Stacking Metabolic Modulators: 5‑Amino‑1MQ with GLP‑3 and SLUPP332‑Style Blends in Adiposity Research
Obesity now affects more than one billion people globally, yet the molecular toolkit available to researchers studying adipose dysfunction has never been more mechanistically diverse. Stacking metabolic modulators, specifically 5-Amino-1MQ with GLP-3 and SLUPP332-style blends in adiposity research, has emerged as one of the most discussed multi-pathway strategies in preclinical metabolic science as of 2026. This guide translates that momentum into a clear mechanistic framework for research professionals.
Key Takeaways
- 5-Amino-1MQ inhibits NNMT, raising cellular NAD+ and shifting adipocyte metabolism toward energy expenditure.
- SLUPP332-style compounds activate ERRalpha/gamma receptors, driving mitochondrial biogenesis and fat oxidation through a distinct but complementary pathway.
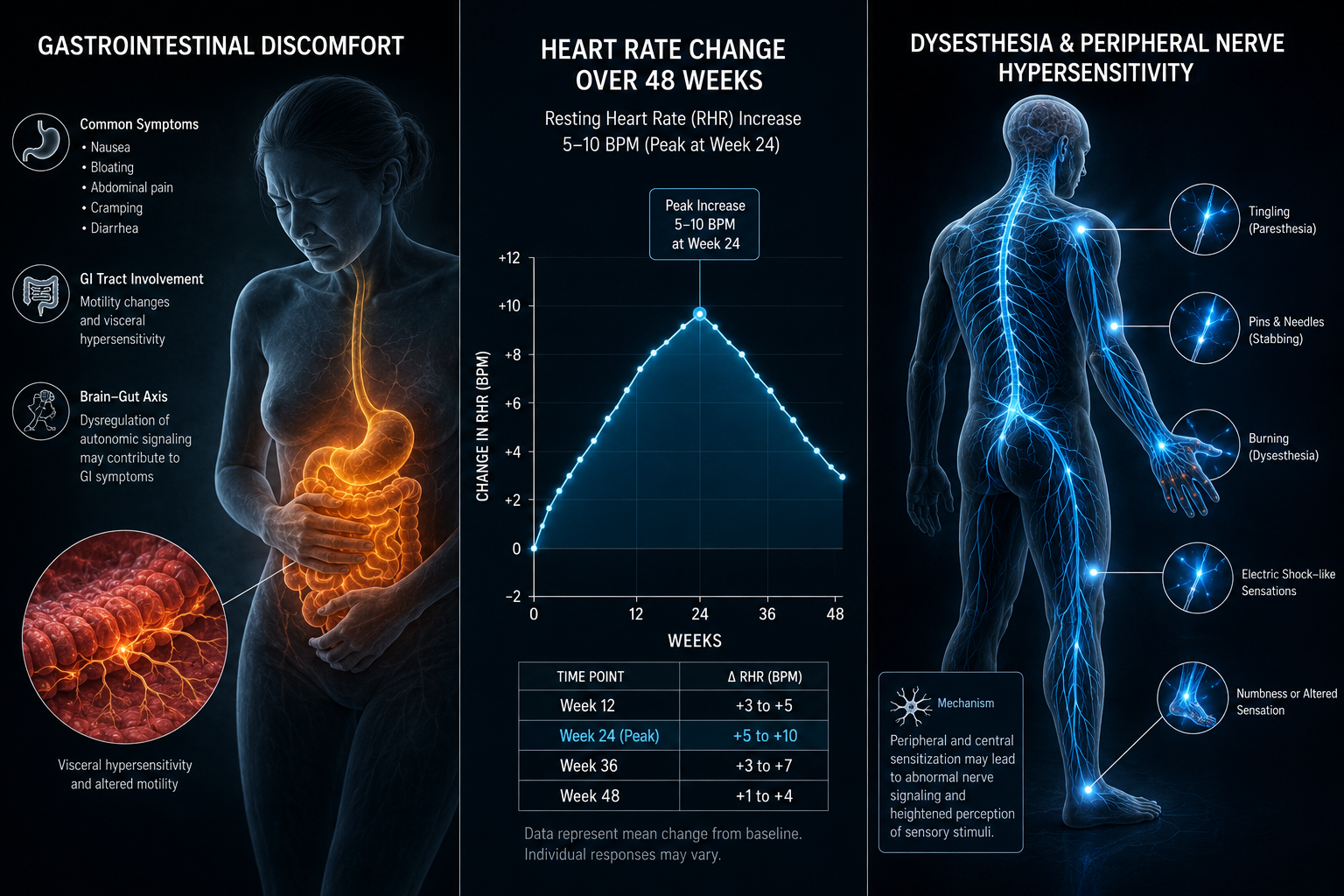
- GLP-3/retatrutide-class agents add incretin-mediated appetite and lipid signaling to the stack, creating a three-axis model.
