CJC-1295 with Ipamorelin: Optimizing Growth Hormone Release for Research Studies
}
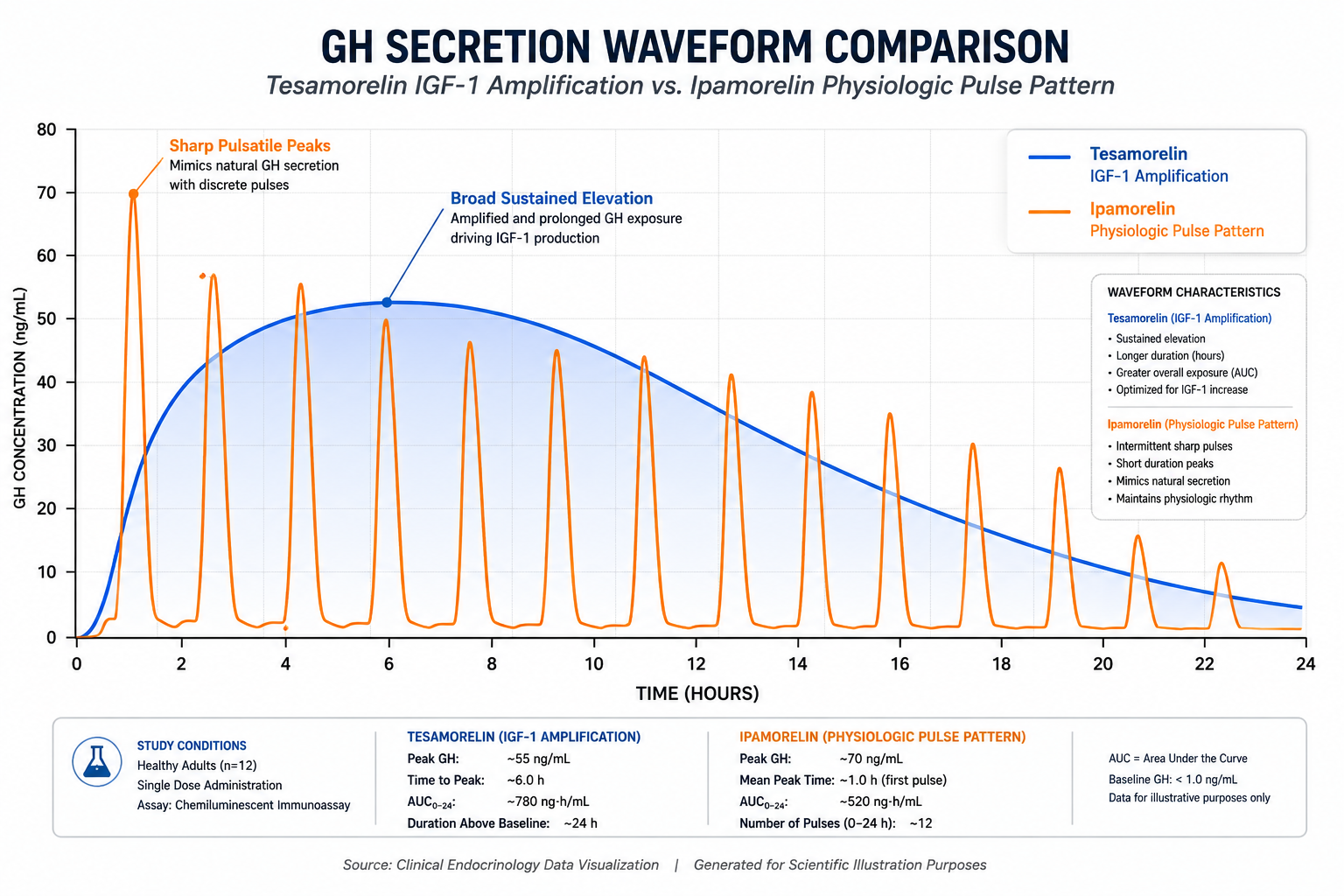
A single subcutaneous injection of CJC-1295 produced a 2- to 10-fold increase in mean plasma growth hormone levels lasting up to six days — a finding that reshaped how researchers think about pulsatile GH stimulation. When paired with Ipamorelin, this effect takes on a new dimension entirely. Understanding the science behind CJC-1295 with Ipamorelin: optimizing growth hormone release for research studies requires examining both peptides at the receptor level and then exploring what happens when their pathways converge.
