CJC-1295 with DAC vs. Without DAC: Impact on Growth Hormone Secretion and Experimental Design
A single structural modification — the addition of a Drug Affinity Complex linker — transforms a short-acting peptide into one with a half-life measured in days rather than minutes. That pharmacokinetic gap sits at the heart of the debate around CJC-1295 with DAC vs. Without DAC: Impact on Growth Hormone Secretion and Experimental Design, and it shapes every variable a researcher must account for when designing a growth hormone (GH) study.
Key Takeaways
- CJC-1295 with DAC binds covalently to serum albumin, extending its half-life to approximately 6-8 days.
- CJC-1295 without DAC (Mod GRF 1-29) has a half-life of roughly 30 minutes and produces pulsatile GH release.
- The DAC variant sustains GH elevation but may disrupt natural pulsatile secretion and risk receptor desensitization.
- Experimental design choices — dosing frequency, combination partners, and outcome measures — differ significantly between the two forms.
- Researchers often pair CJC-1295 without DAC with GHRPs like Ipamorelin to closely mimic physiological GH rhythms.
The Molecular Difference: What DAC Actually Does
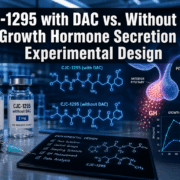
The Drug Affinity Complex (DAC) is a maleimidopropionic acid linker attached to the C-terminus of CJC-1295. This addition allows the peptide to form a covalent bond with the Cys34 residue of serum albumin, effectively anchoring it to a long-lived carrier protein circulating in the bloodstream.
The result is a meaningful increase in molecular weight — from approximately 3,367 Da (without DAC) to roughly 3,647 Da (with DAC) — and a dramatic extension of circulating half-life.
| Feature | CJC-1295 with DAC | CJC-1295 without DAC |
|---|---|---|
| Half-life | ~6-8 days | ~30 minutes |
| Molecular weight | ~3,647 Da | ~3,367 Da |
| Albumin binding | Covalent (Cys34) | None |
| GH release pattern | Sustained, continuous | Pulsatile, transient |
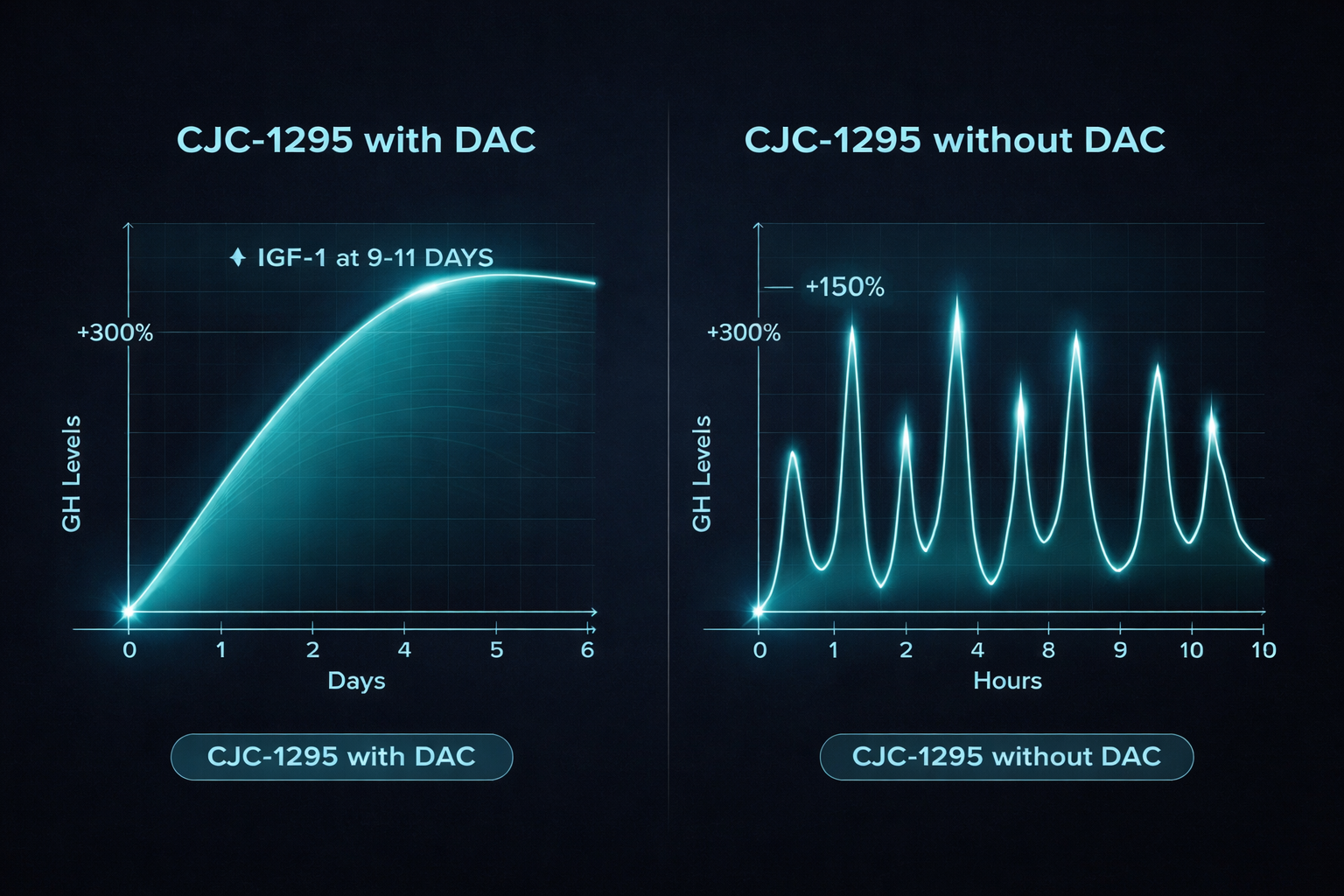
| Dosing frequency | Once or twice weekly | Multiple times daily |
For researchers exploring CJC-1295 research findings, understanding this structural distinction is the essential first step before any protocol is designed.
