GLP-3 Retatrutide vs. GLP-1 and GLP-2: Understanding Receptor Specificity and Research Models
A 39-amino acid peptide achieving 28.7% body weight reduction in preliminary Phase 3 data is not a minor incremental advance — it signals a fundamental shift in how researchers think about metabolic receptor targeting. At the center of this shift is retatrutide, often labeled "GLP-3" in research shorthand, and understanding GLP-3 Retatrutide vs. GLP-1 and GLP-2: Understanding Receptor Specificity and Research Models is now essential for anyone following the metabolic peptide research landscape in 2026.
Key Takeaways
- Retatrutide simultaneously activates three receptors: GLP-1, GIP, and glucagon — unlike GLP-1 or GLP-2 single-agonist peptides.
- Its receptor potency profile is uneven by design, with the GIP receptor showing the highest binding affinity.
- Triple-receptor activation addresses both sides of energy balance: reducing caloric intake and increasing energy expenditure.
- Retatrutide remains investigational as of 2026, with Phase 3 trials ongoing and FDA filing projected for 2026-2027.
- Structural modifications including a C20 fatty diacid moiety enable once-weekly dosing through extended half-life.
How Receptor Specificity Defines the GLP-3 Retatrutide vs. GLP-1 and GLP-2 Distinction
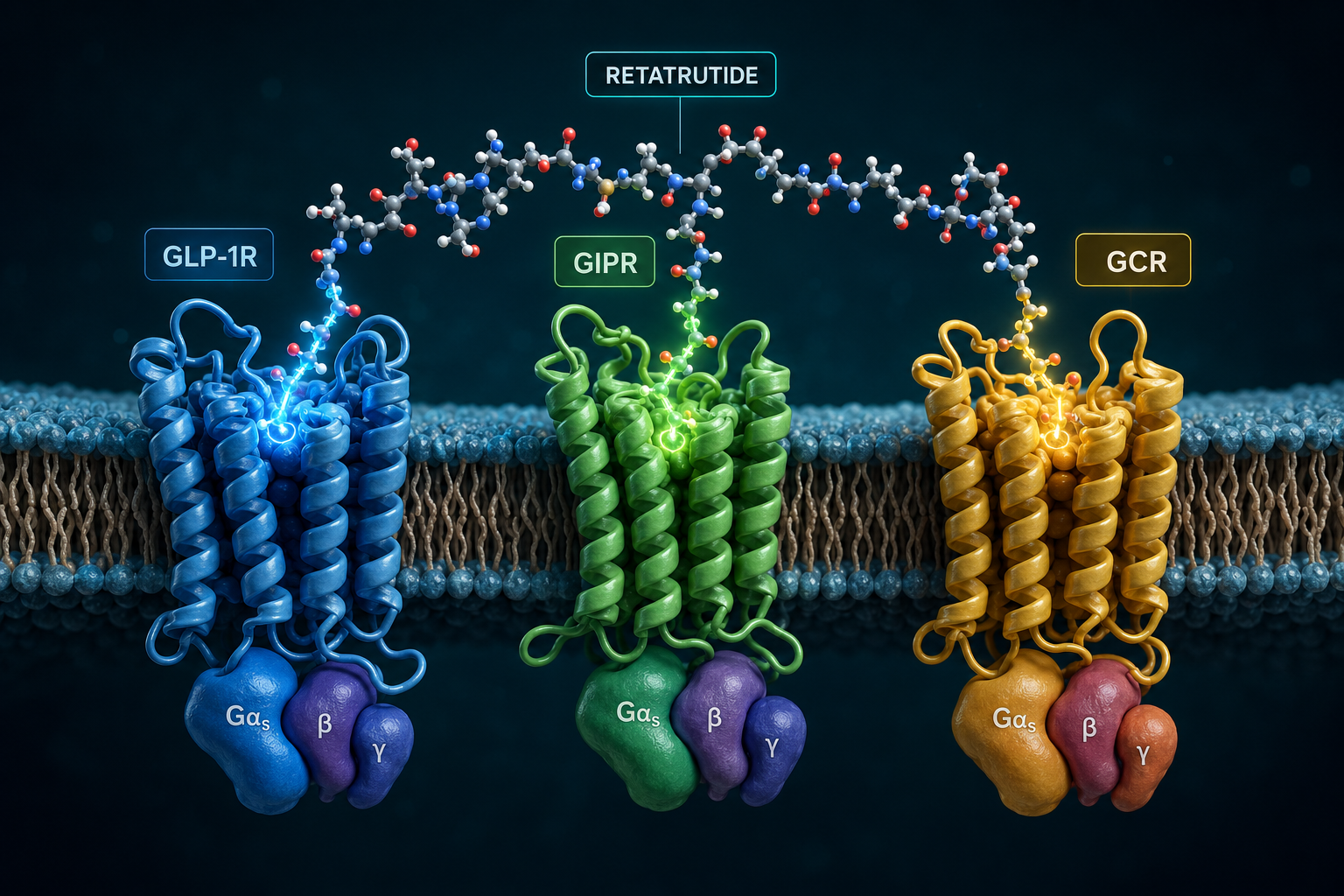
The term "GLP-3" is a colloquial label used in research communities to distinguish retatrutide from earlier incretin-based compounds. Formally, retatrutide is a triple agonist — it binds and activates the GLP-1 receptor, the GIP receptor, and the glucagon receptor. This is categorically different from GLP-1 receptor agonists like semaglutide, which target a single receptor, and from GLP-2, a peptide primarily involved in intestinal growth and repair through its own dedicated receptor.
