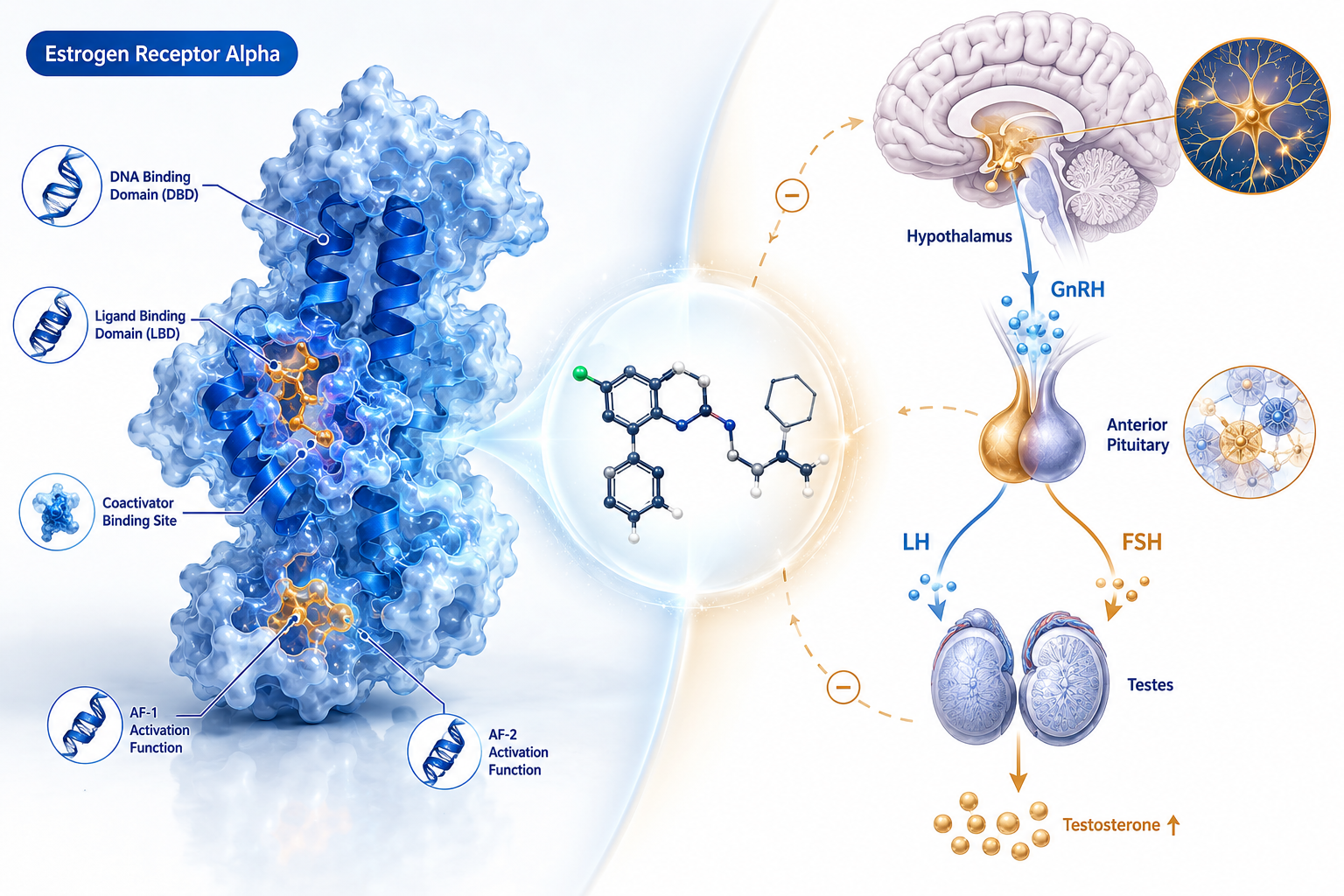
Enclomiphene is the trans-isomer of clomiphene and functions as a selective estrogen receptor modulator (serm). Its primary site of action is the hypothalamus and pituitary, where it blocks estrogen receptors and removes the negative-feedback brake on gonadotropin-releasing hormone (GnRH) pulsatility. The result is a cascade: GnRH rises, LH and FSH secretion increases, and the testes respond with elevated testosterone production.
