Enclomiphene in Male Endocrine Research: Mechanism vs Clomiphene and Overlaps With Luteinizing Phase Physiology
Only one isomer inside a decades-old fertility drug is responsible for raising testosterone in men — and isolating it may change how researchers approach male hypogonadism entirely. That single compound is enclomiphene, and its growing presence in male endocrine research is reshaping how scientists think about the hypothalamic-pituitary-gonadal (HPG) axis.
Research into enclomiphene in male endocrine research: mechanism vs clomiphene and overlaps with luteinizing phase physiology has accelerated in 2026, driven by demand for testosterone-raising strategies that do not suppress fertility. Understanding why enclomiphene works — and how it differs from its parent compound — requires a close look at receptor pharmacology and the fundamental biology of luteinizing hormone (LH) signaling.
Key Takeaways
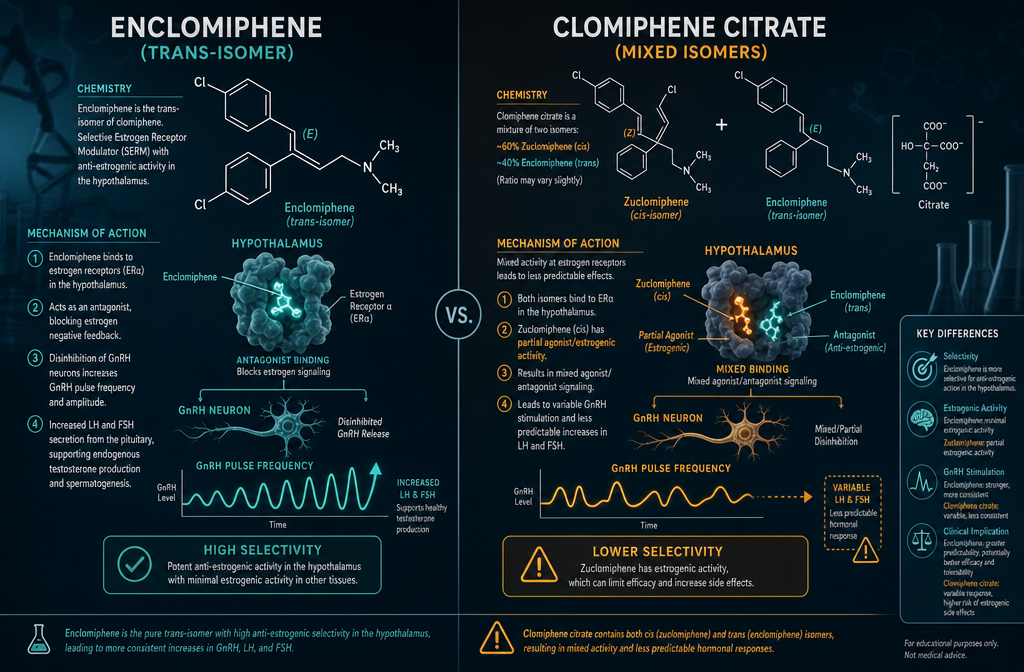
- Enclomiphene is the trans-isomer of clomiphene citrate and is solely responsible for its anti-estrogenic, testosterone-stimulating effects in men.
- It blocks hypothalamic estrogen receptors, increasing GnRH pulsatility and driving LH and FSH release — mirroring the natural luteinizing phase feedback loop.
- Unlike exogenous testosterone replacement therapy (TRT), enclomiphene preserves sperm production and endogenous hormone signaling.
- Zuclomiphene, the other isomer in clomiphene, carries weak estrogenic activity and a longer half-life, contributing to mood and visual side effects.
- Clinical data show enclomiphene produces meaningful testosterone increases with a lower adverse-event profile than mixed clomiphene.