- No human clinical trials have yet validated any of these combinations; all data remains preclinical as of mid-2026.
- Multi-pathway stacking is theoretically additive, but rigorous safety profiling for combined use is still absent from the literature.
Mechanistic Foundations of Stacking Metabolic Modulators
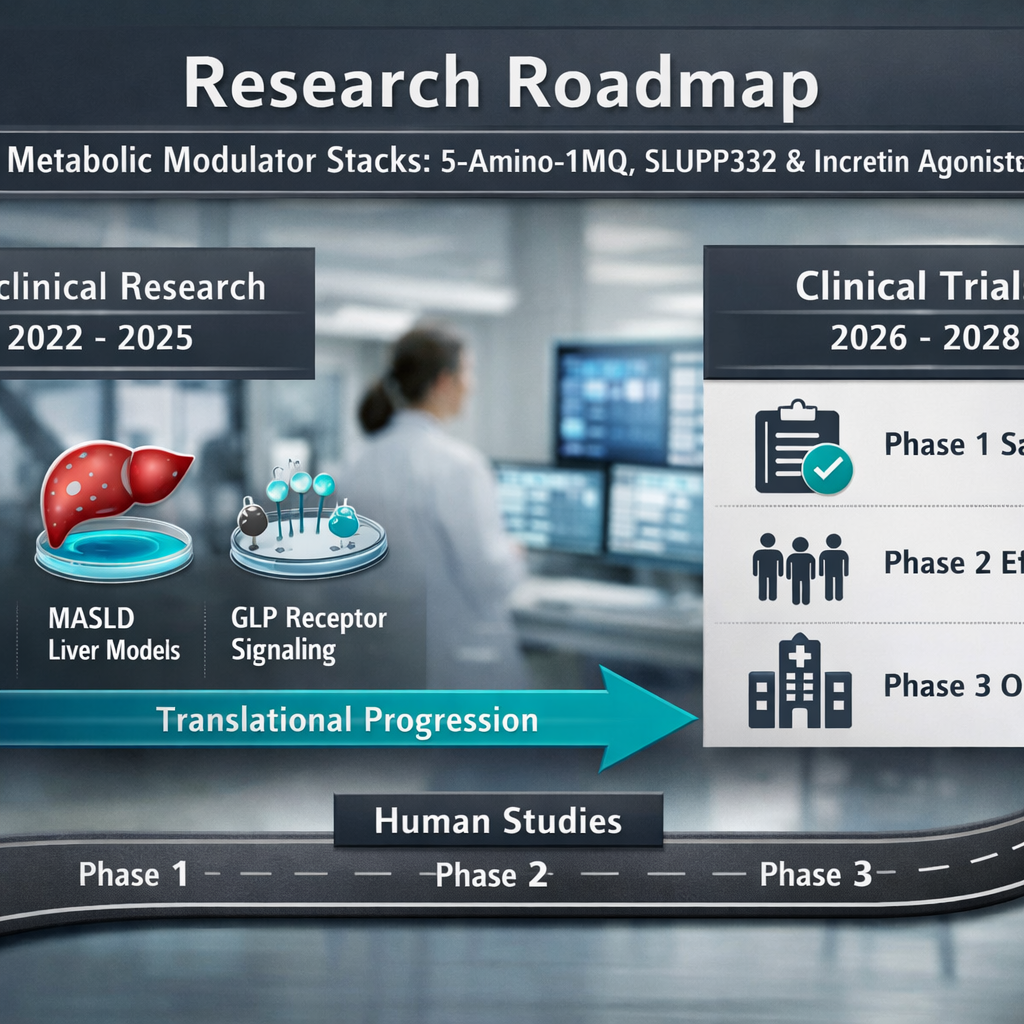
Understanding why researchers are interested in stacking metabolic modulators begins with the biology of adipose tissue dysfunction in obesity and metabolic-associated steatotic liver disease (MASLD).
