
Enclomiphene for Research: Understanding its Mechanism in Hormone Regulation Studies
Fewer than 15% of men diagnosed with secondary hypogonadism have access to treatments that raise testosterone without shutting down sperm production — a gap that makes enclomiphene for research: understanding its mechanism in hormone regulation studies one of the most actively pursued topics in endocrinology today. As a selective estrogen receptor modulator (serm) with a uniquely targeted action on the hypothalamic-pituitary-gonadal (HPG) axis, enclomiphene has drawn significant scientific attention for its ability to restore hormonal balance through the body's own signaling pathways.
Key Takeaways
- Enclomiphene blocks hypothalamic estrogen receptors, triggering a natural cascade of LH, FSH, and testosterone production.
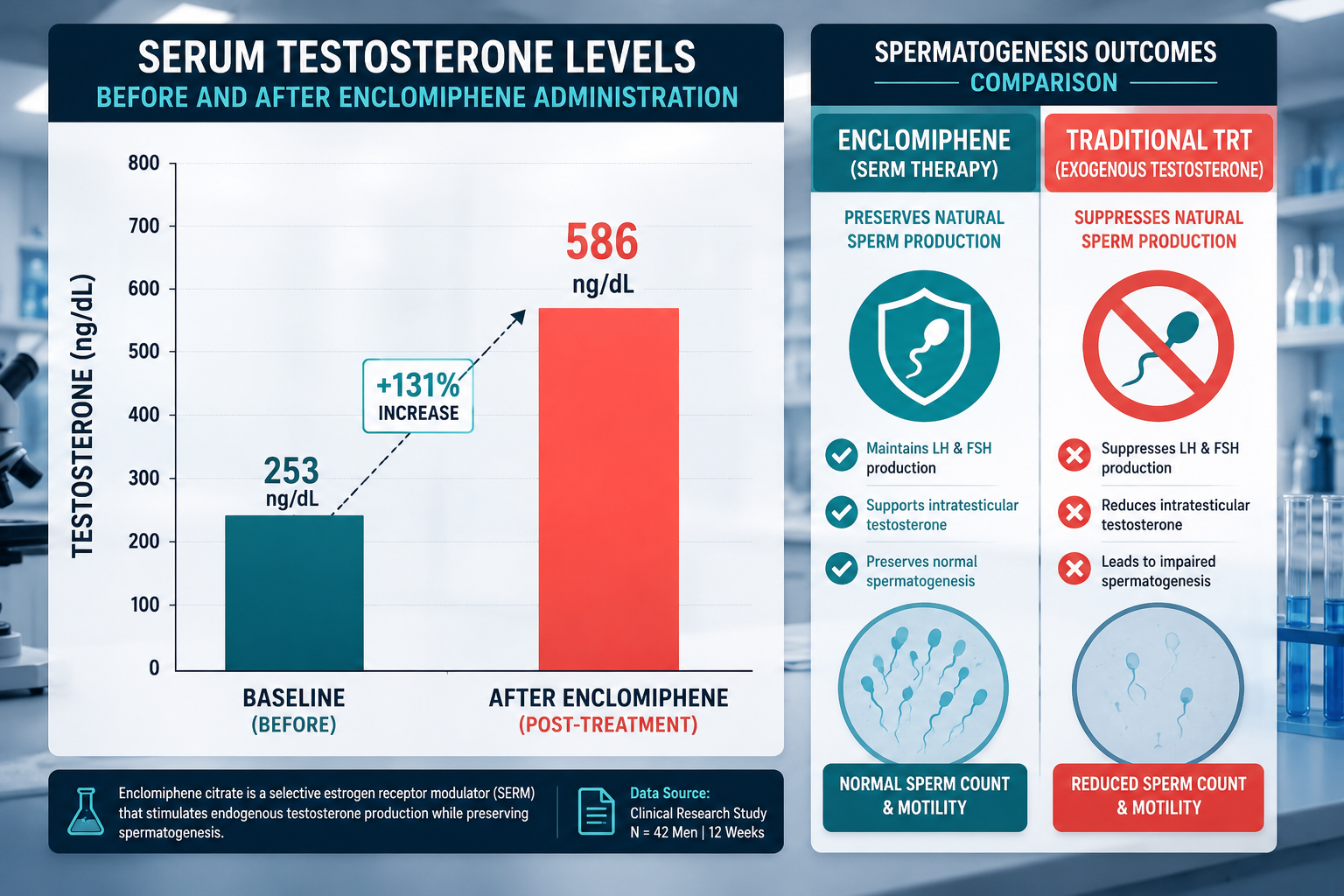
- Unlike testosterone replacement therapy (TRT), enclomiphene preserves spermatogenesis, making it valuable in fertility-focused research.