Understanding the receptor specificity comparison requires looking at potency data:
| Receptor | EC50 Value | Relative Potency vs. Native Peptide |
|---|---|---|
| GIP Receptor | 0.0643 nM | ~8.9x more potent than native GIP |
| GLP-1 Receptor | 0.775 nM | ~0.4x potency of native GLP-1 |
| Glucagon Receptor | 5.79 nM | ~0.3x potency of native glucagon |
This asymmetric potency profile is intentional. The GIP receptor is activated most strongly, while glucagon receptor engagement is kept moderate — enough to drive thermogenesis and fat mobilization without triggering hyperglycemia. GLP-1 receptor activation suppresses appetite and enhances insulin secretion, while GLP-2 operates on an entirely separate pathway focused on gut mucosal integrity, making it functionally distinct from retatrutide's mechanism.
For researchers exploring incretin biology, the GLP-3 incretin research themes page provides a useful foundation for understanding how this triple-agonist model differs from classic GLP-1 frameworks.
Downstream Signaling Pathways: Where GLP-3 Retatrutide vs. GLP-1 and GLP-2 Research Models Diverge
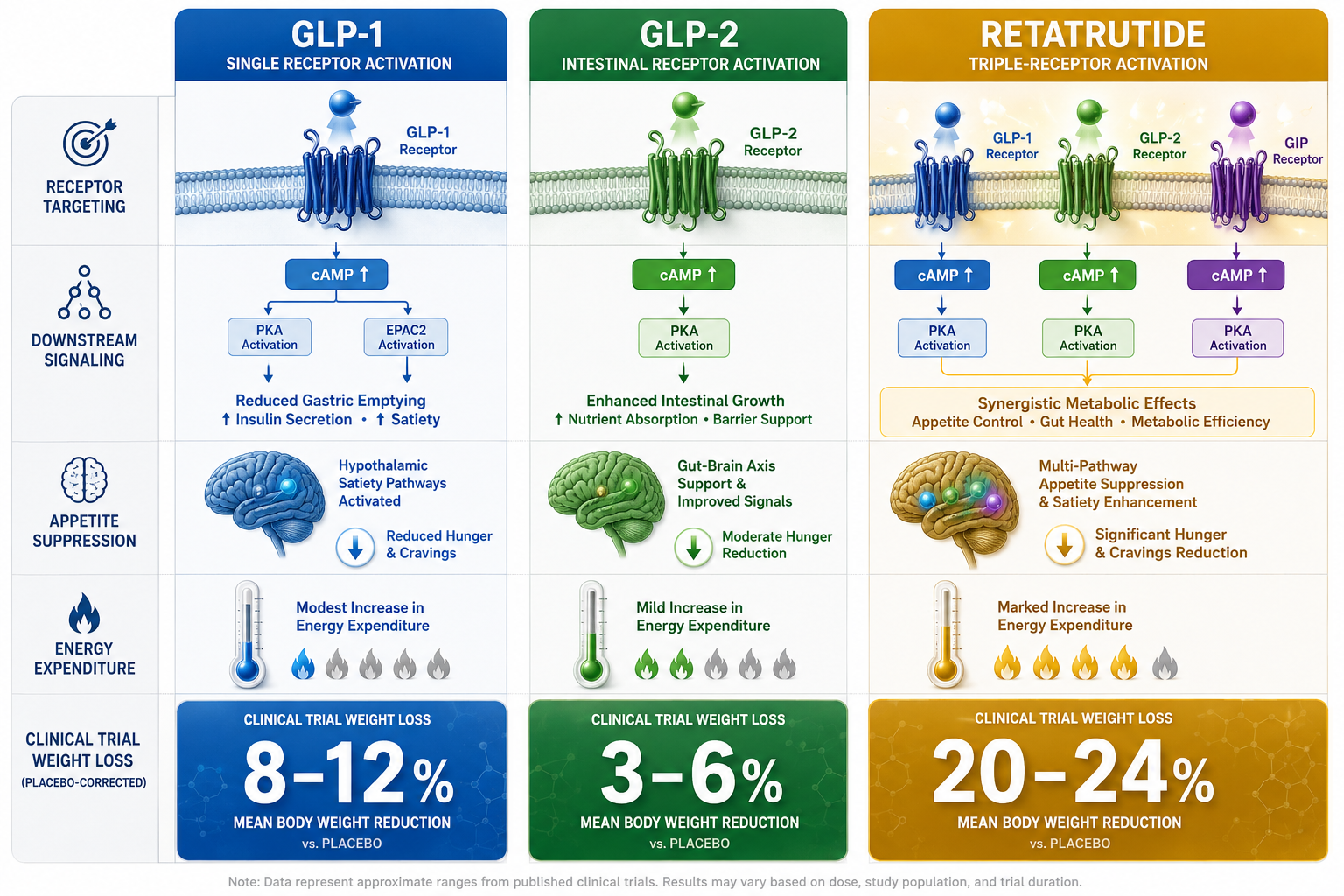
The downstream effects of receptor activation explain why retatrutide produces outcomes that single-agonist peptides cannot replicate. Each receptor pathway contributes a distinct physiological signal:
- GLP-1 receptor activation: Slows gastric emptying, reduces appetite via central nervous system signaling, and stimulates glucose-dependent insulin release.
- GIP receptor activation: Enhances insulin secretion, may improve insulin sensitivity, and contributes to adipose tissue regulation.
- Glucagon receptor activation: Increases hepatic glucose output at low levels, but more critically at therapeutic doses, drives thermogenesis and promotes lipolysis.
GLP-2, by contrast, signals primarily through receptors in the intestinal epithelium, stimulating mucosal growth and nutrient absorption. Its downstream effects are largely confined to the gut, with no meaningful overlap with the metabolic energy-balance pathways that retatrutide engages.
This divergence has significant implications for research model design. Studies examining retatrutide must account for simultaneous multi-receptor crosstalk, whereas GLP-1 or GLP-2 models involve cleaner, more isolated signaling environments. Researchers interested in how GIP receptor dynamics fit into this picture can explore the GIP receptor and its importance for additional context.
Those comparing generational differences in GLP-1 compounds may also find value in reviewing generations of GLP-1 differences to place retatrutide's design within a broader evolutionary framework of incretin drug development.