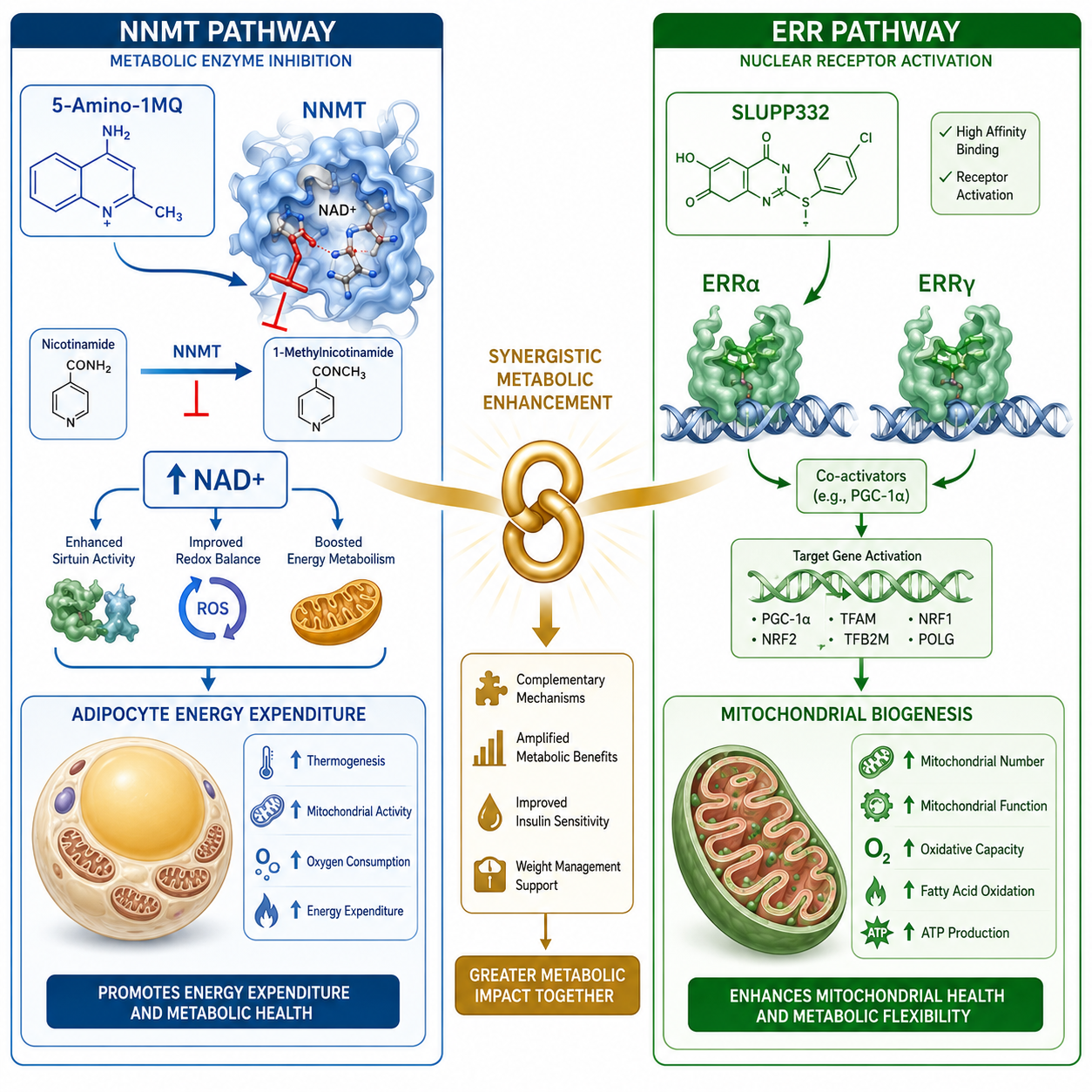
5-Amino-1MQ: NNMT Inhibition and NAD+ Elevation
5-Amino-1MQ is a small-molecule inhibitor of nicotinamide N-methyltransferase (NNMT), an enzyme significantly overexpressed in the adipose tissue of obese subjects. When NNMT is active, it consumes methyl groups and depletes the NAD+ precursor pool, effectively suppressing mitochondrial activity in fat cells.
