Retatrutide Clinical Trials: What Phase 3 Data Mean for Research-Only Readers
A single Phase 3 trial readout in December 2025 shifted the entire conversation around triple agonism: 28.7% mean weight loss at 68 weeks. That number, from the TRIUMPH-4 study of retatrutide, is not a projection or a preclinical estimate. It is human trial data, and it demands careful reading by anyone tracking metabolic research.
This article breaks down what those results mean, how the trial was designed, and why the data carry weight for researchers studying GIP/GLP-1/glucagon receptor pathways — while making clear that retatrutide remains strictly investigational in 2026.
Key Takeaways
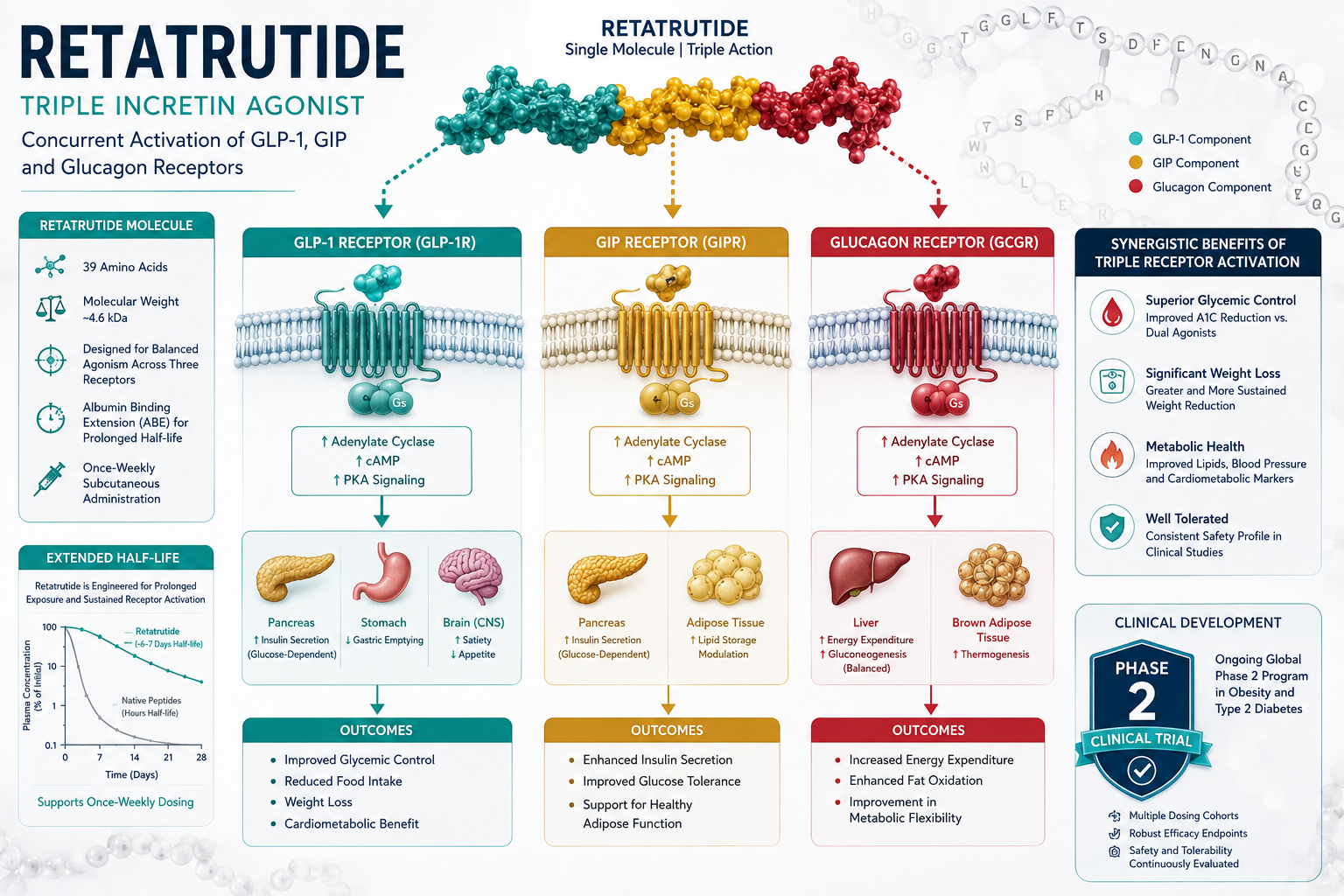
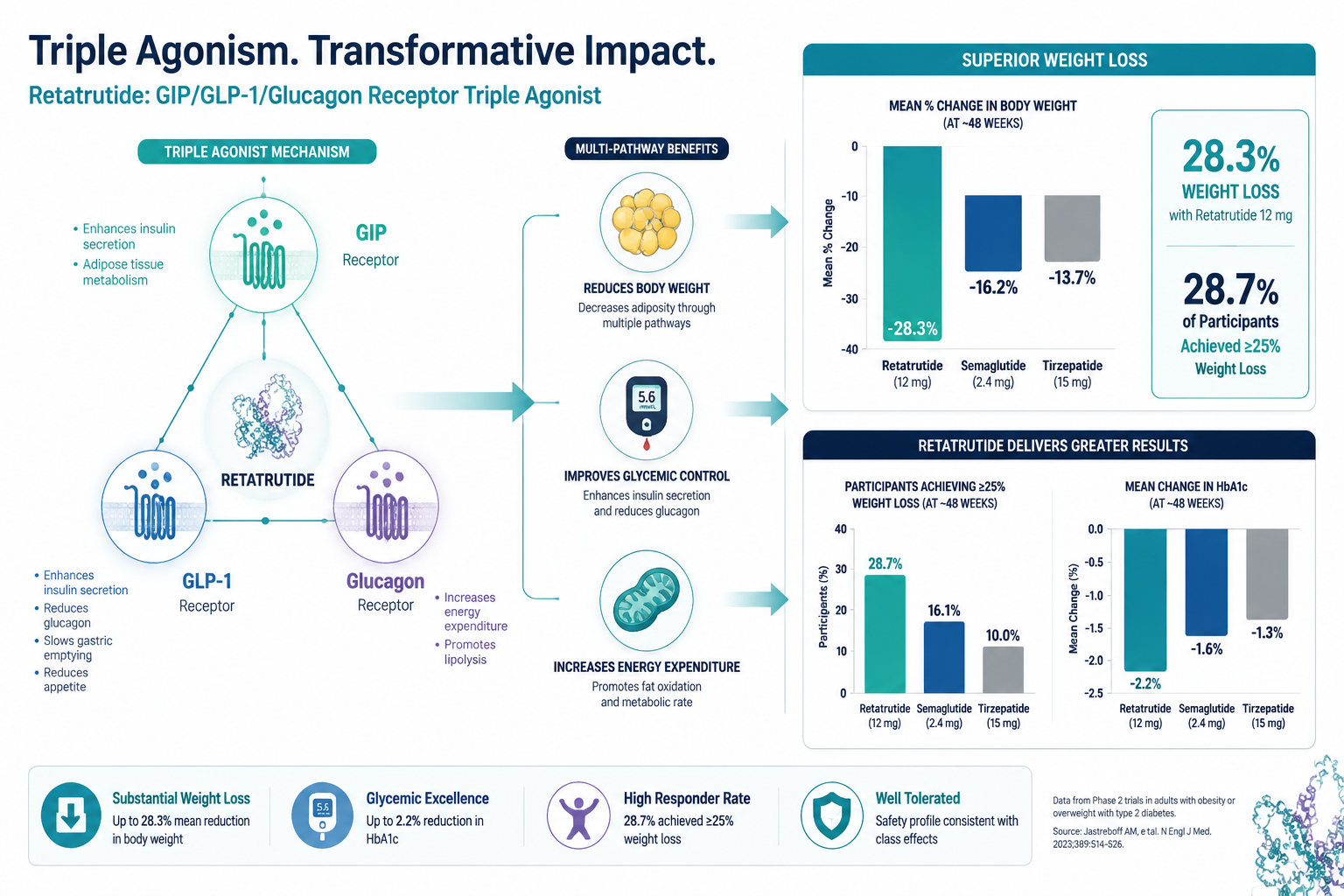
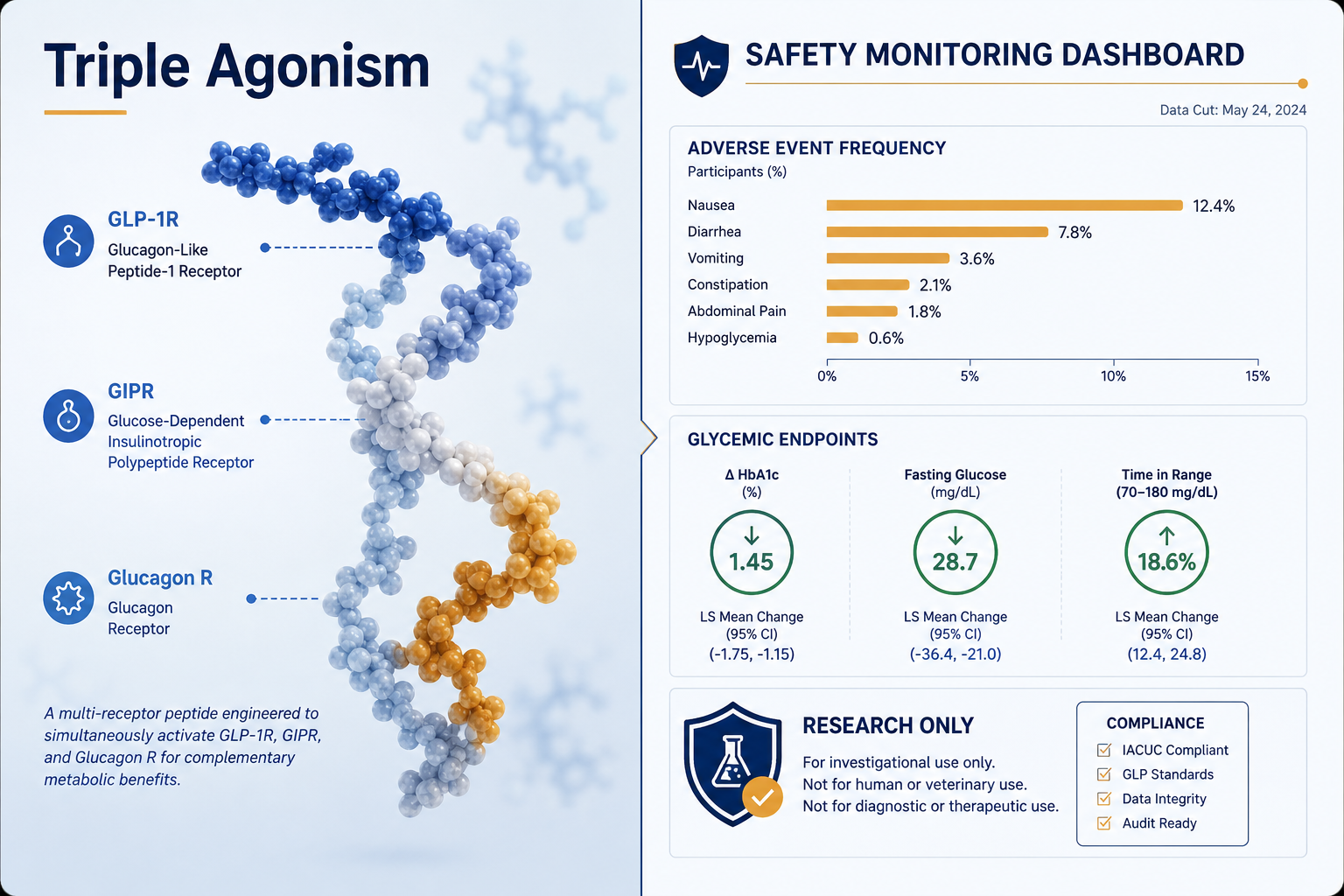
- Retatrutide (LY3437943) is a once-weekly triple agonist targeting GIP, GLP-1, and glucagon receptors, currently in Phase 3 trials with no regulatory approval anywhere as of 2026.