How Enclomiphene Works: Selective Estrogen Receptor Modulation
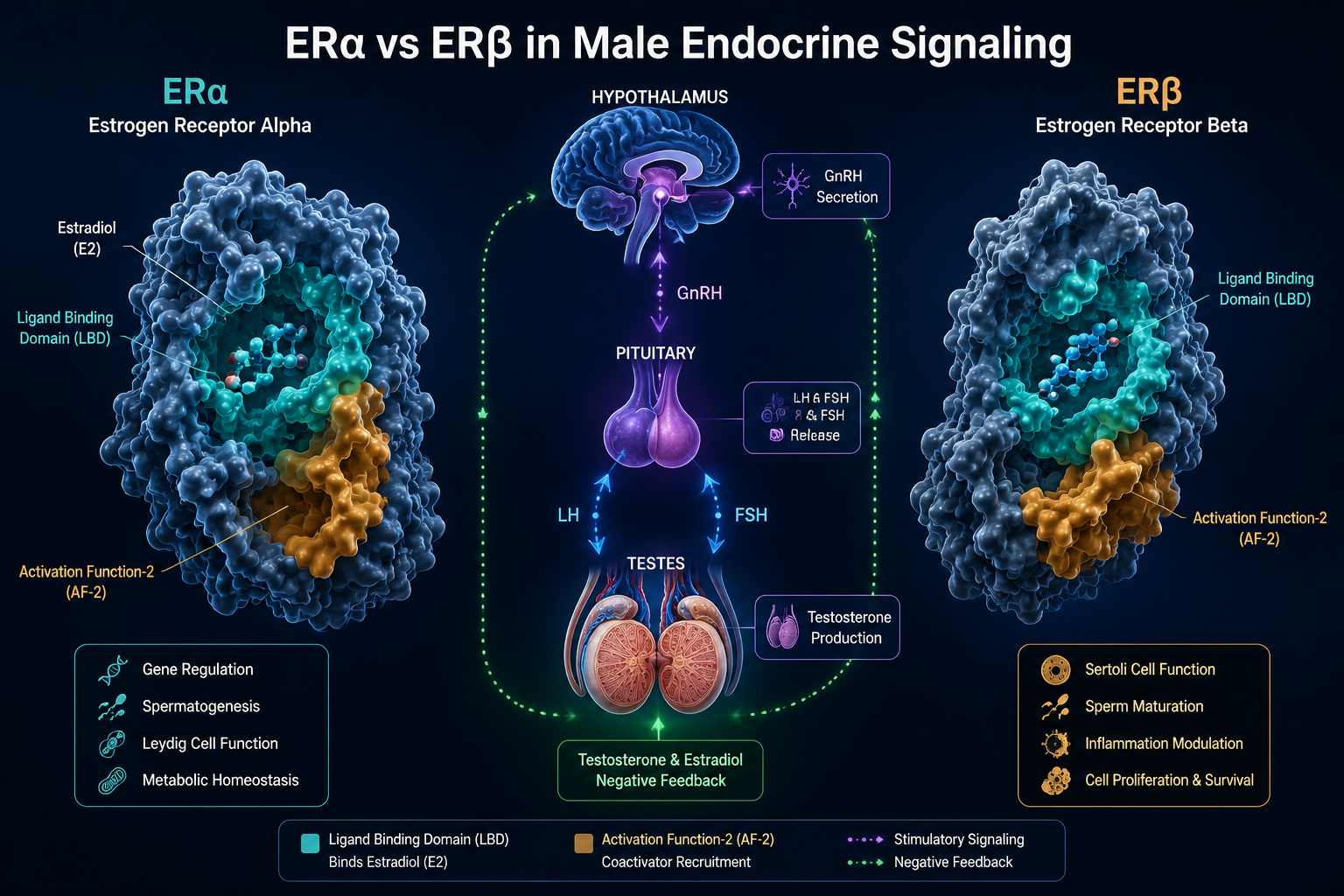
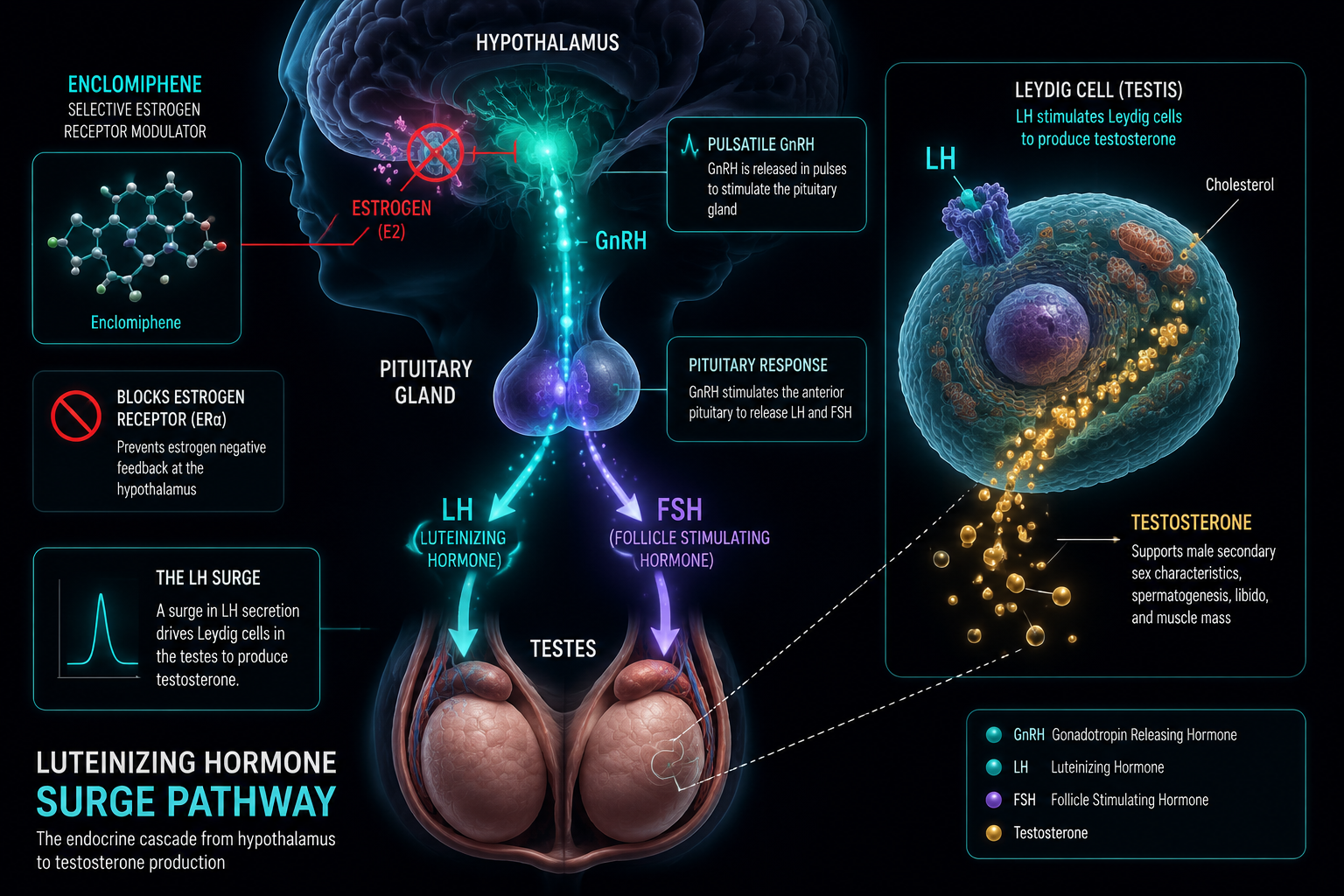
Enclomiphene is classified as a selective estrogen receptor modulator (serm). Its primary action occurs at estrogen receptors in the hypothalamus and pituitary gland. Under normal physiology, circulating estradiol binds to these receptors and signals the hypothalamus to reduce gonadotropin-releasing hormone (GnRH) output — a classic negative feedback loop.
Enclomiphene competitively blocks those receptors. With estradiol unable to deliver its suppressive signal, GnRH pulsatility increases. The pituitary responds by secreting more LH and FSH. Elevated LH then stimulates Leydig cells in the testes to synthesize testosterone, while FSH supports spermatogenesis.