Key Takeaways
- CJC-1295 is a long-acting GHRH analog; Ipamorelin is a selective ghrelin receptor agonist — they activate distinct GH-release pathways.
- Combining both peptides produces greater GH pulse amplitude and frequency than either compound alone.
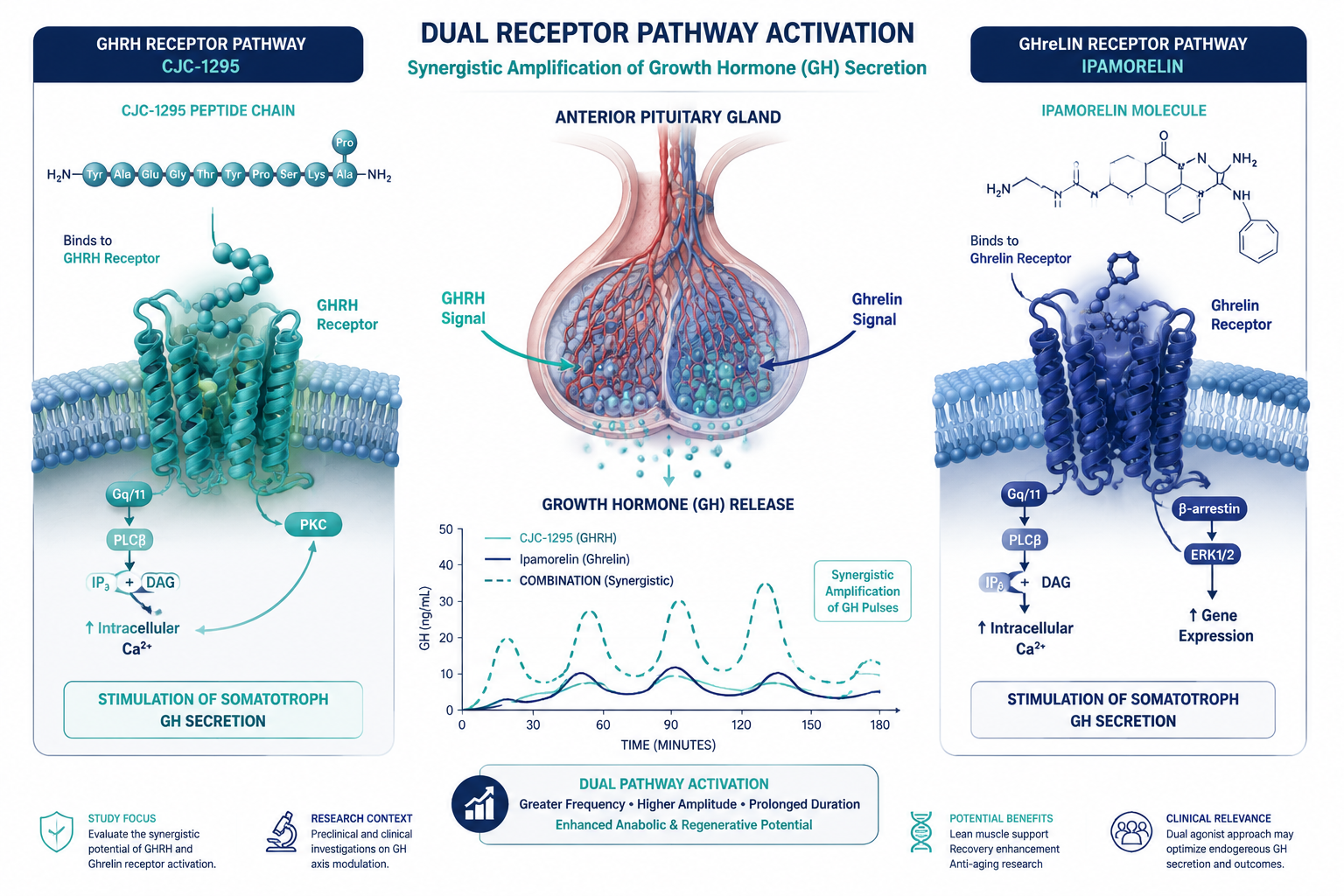
- A 2006 clinical study confirmed CJC-1295's extended half-life of 5.8 to 8.1 days and elevated IGF-1 for up to 11 days.