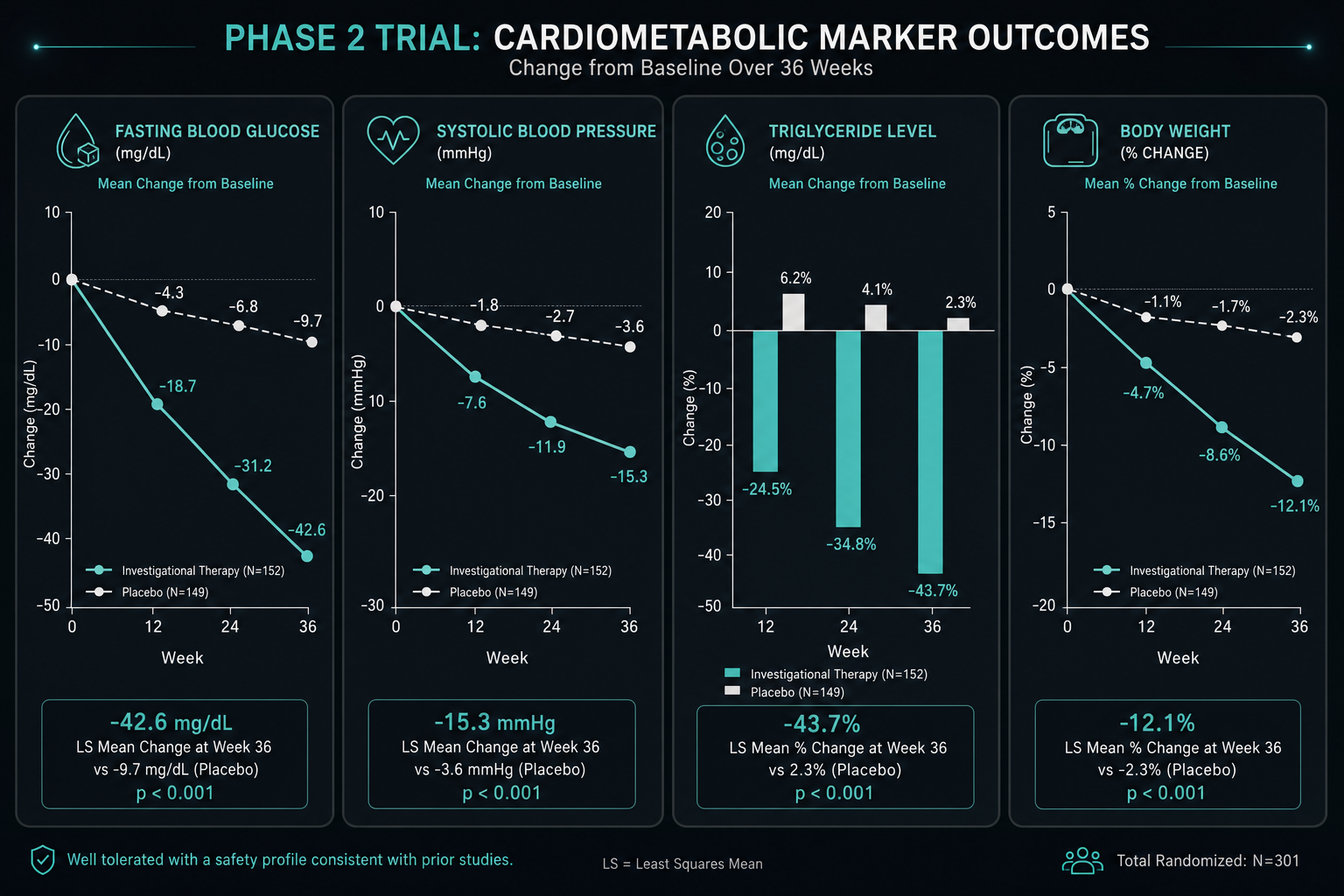
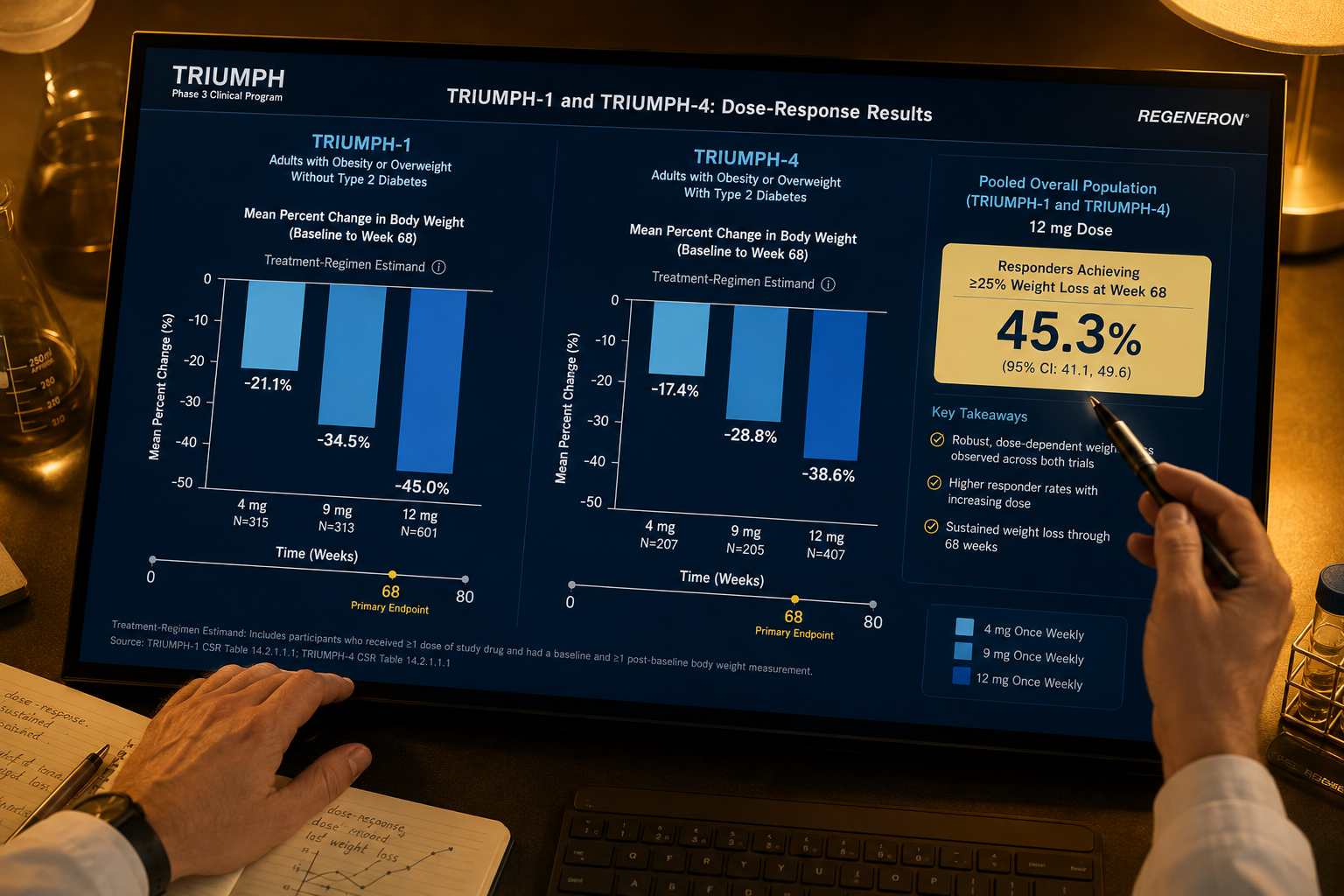
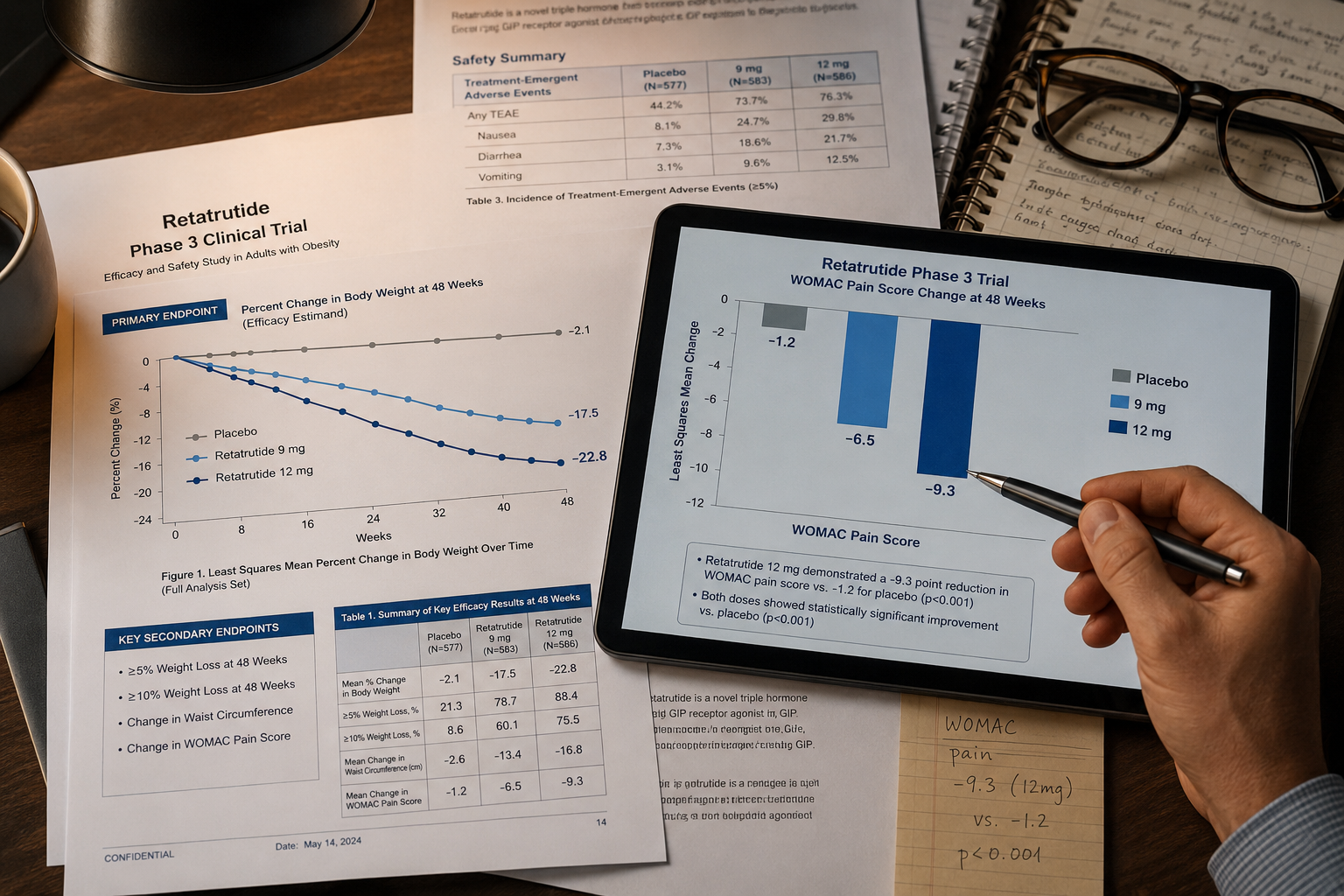
- TRIUMPH-4 reported 26.4% mean weight loss at 9 mg and 28.7% at 12 mg over 68 weeks, versus 2.1% on placebo.