- Clinical data show testosterone levels rising from roughly 253 ng/dL to 586 ng/dL after six weeks at higher doses.
- Enclomiphene is the isolated trans-isomer of clomiphene, offering a cleaner serm profile with fewer estrogenic side effects.
- As of 2026, enclomiphene has not received FDA approval, and long-term safety data remain limited.
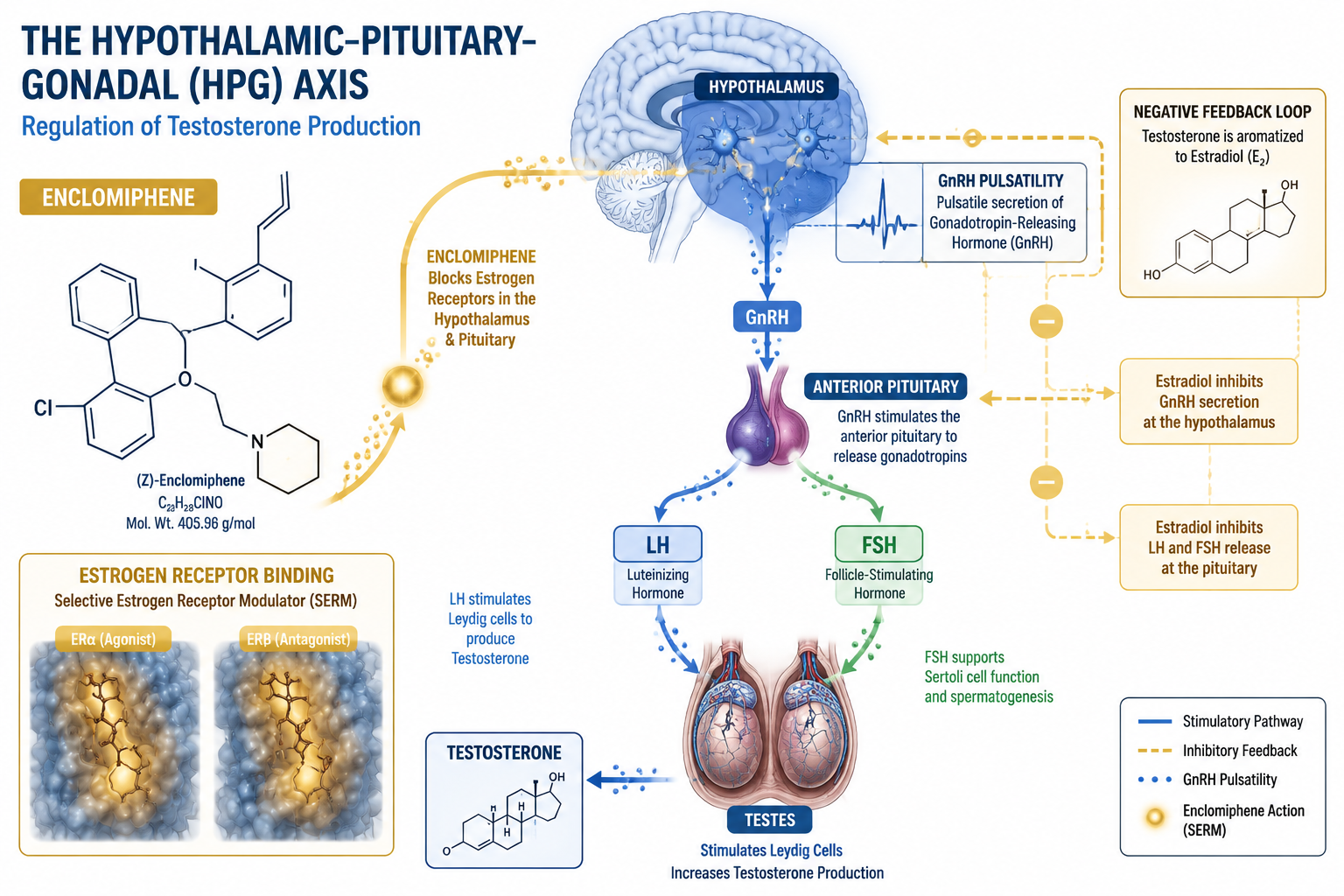
How Enclomiphene Works: The HPG Axis Mechanism
At the core of enclomiphene for research: understanding its mechanism in hormone regulation studies is its precise action on the HPG axis. Enclomiphene functions as a serm by competitively binding to estrogen receptors in the hypothalamus. Under normal conditions, circulating estradiol binds to these receptors and signals the hypothalamus to reduce gonadotropin-releasing hormone (GnRH) secretion — a classic negative feedback loop.