- Neither peptide is FDA-approved; both are classified as research chemicals and appear on the WADA prohibited list.
- No published randomized controlled trials exist for the combination as of 2026, making rigorous preclinical study design critical.
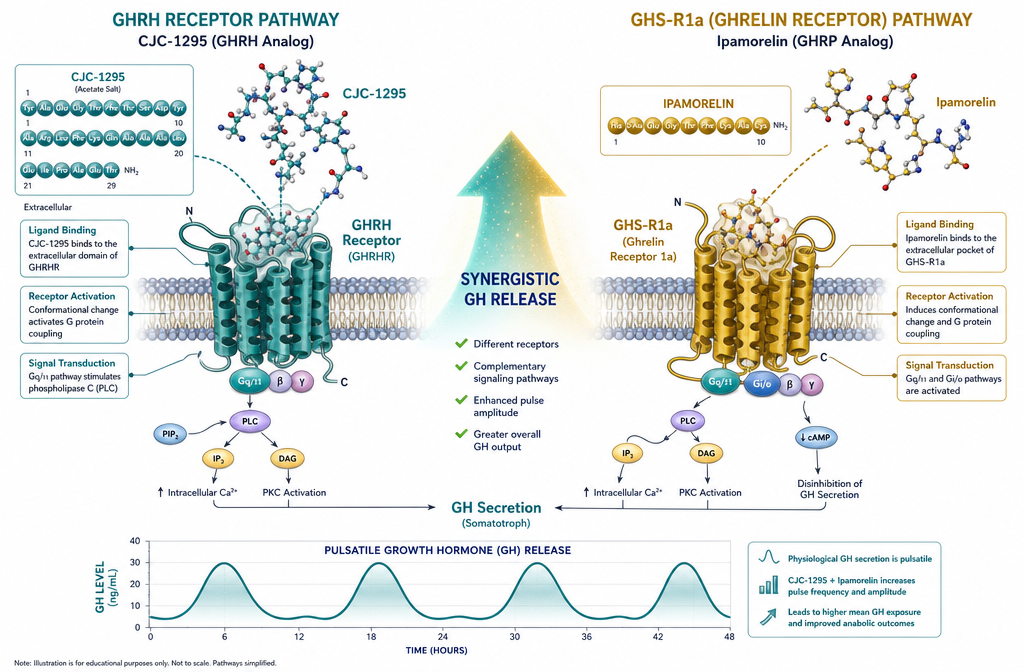
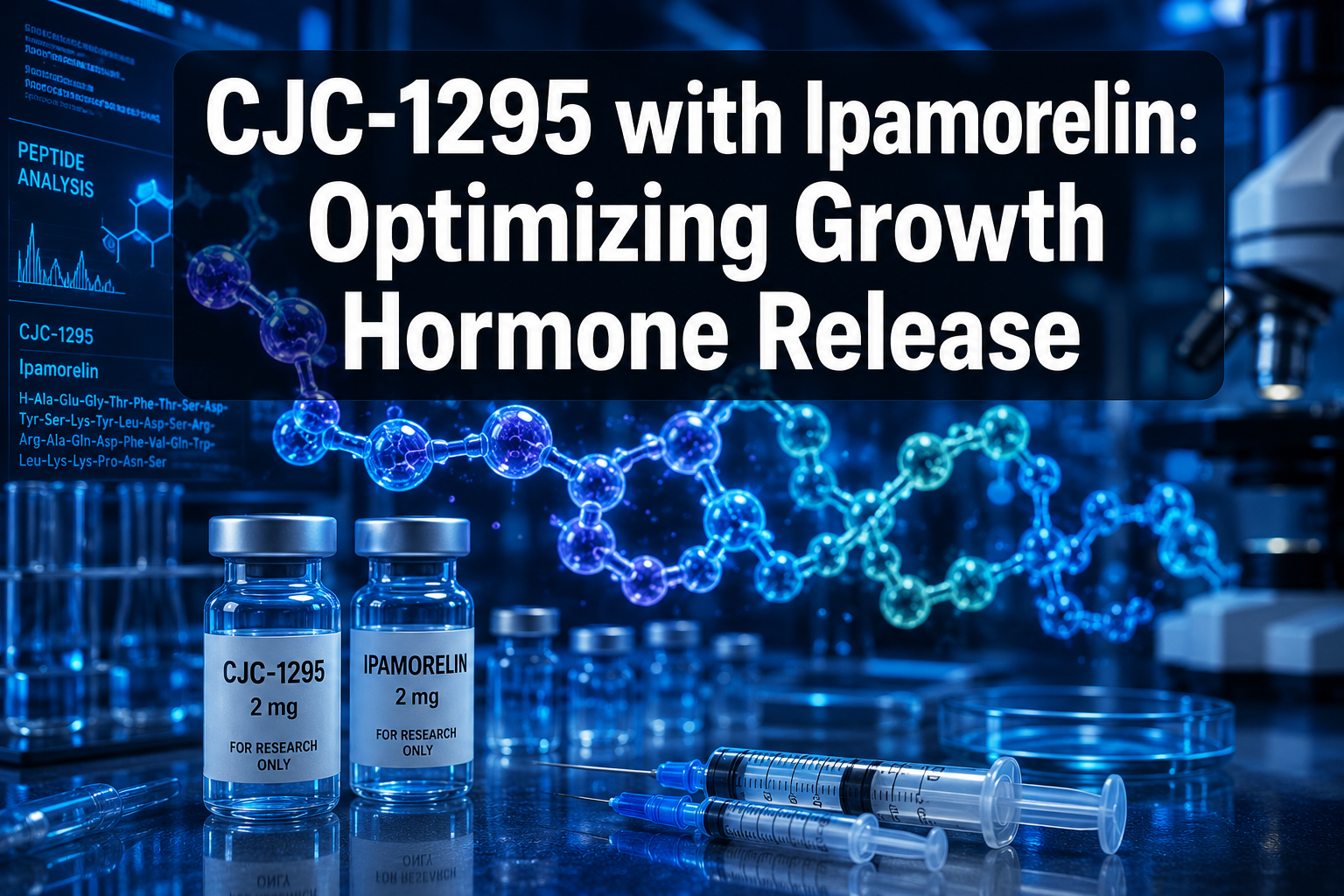
Mechanisms Behind the Synergy
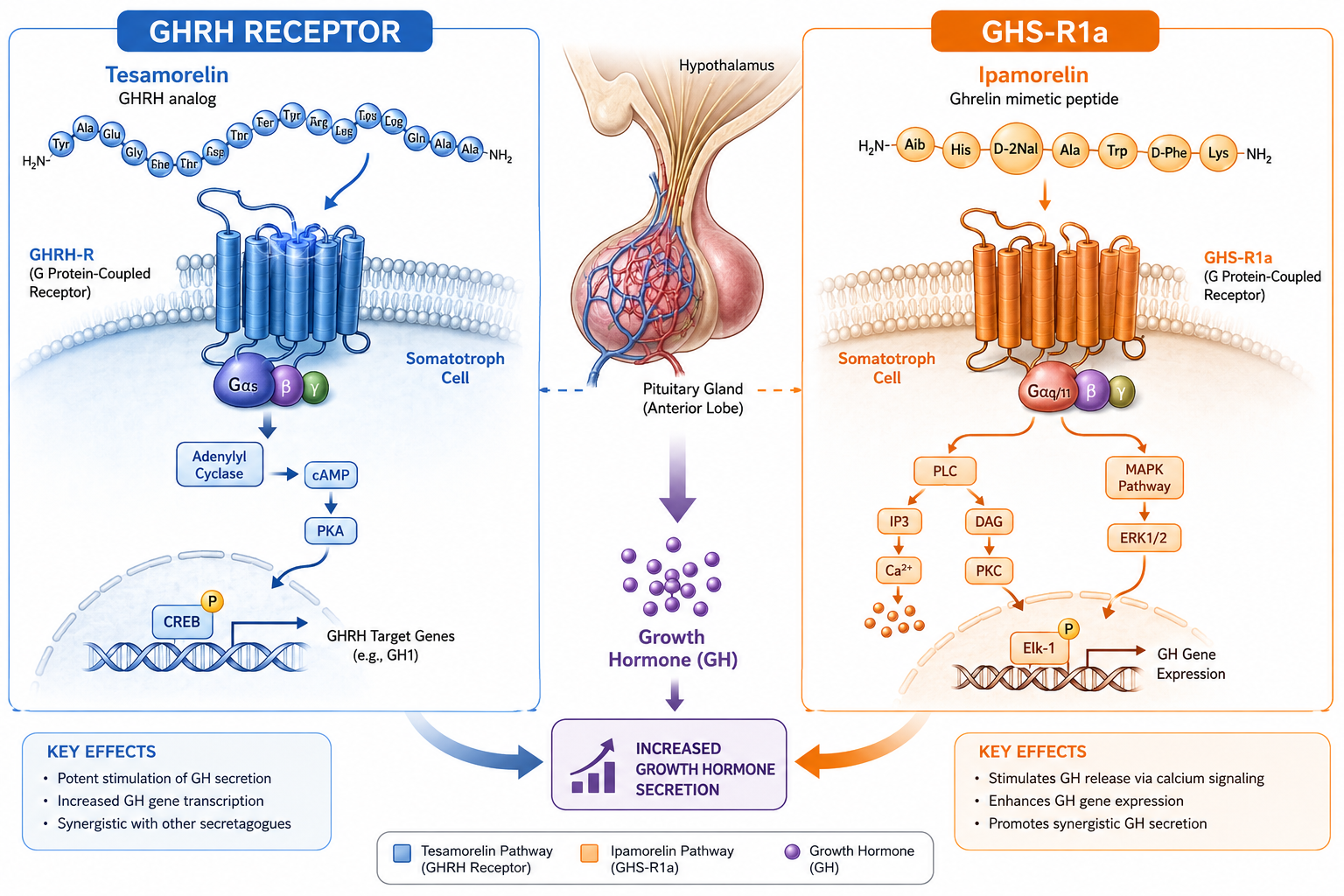
CJC-1295 is a modified analog of Growth Hormone-Releasing Hormone (GHRH). It binds to GHRH receptors on the anterior pituitary, signaling somatotroph cells to synthesize and release GH. Its key structural modification — Drug Affinity Complex (DAC) technology — allows it to bind albumin in plasma, dramatically extending its half-life to between 5.8 and 8.1 days. This stands in sharp contrast to sermorelin and CJC-1295 comparisons where sermorelin clears the body in roughly 10 to 12 minutes and tesa in approximately 30 minutes.
Ipamorelin operates through an entirely separate mechanism. It mimics ghrelin by binding to the GHS-R1a receptor, a G-protein-coupled receptor found on pituitary somatotrophs and hypothalamic neurons. Critically, Ipamorelin achieves GH stimulation without meaningfully elevating cortisol or prolactin, which distinguishes it from older secretagogues like GHRP-6 or GHRP-2.