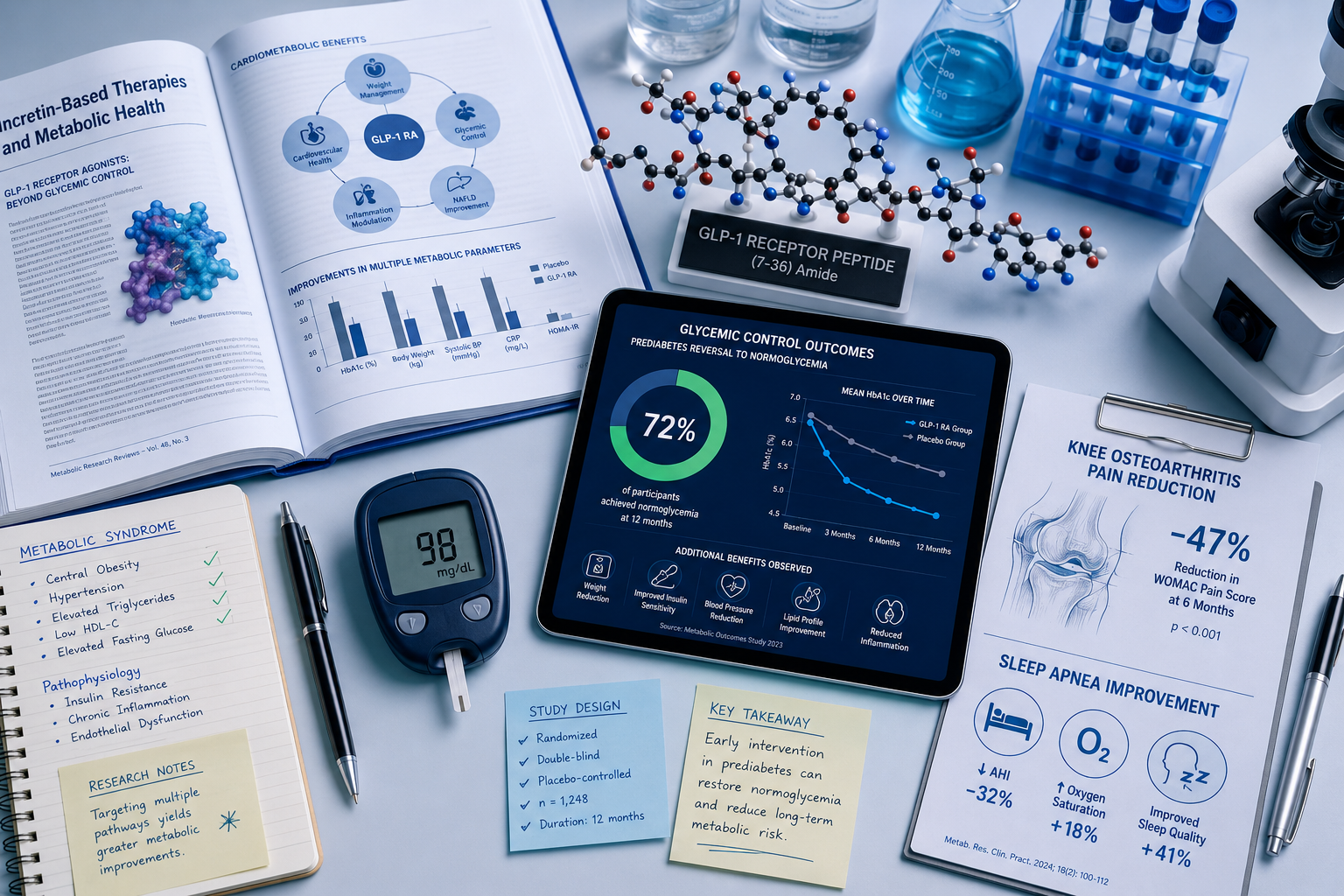
- Secondary endpoints included a 75.8% reduction in WOMAC knee pain scores and a ~72% reversal rate from prediabetes to normoglycemia.