Clinical Research Outcomes and the Triple-Agonist Advantage
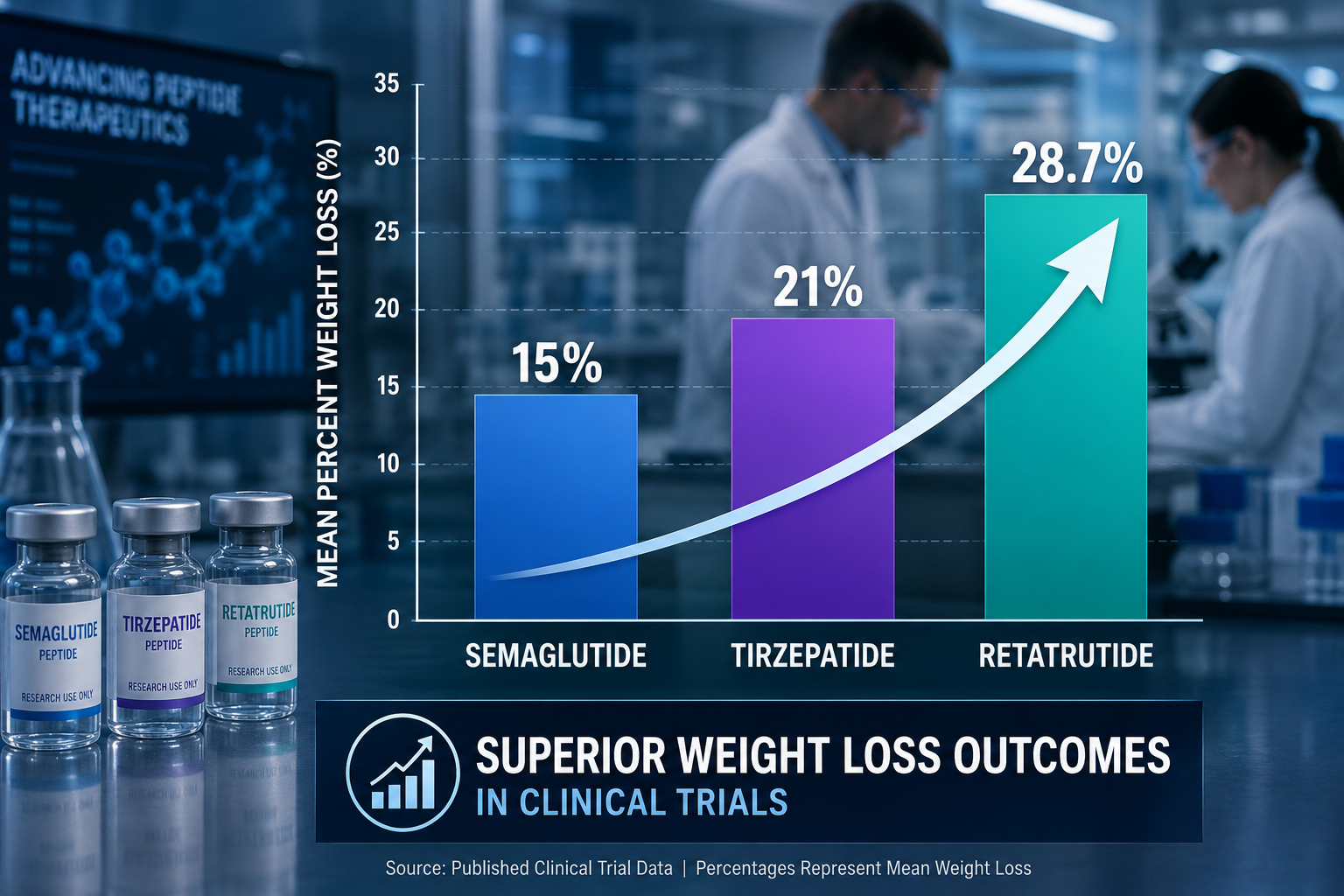
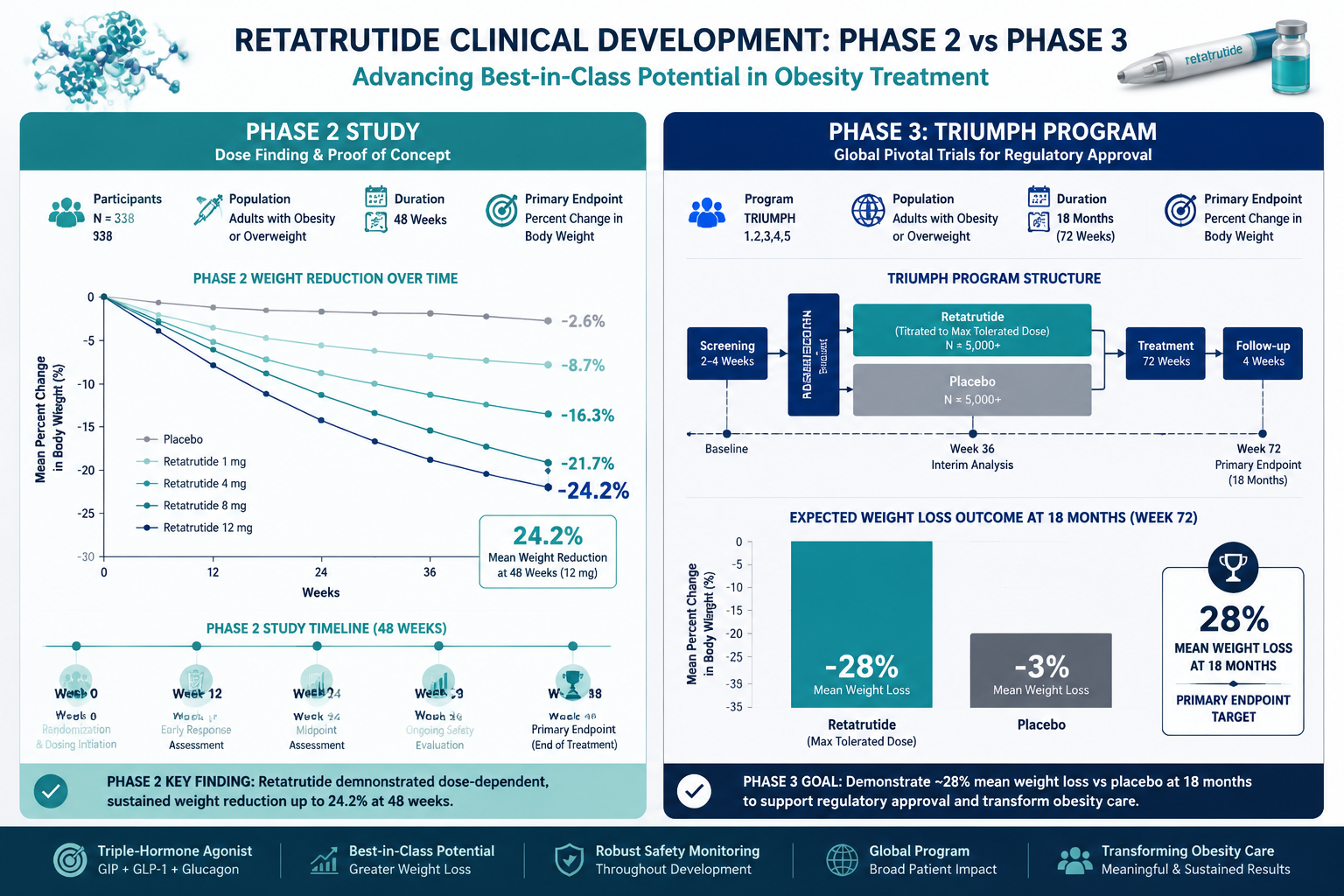
The clinical data emerging from retatrutide trials reflects the compounded benefit of triple-receptor engagement. Phase 2 results showed up to 24.2% body weight reduction over 48 weeks. Preliminary Phase 3 data pushes that figure to 28.7% at 68 weeks — a result that exceeds outcomes from both semaglutide and tirzepatide in comparable timeframes.
Structurally, retatrutide is built on a GIP peptide backbone, modified with 2-aminoisobutyric acid (Aib) residues and a C20 fatty diacid moiety. These modifications resist enzymatic degradation and extend the half-life to approximately six days, making once-weekly subcutaneous dosing feasible. Steady-state plasma concentrations are typically reached within four to five weeks of consistent administration.
As of 2026, retatrutide remains investigational. It has not received FDA approval and is available only in research and clinical trial contexts. An FDA filing is projected for 2026-2027 pending Phase 3 completion.
Researchers building multi-pathway metabolic models may also find it useful to examine how other compounds interact with energy regulation. The SLU-PP-332 metabolic modulation research themes page outlines complementary pathways that some researchers study alongside incretin-based models. Similarly, the GLP-1 peptide generational research concepts resource provides sourcing and conceptual context for GLP-1 receptor research.
For those specifically focused on retatrutide as a research compound, the GLP-3 triple agonist research planning page offers catalog navigation and planning guidance.
Conclusion
The comparison of GLP-3 Retatrutide vs. GLP-1 and GLP-2: Understanding Receptor Specificity and Research Models reveals a clear hierarchy of mechanistic complexity. GLP-2 operates in a gut-specific domain. GLP-1 agonists provide meaningful but single-pathway metabolic control. Retatrutide, through its calibrated triple-receptor engagement, addresses energy balance from multiple angles simultaneously — a design that its clinical outcomes appear to validate.
Actionable next steps for researchers:
- Review published Phase 2 and Phase 3 trial protocols to understand retatrutide's dosing and endpoint design before building research models.
- Map receptor crosstalk carefully when designing in vitro or preclinical studies involving triple agonists.
- Compare GIP receptor potency data against GLP-1 receptor data to understand which pathway dominates at different dose levels.
- Monitor FDA filing updates projected for 2026-2027 to track regulatory trajectory.
- Consult the GLP-3 newest triple agonist overview for updated research framing as new data emerges.