

PT-141 and Melanocortin Receptor Research: What Makes It Different From PDE5 Inhibitor Models?
Roughly one-third of adults who use PDE5 inhibitors for sexual dysfunction report an inadequate response — a gap that has pushed researchers toward entirely different receptor systems. PT-141 and melanocortin receptor research represents one of the most mechanistically distinct approaches in this field, operating through the central nervous system rather than peripheral vasculature. Understanding what makes this model different from PDE5 inhibitor frameworks requires a close look at receptor selectivity, downstream signaling, and the endpoints researchers use to measure outcomes.
Key Takeaways
- PT-141 (bremelanotide) acts centrally at MC3R and MC4R receptors in the brain, not on peripheral vascular tissue
- PDE5 inhibitors require intact nitric oxide signaling; PT-141 does not, making it effective in non-responders
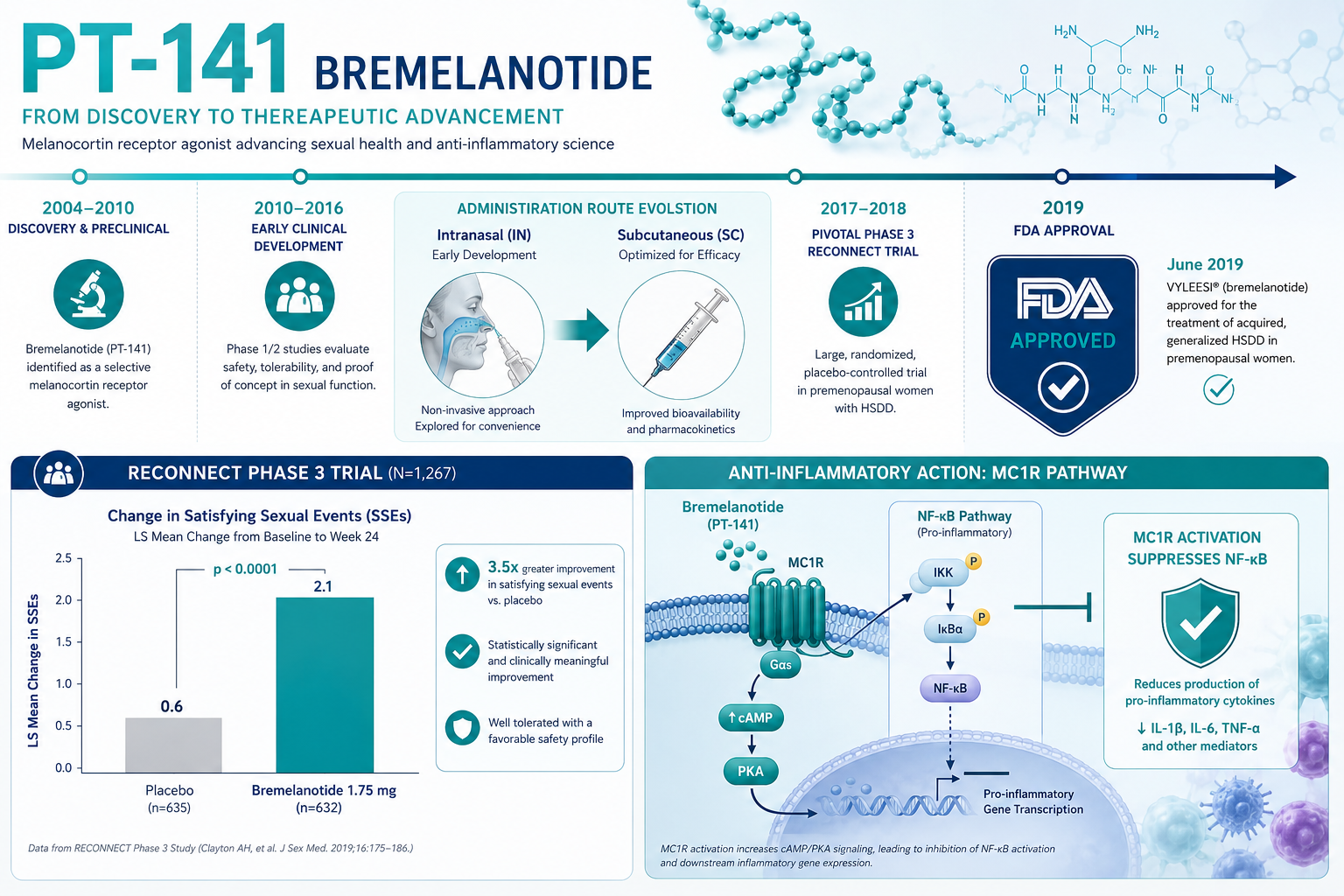
- The FDA approved bremelanotide (Vyleesi) in 2019 for hypoactive sexual desire disorder in premenopausal women
- Phase 3 RECONNECT trial data showed approximately 58% response rates versus 36% for placebo
- PT-141 also retains activity at MC1R, opening research into anti-inflammatory applications
The Central vs. Peripheral Distinction in PT-141 and Melanocortin Receptor Research
The most fundamental difference between PT-141 and PDE5 inhibitor models lies in where each compound acts in the body.