- Glucagon receptor activity appears to drive a lipid benefit, with roughly 20% reductions in LDL-cholesterol linked to PCSK9 degradation.
- All access to retatrutide remains confined to clinical trials and preclinical research settings — it cannot be legally prescribed or compounded.
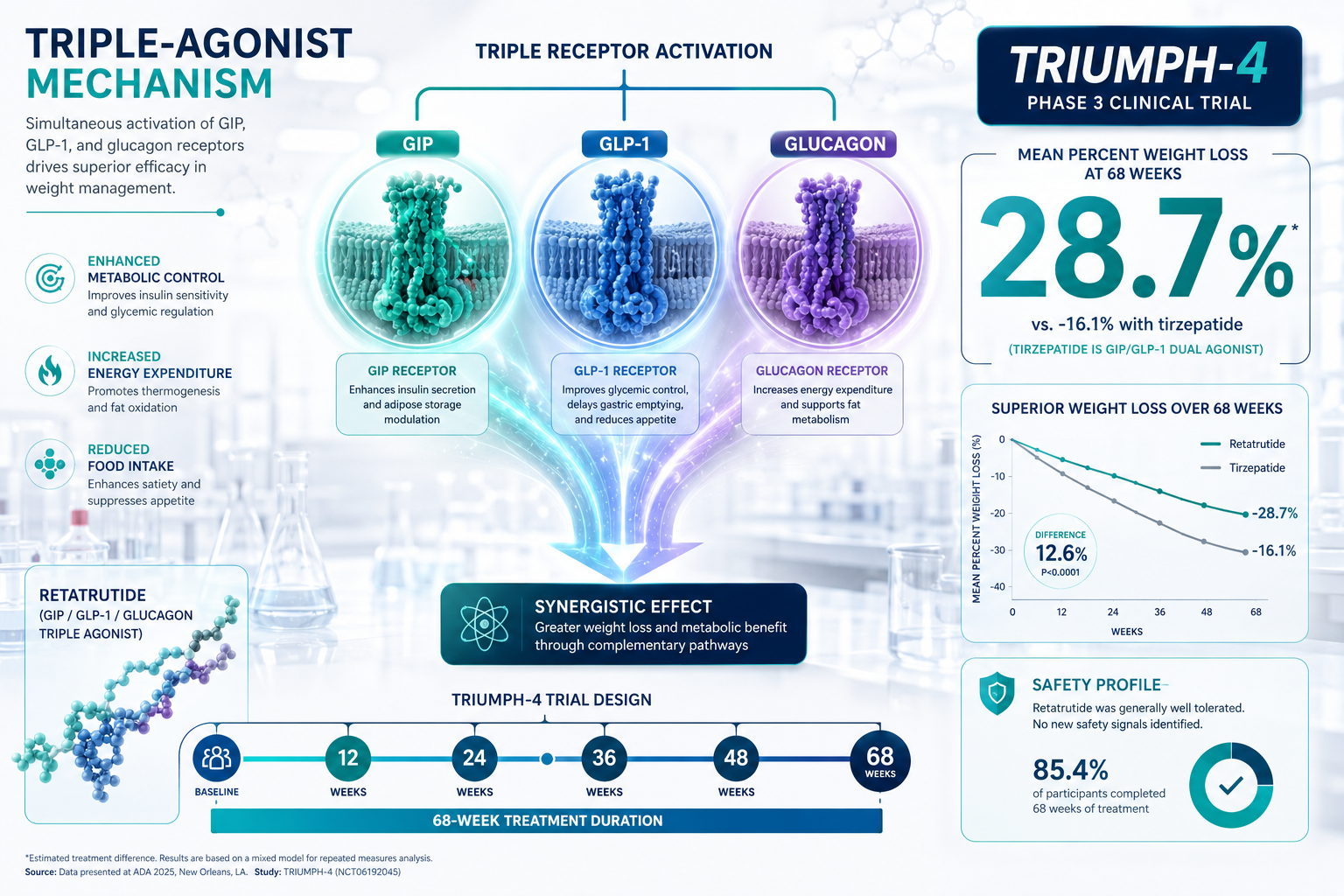
Understanding the TRIUMPH-4 Trial Design
Before interpreting any efficacy number, trial design matters. TRIUMPH-4 enrolled adults with obesity and knee osteoarthritis — a population chosen because weight reduction intersects directly with joint load and pain outcomes. Participants received once-weekly subcutaneous injections of retatrutide at either 9 mg or 12 mg, or placebo, over 68 weeks.