What makes enclomiphene scientifically notable is what it preserves. Unlike exogenous testosterone, enclomiphene leaves the entire hypothalamic-pituitary-gonadal (HPG) axis intact, including its own feedback loops. This distinguishes it sharply from peptide-class HPG stimulators such as gonadorelin or kisspeptin-10, which act at different nodes in the same axis.
Pharmacokinetic profile comparison:
| Compound | Clearance | Axis Preservation |
|---|---|---|
| Enclomiphene | Days | Full HPG axis intact |
| Zuclomiphene (isomer) | Weeks | Partial, prolonged suppression risk |
| Gonadorelin (peptide) | Minutes | Pulsatile, receptor-dependent |
Enclomiphene's rapid clearance — measured in days rather than the weeks seen with its isomer zuclomiphene — makes it a cleaner pharmacological tool for research into upstream estrogen receptor blockade. For comparison, researchers studying GH-axis peptides may find the CJC-1295 and ipamorelin GH axis research a useful parallel for understanding how upstream modulation shapes downstream hormonal output.
GLP-3 Retatrutide Models and the Polypeptide Approach to Metabolic Signaling
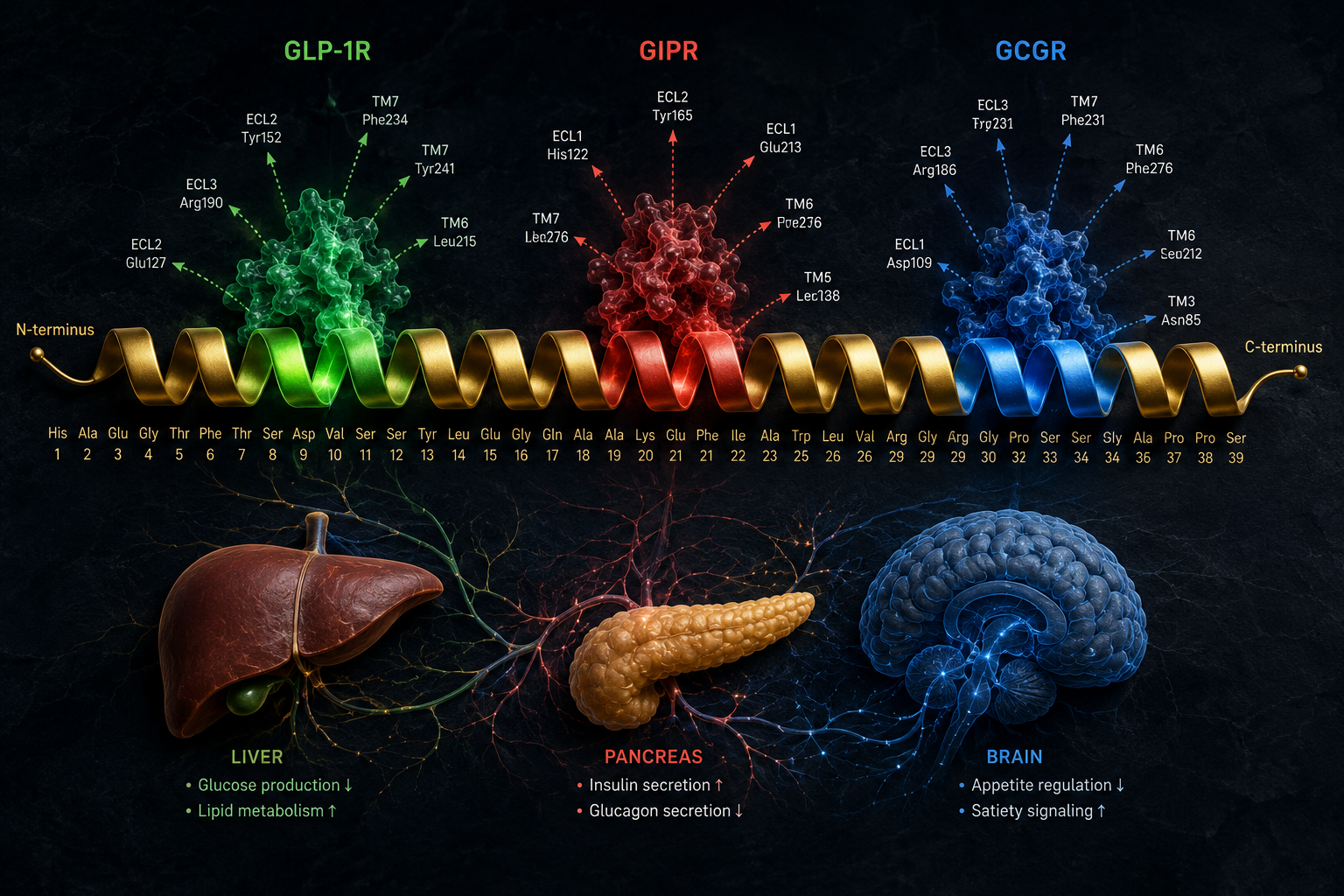
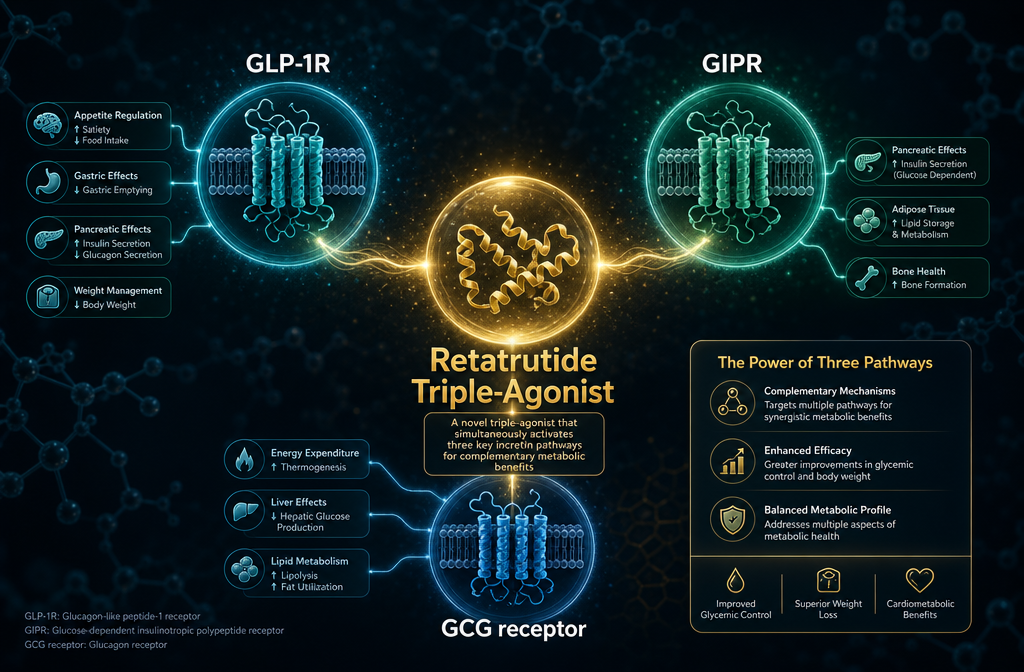
Retatrutide (LY3437943) represents a different philosophy entirely. Rather than blocking a receptor to release a suppressed axis, this synthetic 39-amino-acid polypeptide simultaneously activates three receptors: GLP-1R, GIPR, and GCGR. Cryo-EM structural studies show that retatrutide adopts a single continuous alpha-helix conformation when binding, with receptor-specific amino acid differences accounting for its differential potency at each target.