Key pharmacokinetic facts:
| Parameter | Value |
|---|---|
| Half-life | ~10 hours |
| Time to peak serum concentration | 2-3 hours post-ingestion |
| Steady-state dose | 25 mg/day |
This rapid clearance is clinically significant. Because enclomiphene leaves the body quickly, its receptor blockade is time-limited and controllable — a meaningful advantage in research settings.
Enclomiphene in Male Endocrine Research: Mechanism vs Clomiphene and Overlaps With Luteinizing Phase Physiology
The Isomer Problem With Clomiphene Citrate
Clomiphene citrate is not a single compound. It is a 50:50 mixture of two geometric isomers:
- Enclomiphene (trans-isomer): Blocks estrogen receptors, drives GnRH and LH release, raises testosterone.
- Zuclomiphene (cis-isomer): Carries weak estrogenic activity, has a much longer half-life, and accumulates in tissue over time.
Zuclomiphene's estrogenic activity and slow elimination are linked to side effects reported with clomiphene use, including mood disturbances, reduced libido, and visual changes. By isolating enclomiphene, researchers remove this confounding variable entirely.
Connection to Luteinizing Phase Physiology
The luteinizing phase in reproductive biology refers to the period surrounding the LH surge — a sharp spike in LH that triggers ovulation in females and, in males, governs tonic testosterone production. In men, LH is released in pulses from the pituitary throughout the day, each pulse prompting Leydig cell testosterone output.