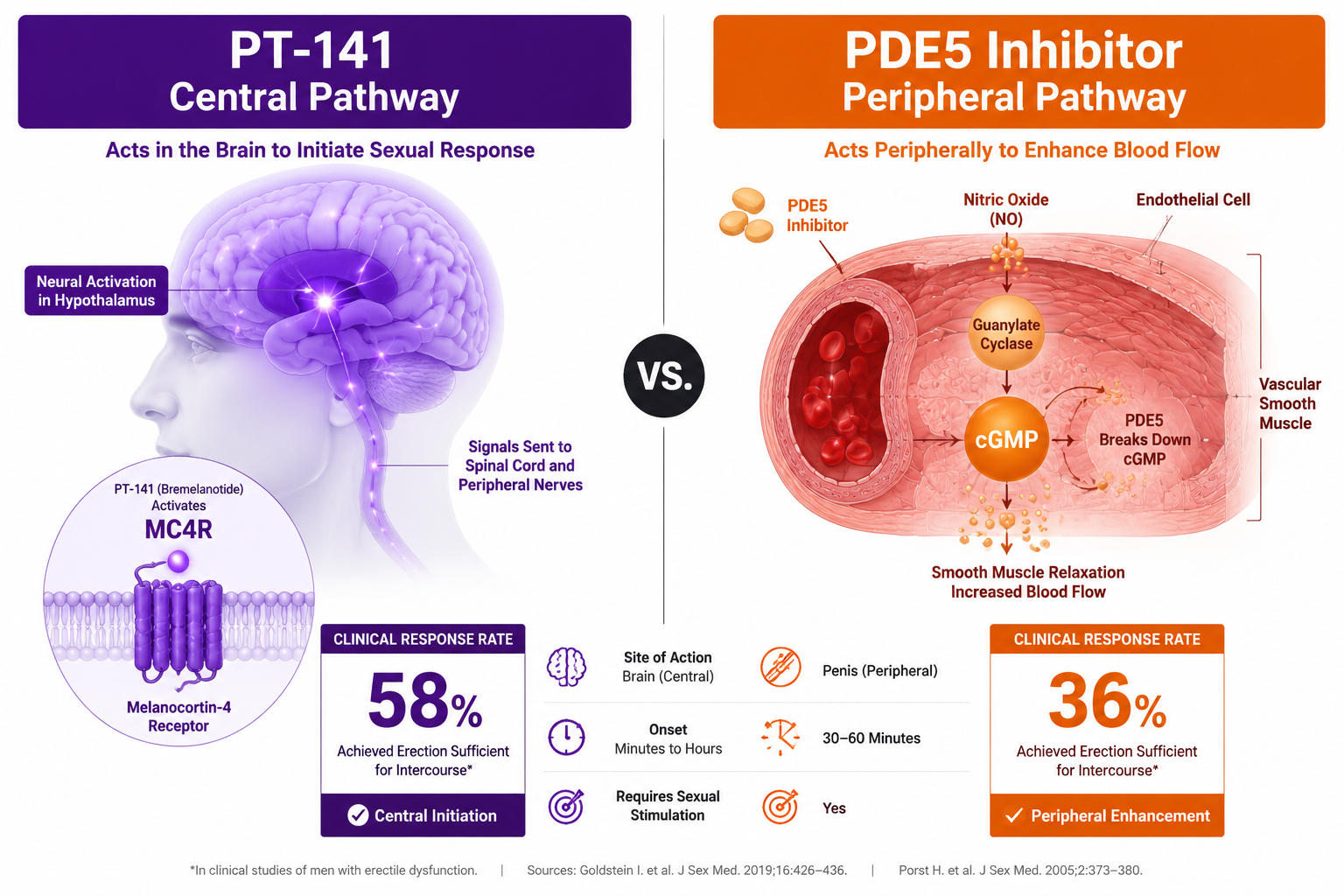
PDE5 inhibitors such as sildenafil work peripherally. They block the phosphodiesterase-5 enzyme in vascular smooth muscle, which prevents the breakdown of cyclic GMP (cGMP). This raises cGMP levels, relaxes smooth muscle, and increases blood flow to erectile tissue. The entire mechanism depends on intact nitric oxide (NO) signaling. If NO signaling is impaired — due to endothelial dysfunction, diabetes, or other vascular conditions — PDE5 inhibitors lose much of their effectiveness.