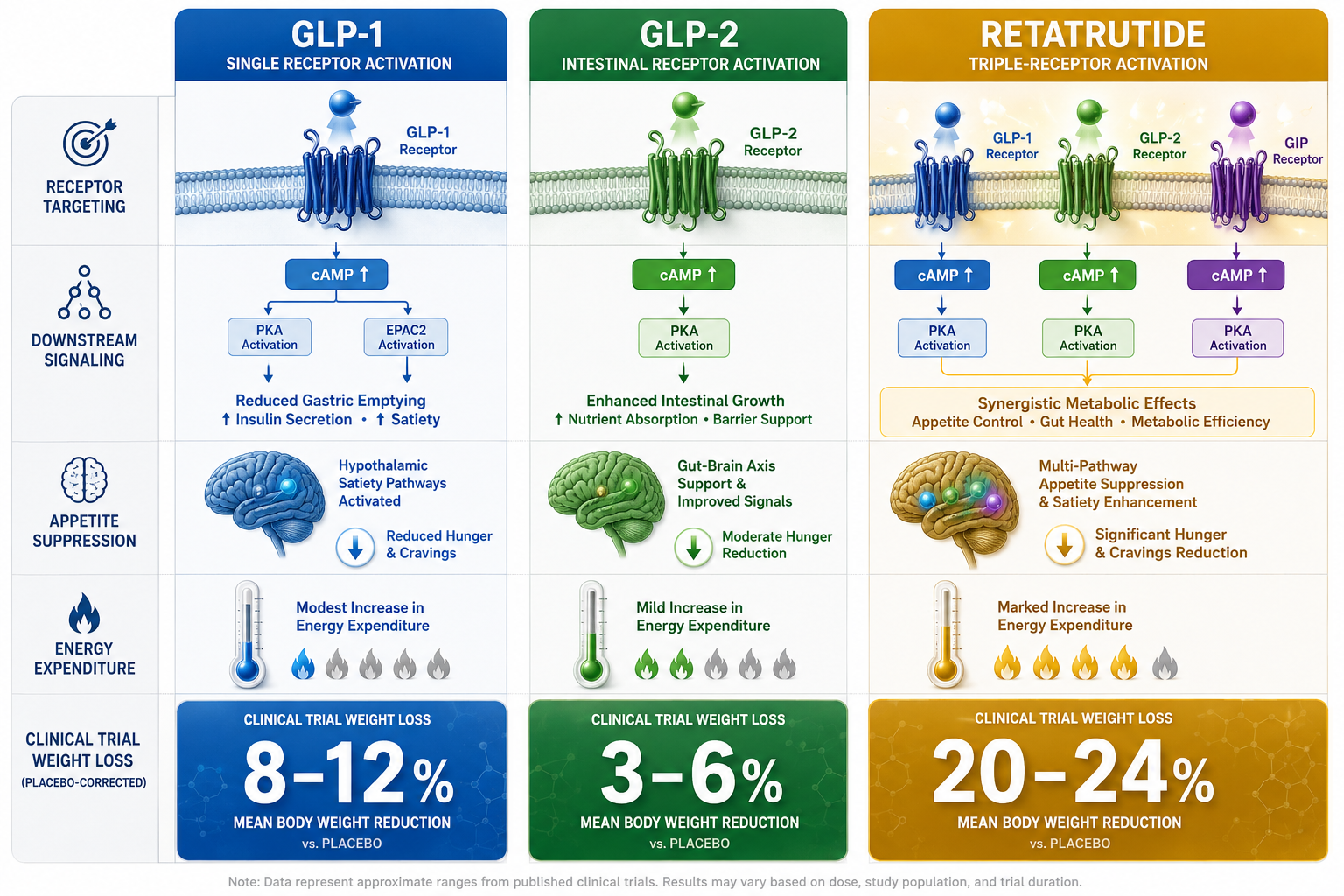
The coordinated activation of all three receptors produces layered metabolic effects:
- GLP-1R activation: Reduces food intake, slows gastric emptying, enhances insulin secretion
- GIPR activation: Amplifies insulin response, modulates adipose tissue signaling
- GCGR activation: Increases energy expenditure, improves hepatic lipid metabolism
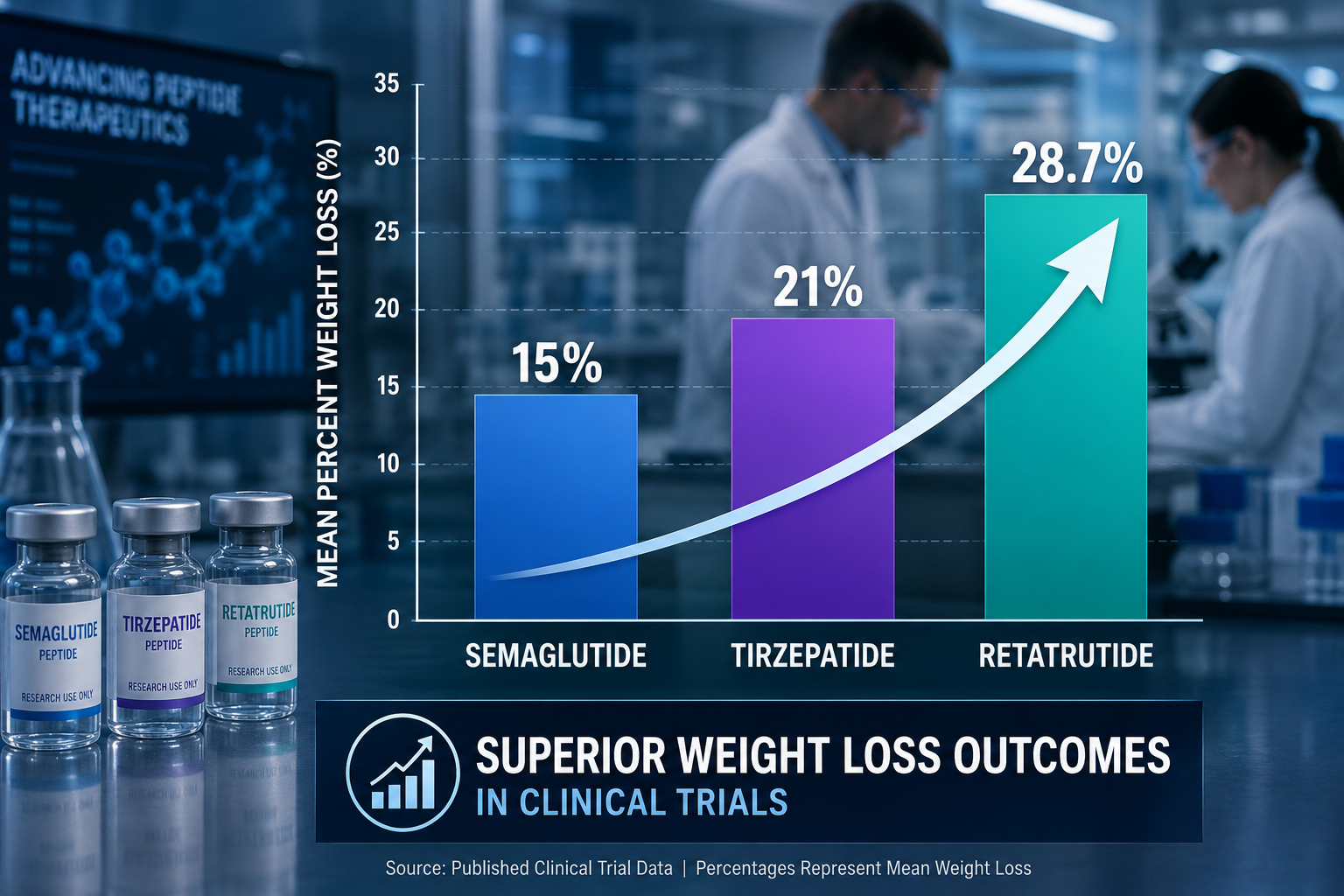
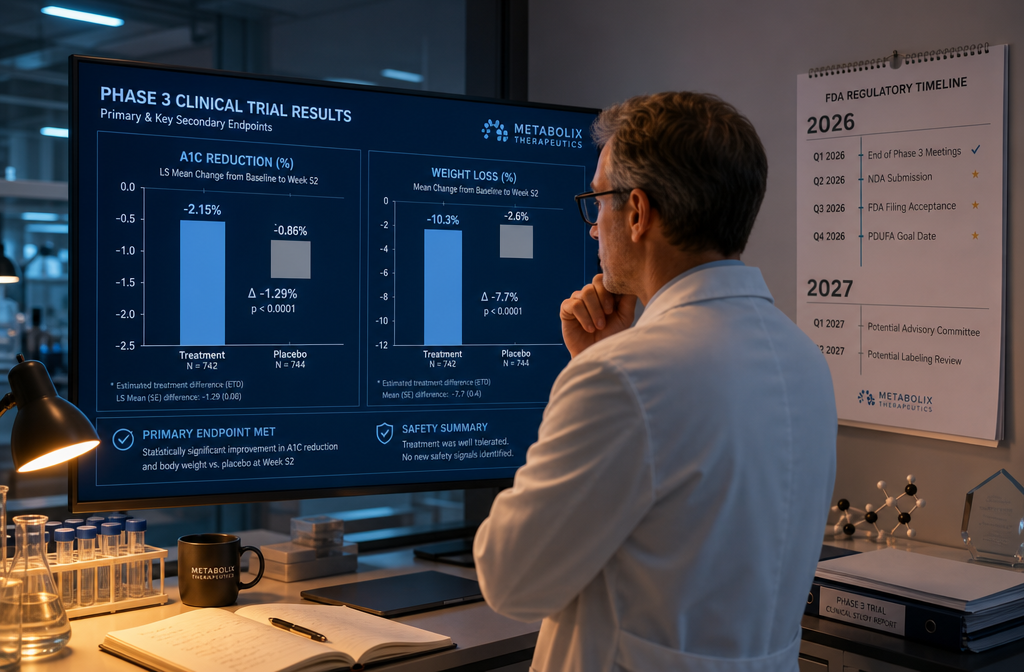
Phase 2 clinical trial data published in 2023 demonstrated significant weight loss and glycemic improvement in participants with obesity and type 2 diabetes. As of 2026, retatrutide has not received regulatory approval for human use and remains within the scope of clinical investigation and preclinical research.
For researchers building context around incretin-based peptide models, the GLP-3 Retatrutide incretin research themes page and the companion GLP-1 incretin research overview offer structured background. The cagrilintide synergy with GLP-1 research further illustrates how dual and triple agonist combinations are reshaping metabolic peptide research.