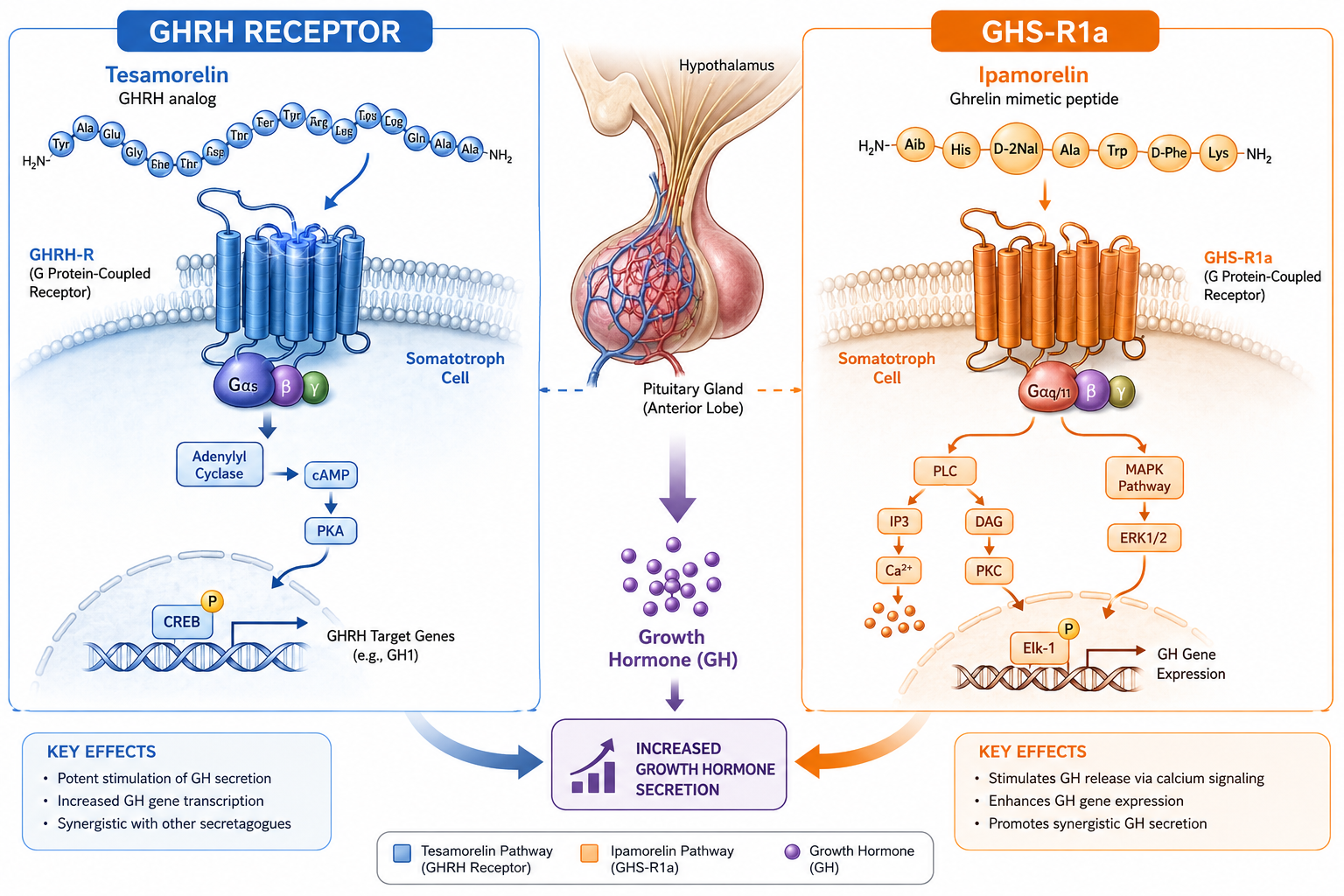
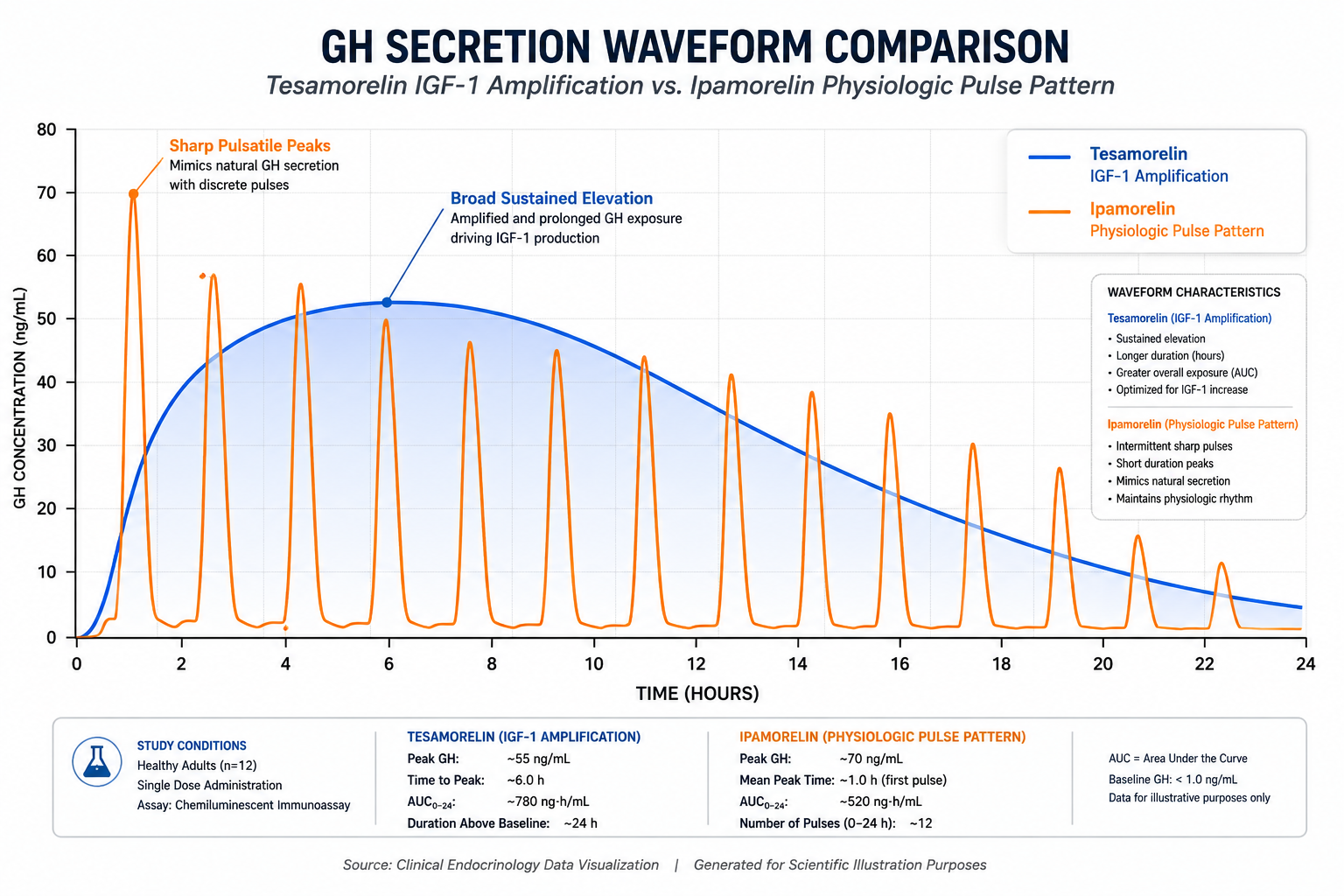
GH Secretion Patterns: Sustained Elevation vs. Physiological Pulses
The pharmacokinetic difference between the two variants produces fundamentally different growth hormone secretion profiles, each with distinct research implications.
CJC-1295 with DAC: Continuous Stimulation
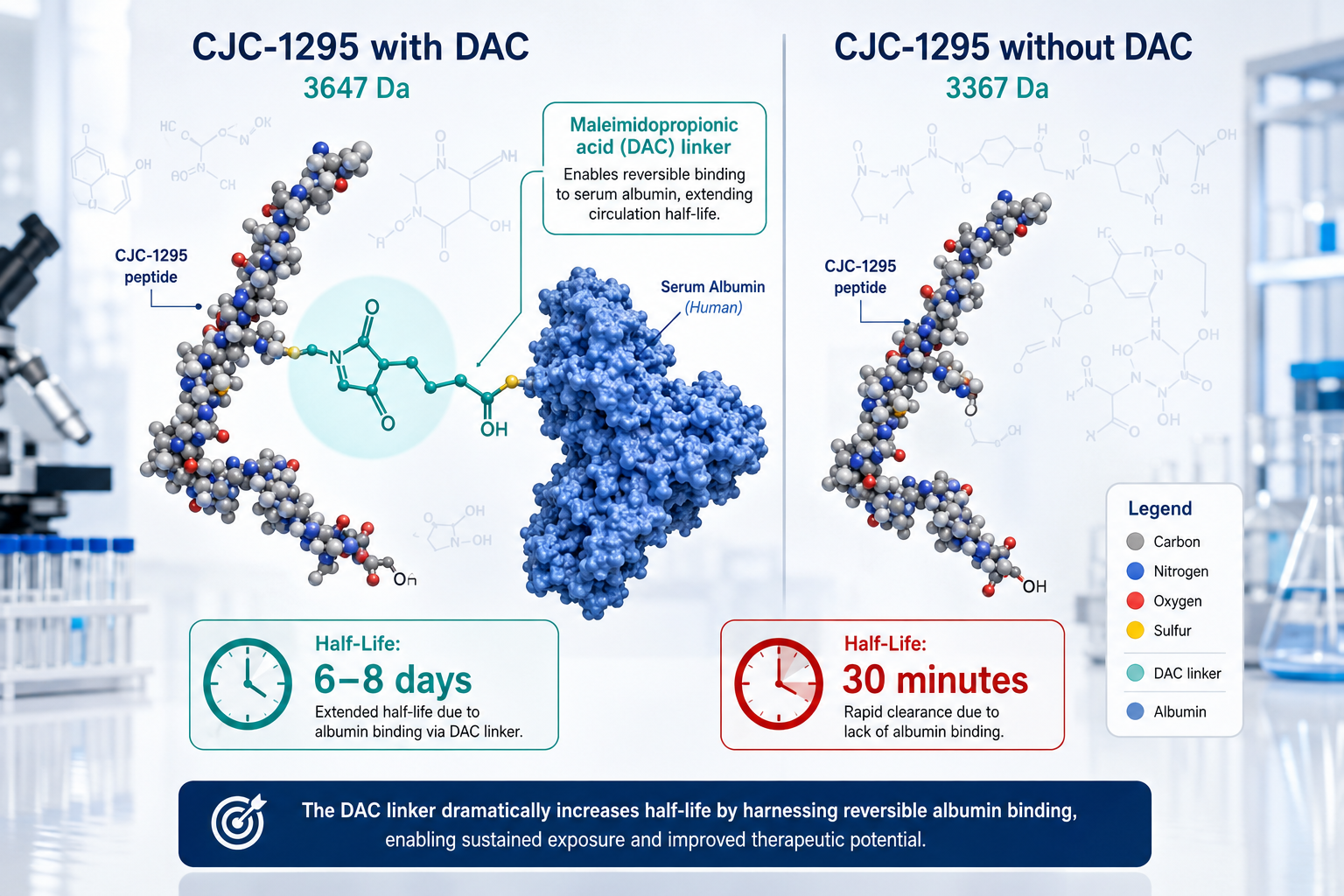
Clinical data from Phase I and II trials conducted in the mid-2000s showed that a single dose of CJC-1295 with DAC produced a 2-10 fold increase in GH levels lasting up to six days. IGF-1 levels remained elevated for 9-11 days following that single administration. This sustained profile makes the DAC variant well-suited for studies requiring prolonged GH elevation without frequent dosing.
However, continuous GH stimulation carries a notable concern: receptor desensitization. Prolonged activation of GHRH receptors may reduce their sensitivity over time, potentially blunting the GH response in longer-term protocols.
CJC-1295 without DAC: Mimicking Natural Rhythms