Enclomiphene essentially amplifies this pulsatile system. By lifting estradiol's brake on the hypothalamus, it restores or enhances the natural LH-driven testosterone cascade. This overlap with luteinizing phase physiology is why enclomiphene is particularly relevant for men with secondary hypogonadism — a condition where the testes are functional but the upstream HPG signaling is insufficient.
Researchers studying neuroendocrine and innate immunity interactions will recognize this HPG axis modulation as part of a broader hormonal communication network that extends well beyond reproductive function.
Clinical Evidence and Safety Profile
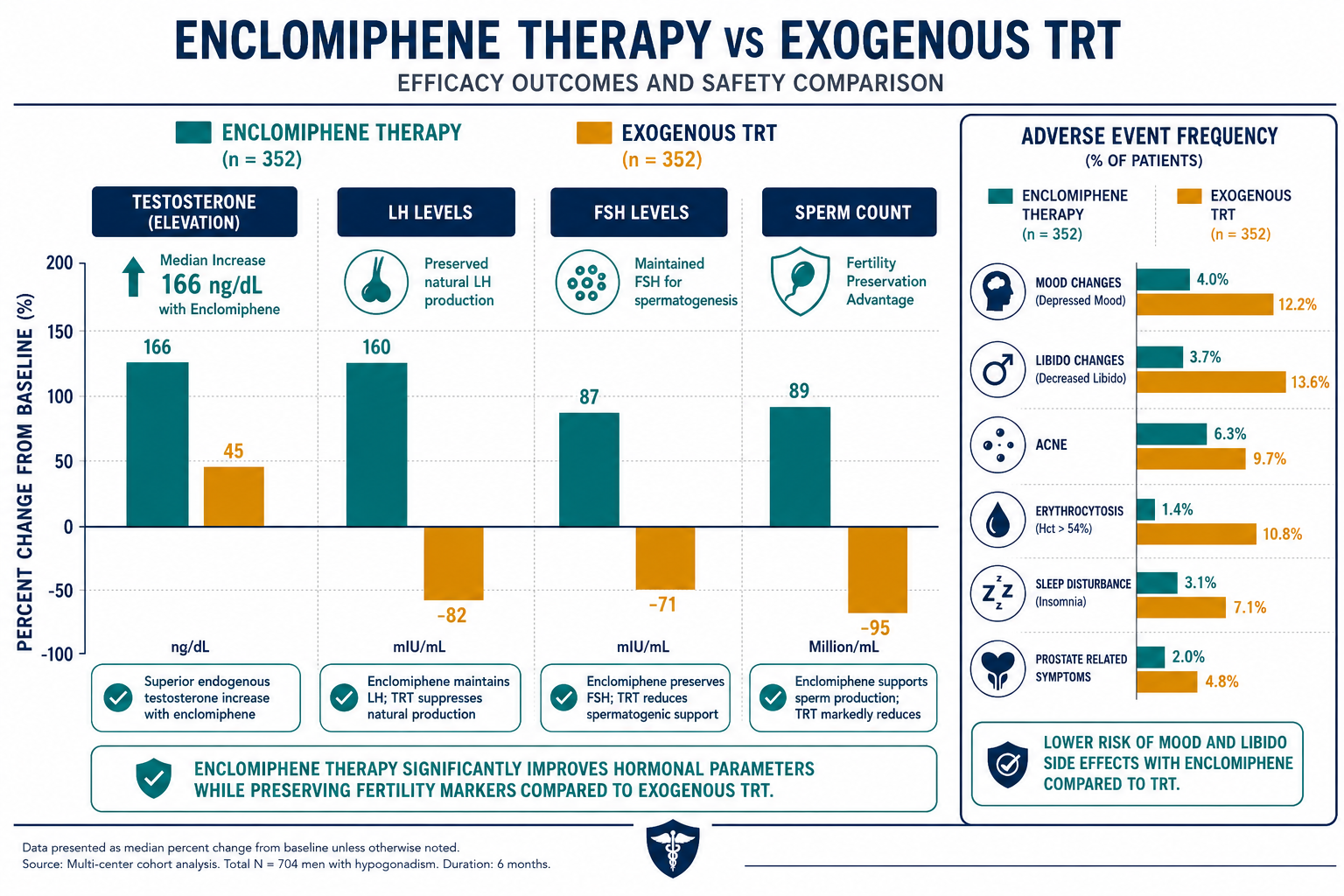
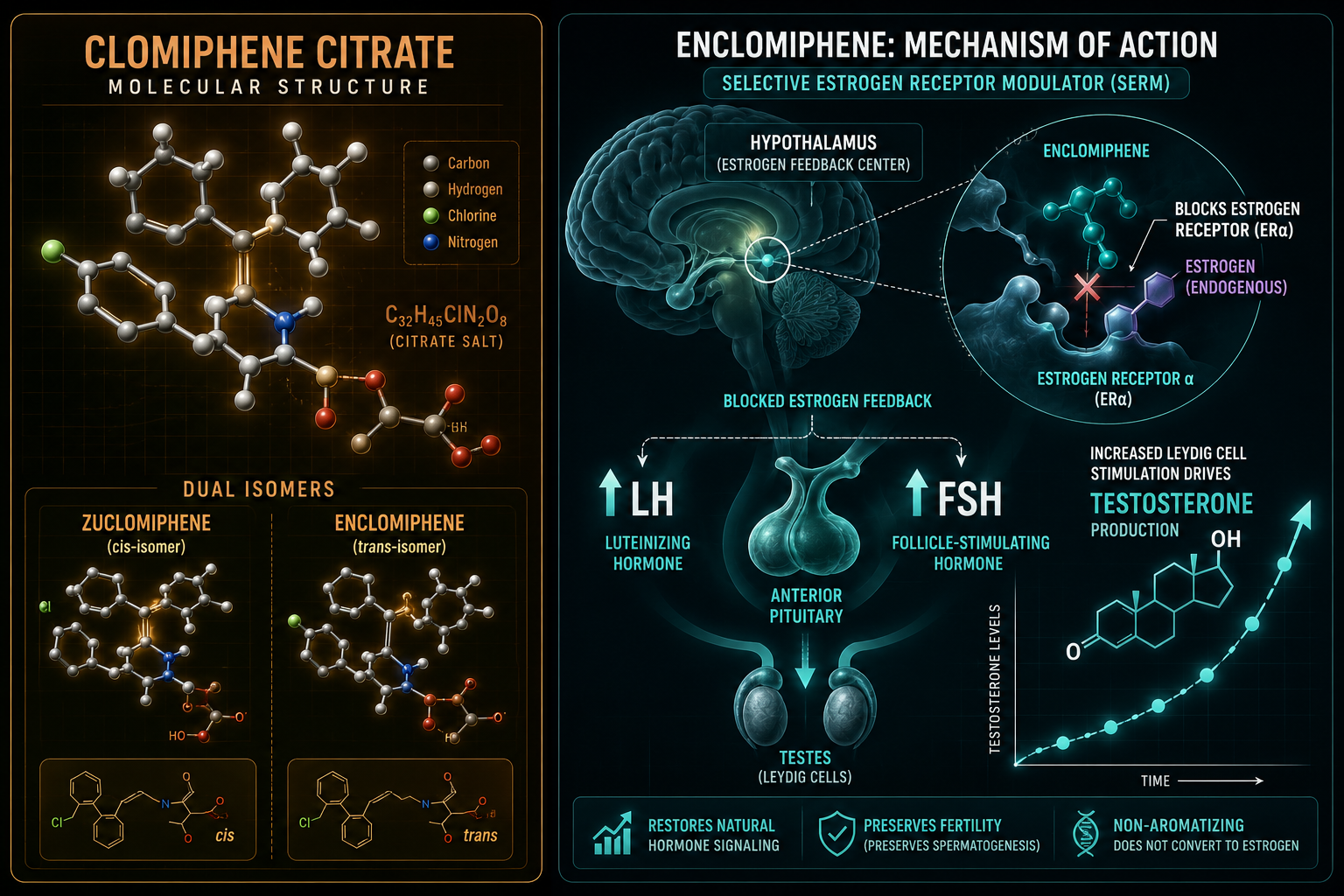
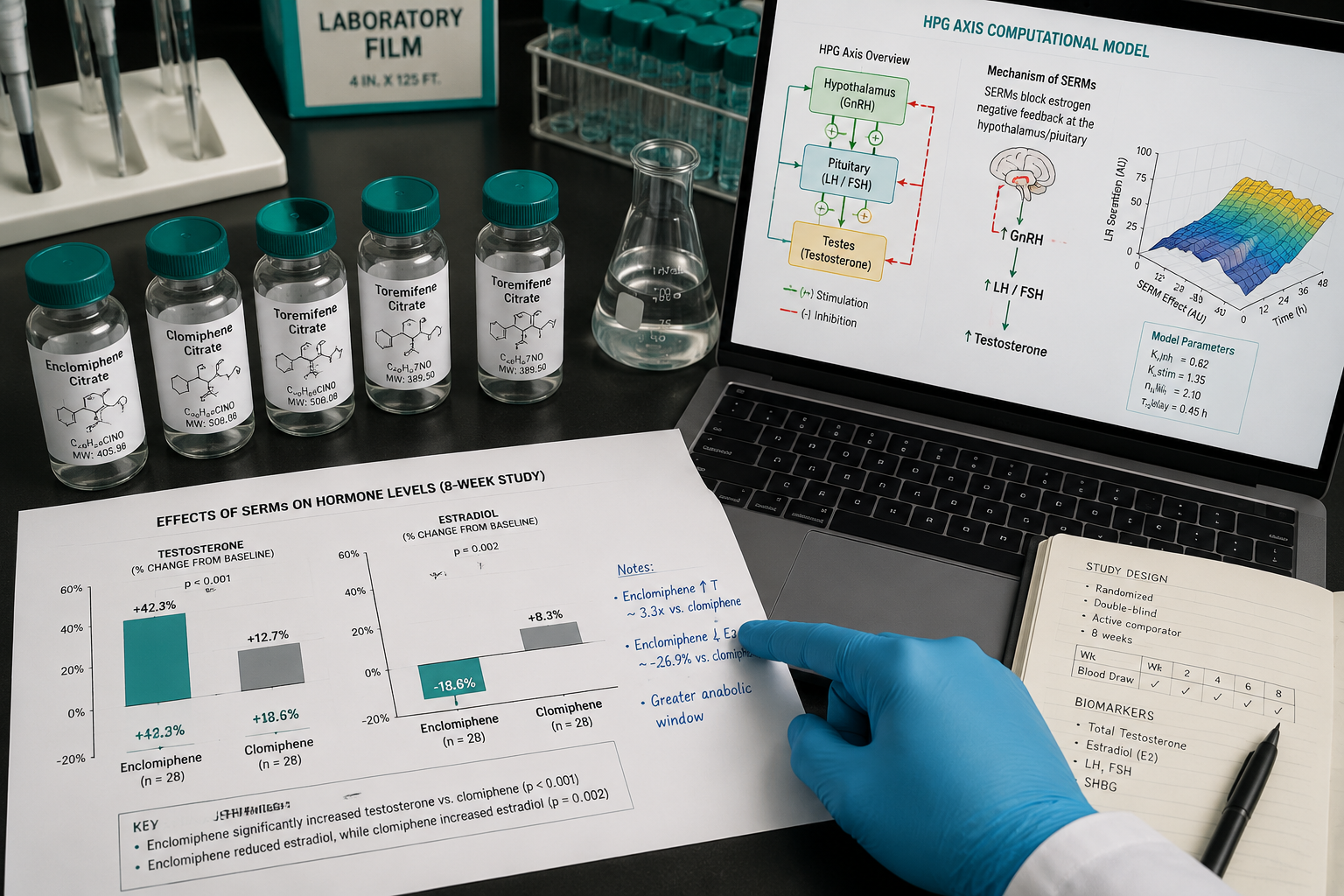
A retrospective study of 66 patients found that enclomiphene produced a median testosterone increase of 166 ng/dL with a statistically lower rise in estradiol compared to clomiphene. Adverse effects — including decreased libido, reduced energy, and mood changes — were significantly less frequent with enclomiphene.