By blocking this feedback, enclomiphene removes the "brake" on GnRH pulsatility. The result is a downstream surge in both luteinizing hormone (LH) and follicle-stimulating hormone (FSH) from the anterior pituitary, which in turn stimulates Leydig cells in the testes to produce endogenous testosterone.
"Enclomiphene essentially resets the hormonal thermostat by working upstream rather than adding exogenous hormone."
This mechanism stands in sharp contrast to traditional TRT, which suppresses the HPG axis entirely. Researchers studying gonadorelin and GnRH pulsatility will find enclomiphene's upstream action particularly relevant, as both compounds engage the same signaling architecture.
Key receptor interactions in enclomiphene's mechanism:
| Site | Action | Downstream Effect |
|---|---|---|
| Hypothalamus | Blocks estrogen receptor | Increases GnRH pulsatility |
| Anterior pituitary | Elevated GnRH input | Raises LH and FSH output |
| Testes (Leydig cells) | LH stimulation | Boosts endogenous testosterone |
| Testes (Sertoli cells) | FSH stimulation | Preserves spermatogenesis |
Clinical Research Findings and Fertility Preservation
The practical value of enclomiphene for research: understanding its mechanism in hormone regulation studies becomes clearest when examining clinical trial data. In one well-cited trial, men with secondary hypogonadism who had baseline testosterone levels averaging 253 ng/dL reached an average of 586 ng/dL after six weeks on the highest tested dose. This restoration to normal physiological range without exogenous hormone administration is a significant research milestone.
What makes this especially notable for researchers:
- Sperm counts remained stable or improved, unlike outcomes seen with TRT
- LH and FSH levels rose proportionally, confirming HPG axis engagement
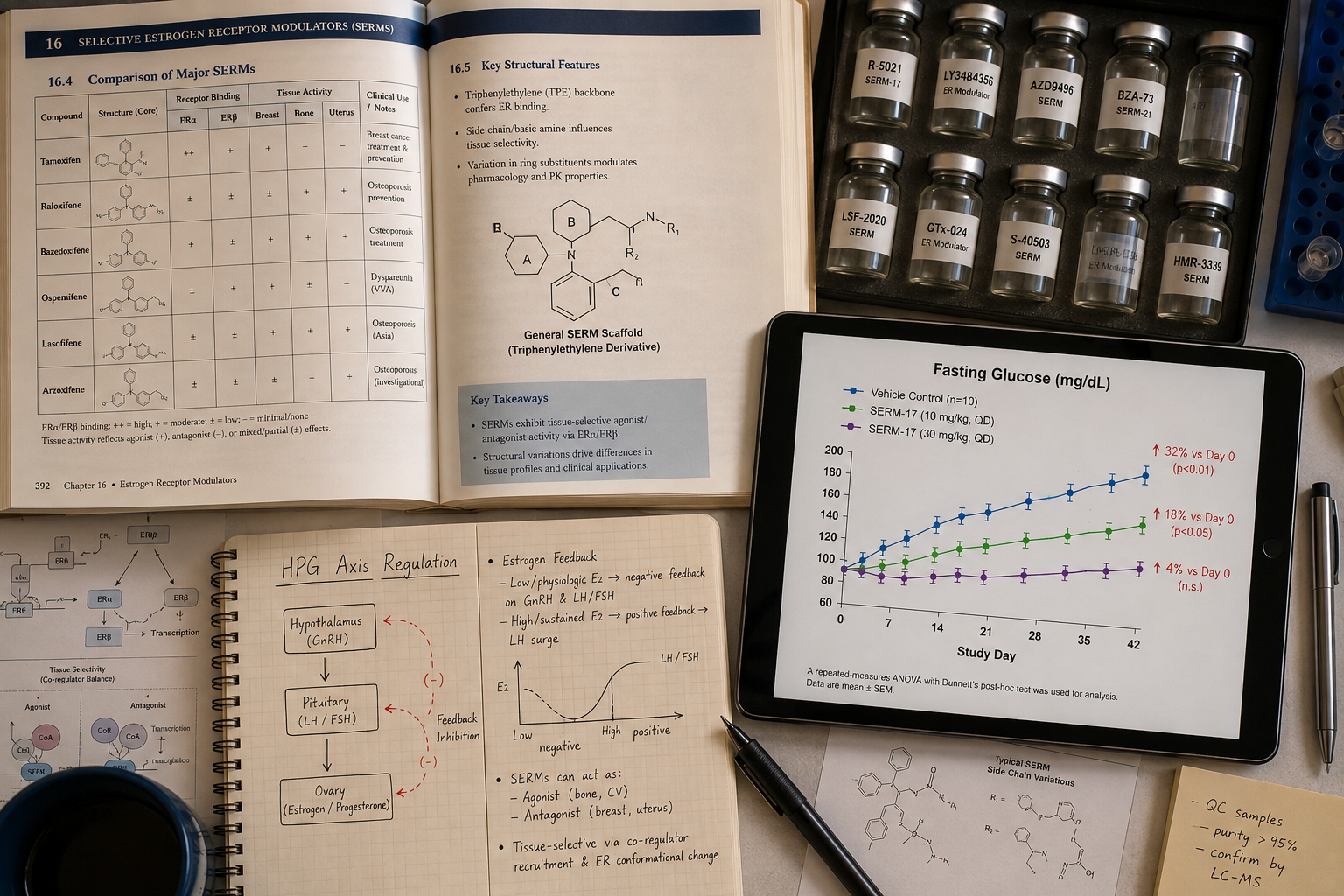
- Some participants showed improvements in fasting plasma glucose, suggesting potential metabolic benefits worth investigating further
This fertility-preserving profile makes enclomiphene a subject of interest in studies that also examine IPA serm stack research, where multiple compounds are evaluated for their combined effects on the endocrine system.
Enclomiphene vs. Clomiphene: A Cleaner Research Tool
Enclomiphene is the trans-isomer of clomiphene citrate. Standard clomiphene contains both the enclomiphene (trans) and zuclomiphene (cis) isomers. The zuclomiphene isomer carries weak estrogenic activity that can contribute to unwanted side effects. By isolating enclomiphene, researchers work with a compound that delivers a more targeted serm effect, reducing confounding variables in hormone regulation studies.