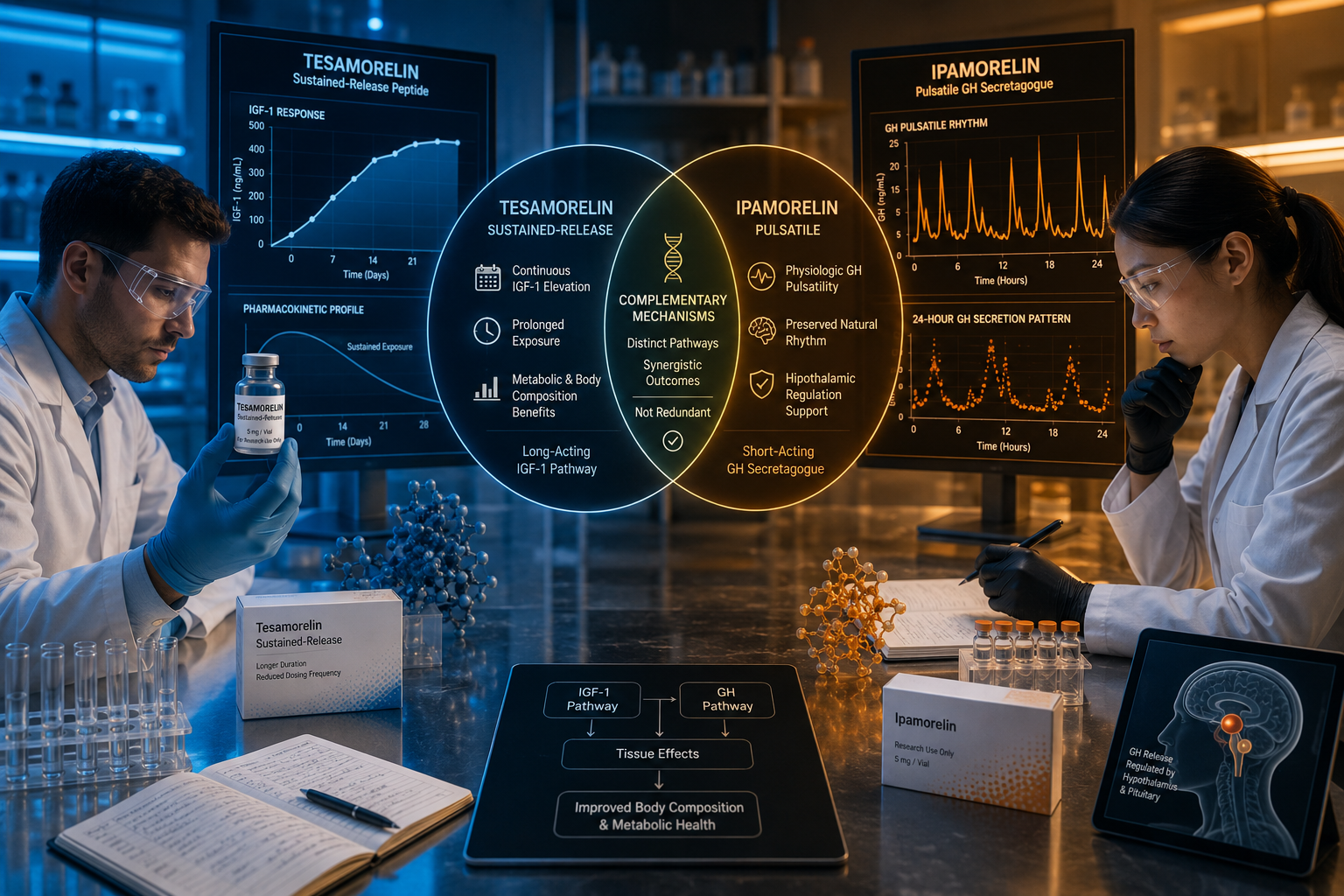
When both peptides are used together, the result is a dual-pathway amplification of GH release. GHRH receptor activation raises the ceiling on GH output, while ghrelin receptor stimulation increases the frequency of GH pulses. Research models studying this combination can explore the CJC-1295 no-DAC research themes alongside full DAC variants to isolate half-life variables.