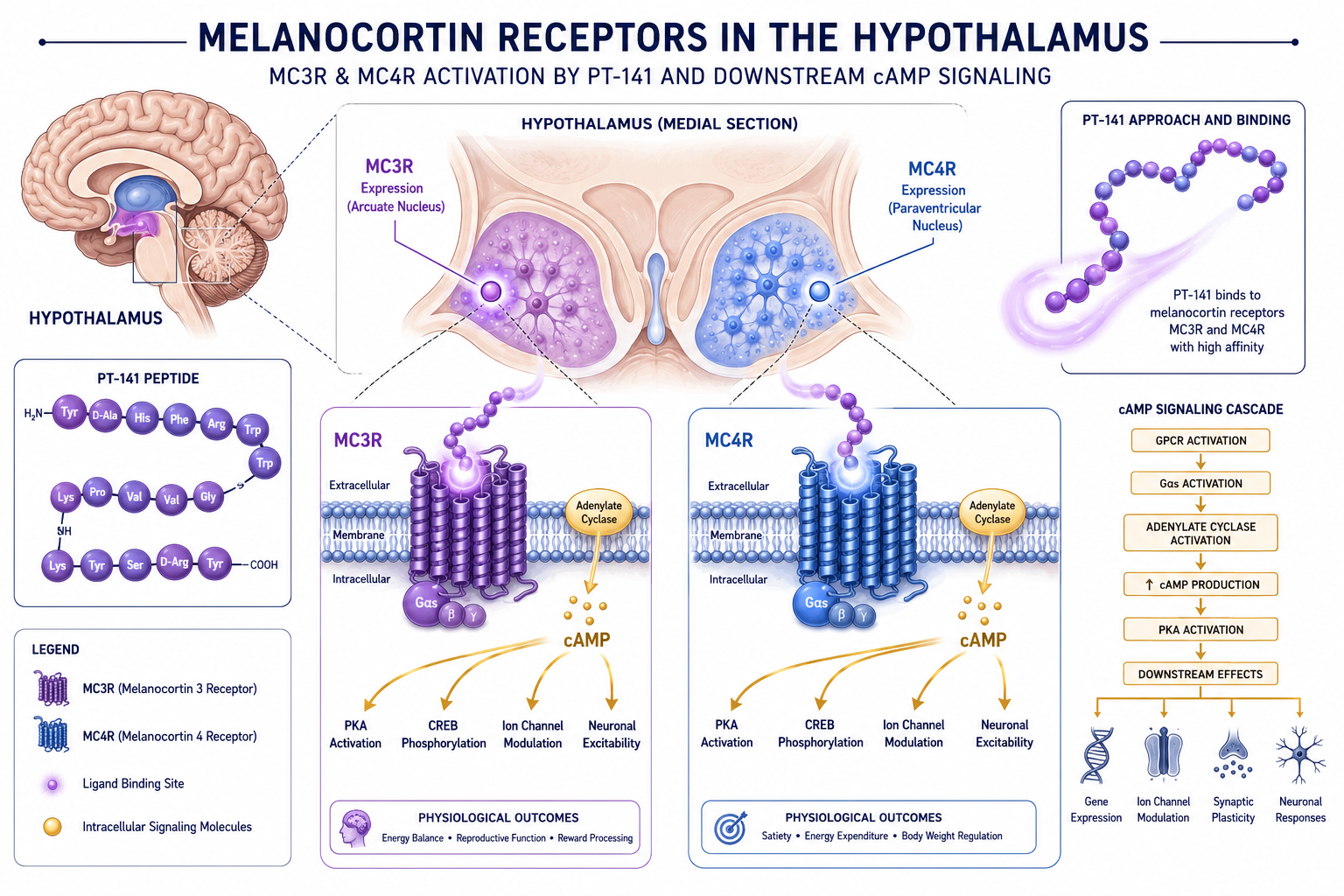
PT-141, by contrast, is a synthetic cyclic heptapeptide that acts as an agonist at melanocortin receptors, specifically MC3R and MC4R, within the central nervous system. These receptors are concentrated in the hypothalamus and other brain regions involved in sexual arousal and motivation. Activation of MC4R in particular triggers downstream cAMP-mediated signaling that initiates pro-erectile and pro-desire neural pathways without requiring peripheral vascular integrity.
"PT-141's central mechanism allows it to be effective in individuals who do not respond adequately to PDE5 inhibitors — a clinically meaningful distinction."