The dual primary endpoints were percent change in body weight and change in WOMAC pain score (a validated knee pain scale). This design is notable because it moved beyond simple weight loss to ask whether the weight loss translated into a clinically meaningful functional outcome.
Why this matters for researchers: The trial architecture reflects a broader trend in metabolic peptide research — moving from single-endpoint obesity studies toward multi-system outcome models. For those exploring metabolic modulation research lines, this multi-endpoint framing is increasingly the standard.
Retatrutide Clinical Trials: What Phase 3 Data Mean for Research-Only Readers — Efficacy Signals
The headline numbers from TRIUMPH-4 are striking by any standard in the obesity pharmacology literature.
| Arm | Mean Weight Loss | WOMAC Pain Reduction |
|---|---|---|
| Retatrutide 9 mg | 26.4% | Significant |
| Retatrutide 12 mg | 28.7% | ~75.8% (4.5-point) |
| Placebo | 2.1% | Minimal |
Beyond weight, three secondary signals deserve attention:
- Glycemic reversal: Approximately 72% of participants with prediabetes at baseline returned to normoglycemia. This is consistent with GLP-1 receptor-mediated insulin secretion enhancement.
- LDL reduction: Roughly 20% decreases in LDL-cholesterol were observed, a finding researchers attribute to glucagon receptor activity promoting PCSK9 degradation — a mechanism distinct from GLP-1 pathways alone.
- Joint pain: The 75.8% reduction in WOMAC pain scores suggests that weight loss magnitude at this level produces measurable musculoskeletal benefit, independent of any direct anti-inflammatory peptide effect.
For context on how triple agonism compares to dual-agonist approaches, the GLP-3 triple agonist research planning overview provides useful background on receptor targeting rationale.
Researchers studying adjacent metabolic compounds such as MOTS-c and metabolic flexibility or SLU-PP-332 metabolic research will recognize the overlapping interest in multi-pathway energy regulation.
Retatrutide Clinical Trials: What Phase 3 Data Mean for Research-Only Readers — Safety Reporting and Regulatory Status
No Phase 3 data set is complete without its safety profile. Retatrutide's adverse event pattern in TRIUMPH-4 followed the class-typical GI profile: nausea, vomiting, and diarrhea were the most commonly reported events, predominantly mild-to-moderate and dose-dependent. Discontinuation rates due to adverse events were consistent with other incretin-based therapies in Phase 3.
Critical regulatory note: As of June 2026, retatrutide holds no approval from the FDA, EMA, or any other major regulatory body. It cannot be legally prescribed, dispensed, or compounded as a medicine. All legitimate access is through enrolled clinical trials or preclinical laboratory research settings.
This distinction is not a formality. Researchers sourcing investigational compounds must verify purity and documentation rigorously. Reviewing quality testing protocols and understanding NAD and GLP-3 research sourcing considerations are practical steps for maintaining research integrity.
For those building broader metabolic research programs, longevity peptide research frameworks and the 5-Amino-1MQ research overview offer complementary context on energy metabolism targets.
Conclusion
The TRIUMPH-4 readout established retatrutide as the highest-performing weight-loss compound yet reported in a Phase 3 human trial, with multi-system benefits across glycemic, lipid, and musculoskeletal endpoints. For research-only readers, the data offer a clear signal: triple agonism at GIP, GLP-1, and glucagon receptors produces effects that exceed dual-agonist benchmarks in both magnitude and breadth.
Actionable next steps for researchers in 2026:
- Review the full TRIUMPH-4 trial protocol and supplementary data for endpoint methodology before drawing mechanistic conclusions.
- Map retatrutide's glucagon receptor contribution against your existing research on lipid and energy metabolism pathways.
- Ensure any investigational compound sourcing follows documented purity and chain-of-custody standards.
- Monitor the ongoing Phase 3 program for cardiovascular outcome data, which will be the next major inflection point in this research area.
The conversation around triple agonism has changed. The data say so.