CJC-1295 without DAC — also called Mod GRF 1-29 — produces short, sharp GH pulses that closely mirror the body's natural pulsatile secretion pattern. This pulsatility is considered important for maintaining insulin sensitivity and preserving receptor responsiveness.
"Pulsatile GH release is not merely a physiological quirk — it is a functional requirement for downstream signaling fidelity."
Researchers focused on physiological accuracy tend to favor the non-DAC variant. It is frequently combined with growth hormone-releasing peptides (GHRPs) such as Ipamorelin to amplify pulsatile release. The Sermorelin, Ipamorelin, and CJC-1295 combination represents a common multi-peptide research approach built on this principle. Similarly, Ipamorelin and Sermorelin stack research provides additional context for synergistic GHRH-GHRP protocols.
Experimental Design Considerations for Each Variant
Choosing between these two forms in a research context is not simply a matter of convenience — it determines the biological question the experiment can validly answer.
When to Use the DAC Variant
- Studies examining sustained GH elevation and downstream IGF-1 responses
- Protocols where infrequent dosing (once or twice weekly) is operationally necessary
- Research into conditions historically linked to GH deficiency, reflecting the peptide's Phase II trial history
When to Use the Non-DAC Variant
- Protocols designed to replicate natural pulsatile GH secretion
- Studies assessing receptor sensitivity over time
- Combination research with GHRPs, where timing and pulse synchronization matter
For researchers also exploring related GHRH analogs, comparing Tesamorelin vs. Sermorelin offers useful pharmacokinetic context. The Tesamorelin and CJC-1295 blend research further illustrates how multi-peptide designs can address complex GH axis questions. Researchers interested in body composition outcomes may also find the Tesamorelin body composition research themes page a valuable reference point.
Dosing frequency is perhaps the most practical design variable. The DAC variant's weekly schedule reduces protocol complexity, while the non-DAC variant's multiple-daily-injection requirement demands tighter experimental control but yields data more reflective of physiological GH dynamics.