Clinical Evidence and Research Protocols for CJC-1295 with Ipamorelin
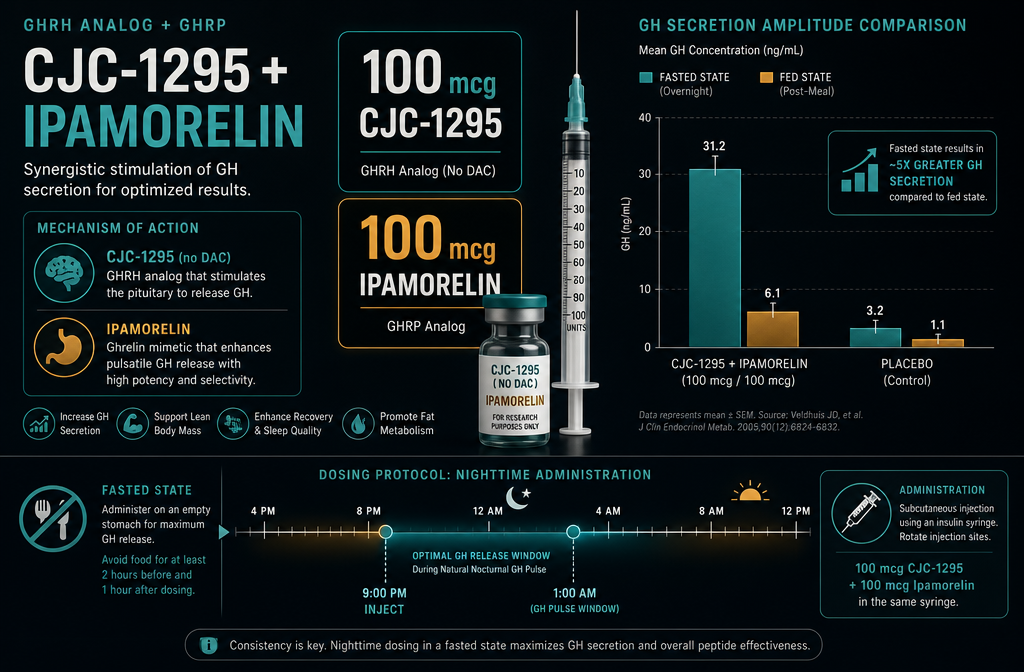
The foundational human data for CJC-1295 comes from a pivotal 2006 study published in the Journal of Clinical Endocrinology and Metabolism. Key findings included:
| Parameter | Observed Outcome |
|---|---|
| Plasma GH increase | 2- to 10-fold above baseline |
| Duration of GH elevation | Up to 6 days post-injection |
| IGF-1 increase | 1.5- to 3-fold above baseline |
| IGF-1 elevation duration | 9 to 11 days |
| Estimated half-life | 5.8 to 8.1 days |
| Tolerated dose range | 30 to 60 mcg/kg |
No serious adverse reactions were observed at these doses. However, no additional human RCTs have been published since 2006, and the CJC-1295/Ipamorelin combination has not been formally tested in published human controlled trials as of 2026.