Unlike exogenous TRT, which suppresses LH, FSH, and sperm production through negative feedback, enclomiphene maintains or improves sperm counts. This makes it a distinct research focus for hypogonadal men who may wish to preserve fertility.
Researchers exploring metabolic modulation research lines may find enclomiphene's downstream effects on body composition and energy metabolism worth examining alongside testosterone normalization data.
Compounds that modulate the HPG axis often intersect with broader metabolic pathways. For context on related peptide-based research tools, MOTS-c and metabolic flexibility research offers a parallel lens on mitochondrial and hormonal crosstalk.
Enclomiphene vs Clomiphene: Quick Comparison
| Feature | Enclomiphene | Clomiphene Citrate |
|---|---|---|
| Isomer composition | Trans only | Trans + cis (50:50) |
| Estrogenic activity | None | Mild (via zuclomiphene) |
| Half-life | ~10 hours | Longer (zuclomiphene accumulates) |
| LH/FSH stimulation | Strong | Moderate |
| Fertility preservation | Yes | Partial |
| Mood/visual side effects | Lower frequency | Higher frequency |
Researchers also studying neural and arousal pathways may find relevant context in PT-141 neural and metabolic research themes, as central neuroendocrine signaling connects testosterone regulation with broader behavioral physiology.
For those examining body composition outcomes alongside hormonal normalization, TESA body composition research themes and IPA muscle and fat research themes provide complementary data on how hormonal environments shape tissue-level outcomes.
Conclusion
The study of enclomiphene in male endocrine research: mechanism vs clomiphene and overlaps with luteinizing phase physiology clarifies a critical point: not all serms are equal, and isomer composition matters enormously. Enclomiphene's clean receptor blockade at the hypothalamus restores the natural LH-driven testosterone pathway without the estrogenic noise introduced by zuclomiphene.
Actionable next steps for researchers in 2026:
- Prioritize enclomiphene over mixed clomiphene in male HPG axis models to reduce confounding estrogenic variables.
- Examine LH pulsatility data alongside testosterone outcomes to map the full luteinizing phase overlap.
- Investigate enclomiphene's role in secondary hypogonadism models where upstream signaling — not testicular function — is the limiting factor.
- Cross-reference testosterone normalization data with metabolic and body composition endpoints for a more complete hormonal profile.
As regulatory and clinical interest in enclomiphene grows, its mechanistic clarity makes it a valuable tool for researchers who need precise, reproducible HPG axis modulation without the side-effect profile of its predecessor.