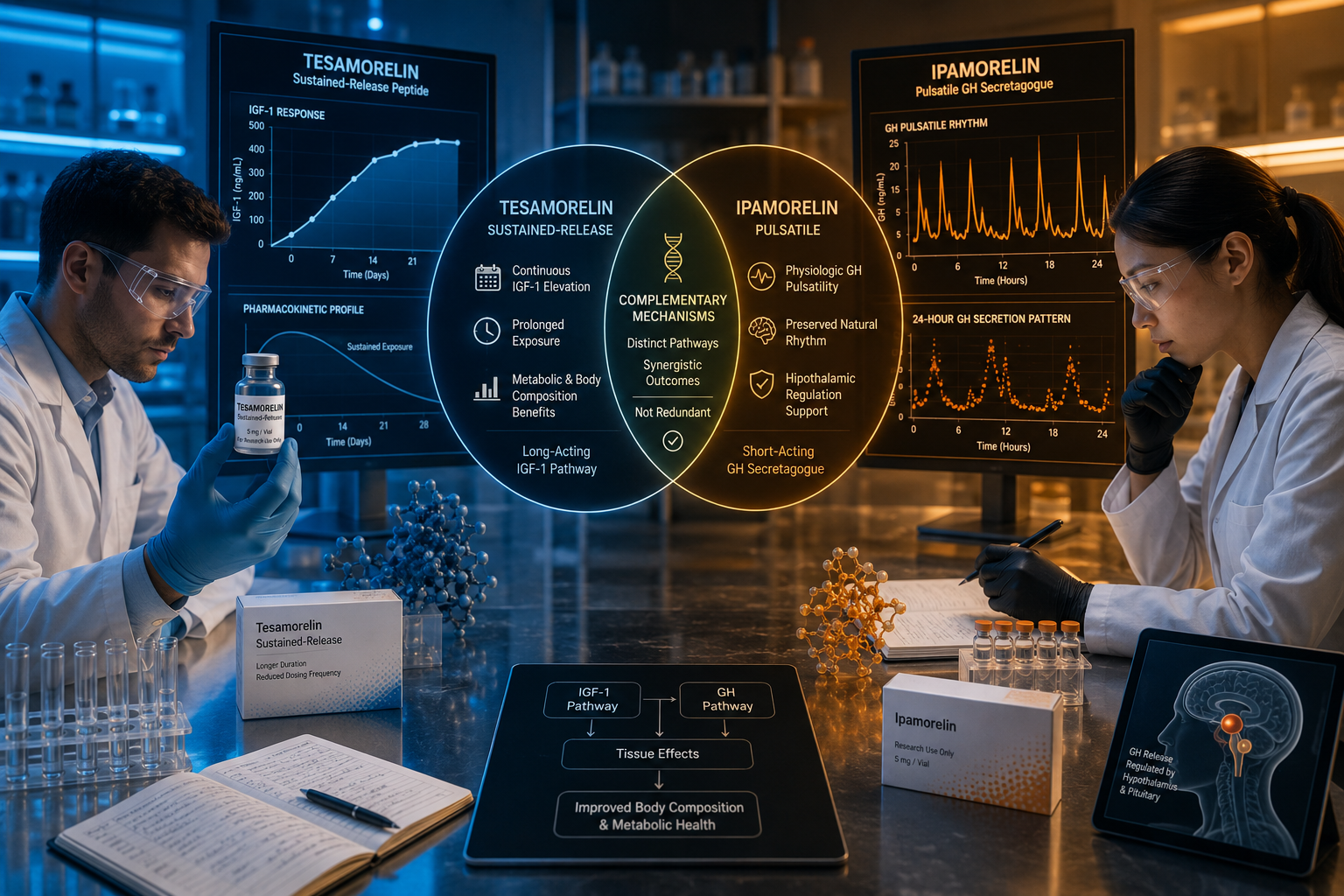
Conclusion
The comparison of CJC-1295 with DAC vs. Without DAC: Impact on Growth Hormone Secretion and Experimental Design ultimately comes down to one core question: does the research require sustained GH elevation or physiological pulsatility?
The DAC variant offers convenience and prolonged action through albumin binding, making it appropriate for sustained-elevation protocols. The non-DAC variant preserves natural GH rhythm, reduces receptor desensitization risk, and pairs effectively with GHRPs for synergistic research designs.
Actionable next steps for researchers in 2026:
- Define the GH secretion profile your study requires before selecting a variant.
- Account for dosing frequency in your experimental timeline and resource planning.
- Consider combination protocols with verified GHRPs when pulsatile secretion fidelity is the priority.
- Review available CJC-1295 research findings and related blend data to inform protocol selection.