For labs exploring broader endocrine research, this specificity pairs well with investigations into longevity peptide research and metabolic hormone modulation.
Research Applications, Dosing Context, and Regulatory Landscape
Standard dosing protocols in research settings typically range from 12.5 mg to 25 mg orally once daily, with adjustments guided by serum testosterone and gonadotropin measurements. Short-term safety data have been satisfactory and broadly comparable to testosterone gels and placebo in controlled settings. However, long-term safety data remain limited — a critical gap that researchers are actively working to address.
As of 2026, enclomiphene has not received FDA approval. Regulatory reviewers have indicated that raising testosterone levels alone may not constitute sufficient clinical benefit without demonstrated symptomatic improvement. This regulatory context shapes how enclomiphene is sourced and studied; it is currently available through compounding pharmacies, which means quality and dosing consistency can vary.
Researchers investigating related hormonal compounds may find useful context in NAD research and metabolic regulation and thymosin alpha-1 mechanism studies, both of which intersect with endocrine health pathways. For those reviewing the latest developments across the field, the peptide research blog provides ongoing updates relevant to serm and hormone regulation research.
Expert consensus points toward placebo-controlled, randomized trials as the next necessary step — particularly for populations with obesity, metabolic syndrome, and infertility-related hypogonadism.
Conclusion
Enclomiphene occupies a distinctive position in hormone regulation research because it works with the body's own feedback architecture rather than bypassing it. Its ability to elevate endogenous testosterone while preserving spermatogenesis addresses a genuine gap in the endocrinology research toolkit. For investigators studying the HPG axis, serm pharmacology, or fertility-adjacent hormone therapies, the compound offers a well-characterized mechanism and a growing clinical evidence base.
Actionable next steps for researchers:
- Review existing clinical trial data on HPG axis modulation to establish baseline comparisons.
- Prioritize sourcing from suppliers with verified testing protocols to ensure compound purity.
- Design studies that measure symptomatic outcomes alongside biomarker changes to address the FDA's stated evidentiary concerns.
- Consider pairing enclomiphene studies with metabolic markers, given preliminary data on fasting glucose improvements.
- Monitor regulatory developments in 2026, as the approval landscape for serms in hypogonadism continues to evolve.