This is why early clinical studies found that PT-141 produced statistically significant erectile responses even in men who had previously shown inadequate responses to PDE5 inhibitor therapy. The two models are not competing — they are operating on entirely different physiological levels.
For researchers exploring other centrally acting or receptor-specific peptides, the longevity peptide research overview provides useful context on how receptor selectivity shapes research design across multiple peptide classes.
Receptor Selectivity, Pharmacokinetics, and Research Endpoints
Melanocortin Receptor Subtypes and Selectivity
The melanocortin system includes five receptor subtypes (MC1R through MC5R). PT-141's research profile is shaped largely by its activity at three of these:
| Receptor | Primary Location | Research Relevance |
|---|---|---|
| MC1R | Peripheral immune cells, skin | Anti-inflammatory signaling, NF-kB suppression |
| MC3R | Hypothalamus, limbic system | Sexual arousal modulation |
| MC4R | Hypothalamus, brainstem | Pro-erectile signaling, energy regulation |
This multi-receptor profile makes PT-141 and melanocortin receptor research broader in scope than PDE5 inhibitor models, which are largely limited to vascular endpoints.
Pharmacokinetics
Bremelanotide is administered subcutaneously. Peak plasma concentrations occur within approximately one hour post-injection, with a plasma half-life of roughly two hours. Hepatic metabolism is the primary elimination pathway. Earlier development programs evaluated intranasal delivery, but the subcutaneous route was selected for the registered product due to more controlled pharmacokinetic exposure and a more acceptable cardiovascular profile.
Preclinical and Clinical Endpoints
Researchers studying PT-141 use endpoints that differ substantially from PDE5 inhibitor trials:
- Central arousal measures: Changes in desire and motivation scores, not just physiological response
- Satisfying sexual events (SSEs): The primary endpoint in HSDD trials
- Female Sexual Distress Scale (FSDS): Validated patient-reported outcome used in RECONNECT Phase 3 trials
- Non-vascular erectile response: Penile tumescence in the absence of visual stimulation
The RECONNECT Phase 3 program reported approximately 58% response rates for bremelanotide versus 36% for placebo in premenopausal women with HSDD — a meaningful separation that led to FDA approval in June 2019 under the trade name Vyleesi.
For comparison, researchers interested in metabolic peptide endpoints may find the AOD-9604 metabolic research overview a useful reference for how endpoint selection varies across peptide categories.
Broader Research Applications and What Makes This Model Unique
Anti-Inflammatory Research Through MC1R
One dimension that separates PT-141 and melanocortin receptor research from PDE5 inhibitor models is the anti-inflammatory potential. PT-141 retains partial agonist activity at MC1R, which is expressed on macrophages, monocytes, and other immune cells. MC1R activation suppresses NF-kB signaling and reduces pro-inflammatory cytokine release. This has prompted preclinical investigations into PT-141's potential utility in hemorrhagic shock and ischemia-reperfusion injury — areas entirely outside the scope of PDE5 inhibitor research.
Safety Profile Compared to PDE5 Inhibitors
The most commonly reported adverse events with PT-141 are flushing and nausea, both typically transient. Importantly, research data show no significant changes in vital signs, ECG readings, laboratory values, or physical examination findings at therapeutic doses. PDE5 inhibitors, by contrast, carry risks related to systemic vasodilation, including hypotension when combined with nitrates — a contraindication that does not apply to PT-141.
Researchers sourcing peptides for study should review quality testing protocols to ensure compound integrity before any preclinical work. Those specifically looking for verified compounds can explore PT-141 peptide for sale and PT-141 research options through tested suppliers.
For researchers comparing receptor-targeted peptide mechanisms across different physiological systems, the GLP-1 dual receptor agonism breakdown offers a parallel example of how multi-receptor engagement shapes research design and clinical endpoints.
Conclusion
PT-141 and melanocortin receptor research occupies a distinct mechanistic space that PDE5 inhibitor models simply cannot address. By targeting MC3R and MC4R centrally, PT-141 bypasses the peripheral vascular requirements that limit sildenafil and related compounds. Its multi-receptor activity — spanning sexual function, energy signaling, and anti-inflammatory pathways — makes it a uniquely versatile subject for preclinical and clinical investigation.
Actionable next steps for researchers in 2026:
- Review the RECONNECT Phase 3 trial data to understand validated endpoints for HSDD research
- Compare melanocortin receptor subtype selectivity profiles when designing preclinical models
- Source only lab-tested, verified PT-141 compounds — see lab-tested peptides for verified options
- Consider MC1R anti-inflammatory endpoints as secondary outcomes in broader research protocols
- Distinguish clearly between central arousal endpoints and peripheral vascular endpoints when designing study protocols