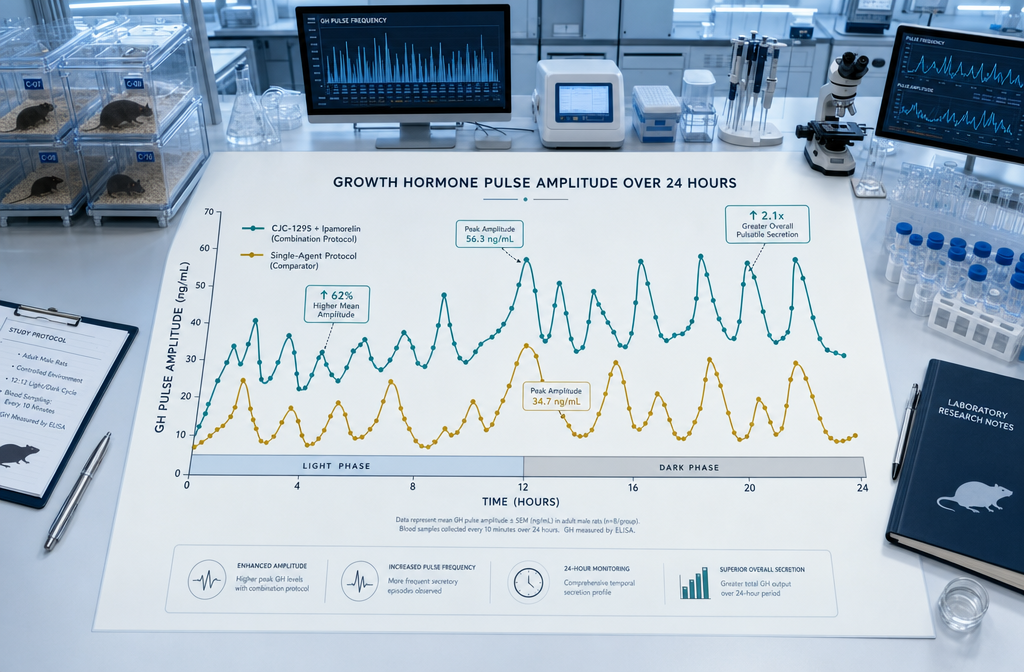
For preclinical research, the combination is typically studied using models that track pulsatile GH secretion patterns over 24-hour windows. Researchers interested in multi-peptide blends can also review tesa, CJC-1295, and Ipamorelin blend protocols to understand how additional GHRH analogs interact within the same framework. A related resource on combining tesa with CJC-1295 and Ipamorelin safety considerations addresses stack-level safety questions relevant to protocol design.
"While CJC-1295 and Ipamorelin can synergistically enhance GH release, their long-term safety and efficacy remain under-researched." — Dr. Quinn Stillson, April 2026
Regulatory Status, Risks, and Research Sourcing
As of 2026, neither CJC-1295 nor Ipamorelin holds FDA approval for any indication. Both are classified as research chemicals for laboratory use only and are listed on the World Anti-Doping Agency's prohibited substances list. This regulatory status has direct implications for study design, institutional review, and sourcing standards.
Key risk considerations for research models include:
- Potential receptor desensitization with prolonged GH secretagogue exposure
- Difficulty assessing long-term consequences of sustained elevated IGF-1 without longitudinal human data
- Variability in peptide purity across suppliers, which can confound results
Sourcing peptides with verified purity documentation is non-negotiable for valid research outcomes. Reviewing certificates of analysis before procurement ensures compound integrity. Researchers building broader metabolic panels may also find value in MOTS-c metabolic flexibility research themes or BPC-157 research themes as complementary study arms.
For those sourcing the combination directly, the CJC-1295 with Ipamorelin 10mg research product provides a pre-blended option with documented testing standards.
Conclusion
CJC-1295 with Ipamorelin: optimizing growth hormone release for research studies represents one of the most mechanistically coherent dual-peptide strategies in current GH research. The GHRH/ghrelin receptor co-activation model offers a compelling framework for studying pulsatile GH dynamics, IGF-1 modulation, and downstream metabolic effects.
Actionable next steps for researchers in 2026:
- Define your GH endpoint clearly — pulse amplitude, IGF-1 area under the curve, or downstream tissue response.
- Source verified, tested peptides with published certificates of analysis to eliminate purity as a confounding variable.
- Design time-course sampling protocols that capture the extended half-life profile of CJC-1295 (up to 11 days for IGF-1 elevation).
- Consult current regulatory guidance before initiating any study involving WADA-listed compounds.
- Review adjacent peptide research — including Ipamorelin and sermorelin stack research — to contextualize your findings within the broader secretagogue literature.
The data foundation exists. Rigorous, well-sourced research design is what transforms that foundation into meaningful scientific contribution.