Bridging the Two Models: What Peptides and Polypeptides in Endocrine Research Reveal
The deeper insight from studying peptides and polypeptides in endocrine research: linking estrogen receptor signaling to enclomiphene and GLP-3 retatrutide models together is architectural. Enclomiphene works by subtracting a signal — removing estrogenic feedback — to let a natural axis reassert itself. Retatrutide works by adding multiple signals simultaneously, forcing coordinated receptor activation across organ systems.
Both strategies reflect a move away from single-target pharmacology. Both also interact, directly or indirectly, with estrogen receptor biology. GPER, for instance, has been implicated in metabolic regulation, and GLP-1 receptor signaling has documented interactions with sex hormone pathways in adipose and hepatic tissue.
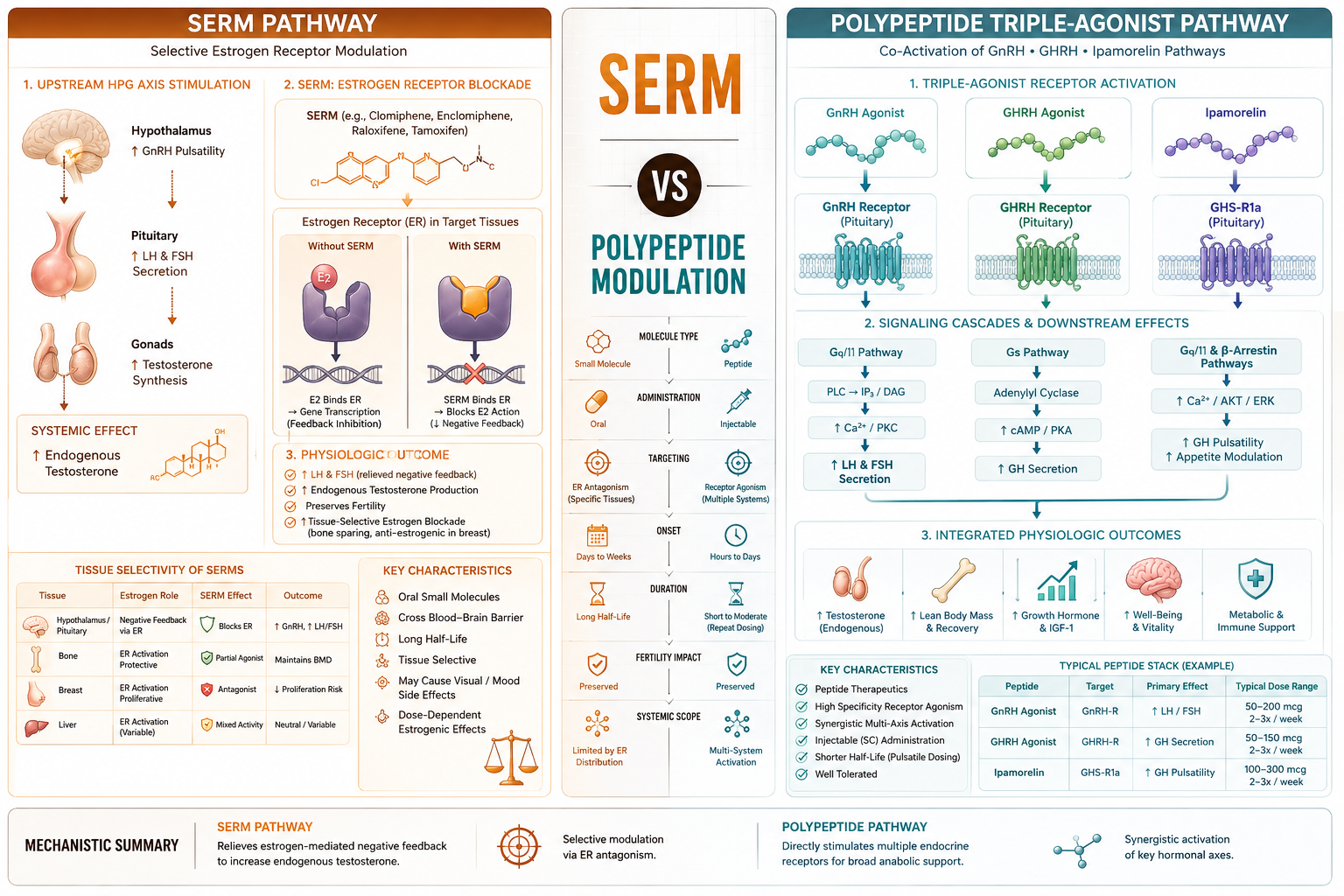
Key distinctions between serm-based and polypeptide-based endocrine modulation:
- Mechanism: Receptor blockade (serm) vs. receptor co-activation (polypeptide agonist)
- Axis impact: Preserves negative feedback (enclomiphene) vs. bypasses feedback (retatrutide)
- Structural class: Small molecule (enclomiphene) vs. synthetic peptide chain (retatrutide)
- Research maturity: Enclomiphene has longer clinical history; retatrutide is in active Phase 2/3 investigation
Researchers interested in how peptide structural biology shapes receptor selectivity may also find value in reviewing tesa research themes and the IPA muscle and fat research overview, both of which demonstrate how peptide sequence modifications alter tissue-level outcomes.
Conclusion
The convergence of estrogen receptor biology, serm pharmacology, and synthetic polypeptide design represents one of the most productive frontiers in endocrine research today. Enclomiphene demonstrates that precise receptor-site selectivity can restore entire hormonal axes with minimal disruption. Retatrutide demonstrates that a single engineered polypeptide can coordinate metabolic signaling across three receptor families simultaneously.
Actionable next steps for researchers:
- Review GPER-specific literature to understand non-genomic estrogen signaling before designing peptide interaction studies.
- Use enclomiphene's HPG axis preservation model as a benchmark when evaluating upstream versus downstream peptide interventions.
- Consult Phase 2 retatrutide data for structural insights into multi-receptor polypeptide engineering.
- Explore the comprehensive peptide catalog to identify research compounds relevant to metabolic and hormonal pathway studies.
- Prioritize compounds with published quality testing data — see quality testing protocols — when designing rigorous endocrine research protocols.
The field is moving fast. Researchers who understand both the receptor-level architecture and the structural biology of the peptides involved will be best positioned to interpret emerging data as it arrives.