By blocking NNMT, 5-Amino-1MQ:
- Elevates intracellular NAD+, activating sirtuins and PARP pathways
- Reduces lipid accumulation in adipocytes in preclinical models
- Shifts energy balance toward oxidative metabolism rather than storage
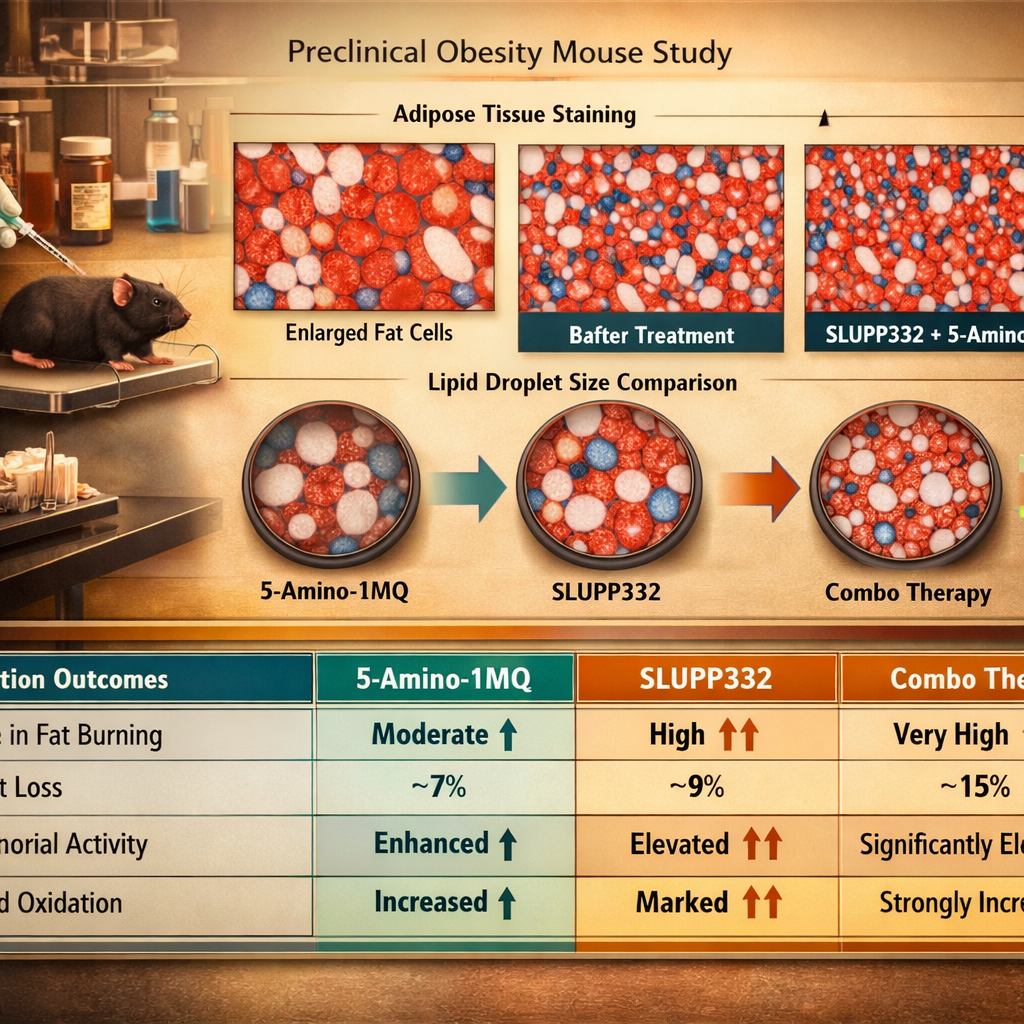
Preclinical data in rodent obesity models is compelling, though human clinical trial data remains absent as of 2026.
SLUPP332-Style Compounds: ERR Agonism and Mitochondrial Biogenesis
SLU-PP-332 metabolic modulation research centers on estrogen-related receptor alpha and gamma (ERRalpha/gamma) agonism. These nuclear receptors regulate genes governing oxidative phosphorylation and mitochondrial biogenesis, processes that are blunted in obese and insulin-resistant tissue.
Key SLUPP332-style effects in preclinical models:
| Mechanism | Observed Effect |
|---|---|
| ERRalpha activation | Upregulation of fatty acid oxidation genes |
| ERRgamma agonism | Increased mitochondrial density in skeletal muscle |
| Combined ERR agonism | Improved exercise endurance without training |
This makes SLUPP332-style compounds mechanistically distinct from, yet complementary to, 5-Amino-1MQ.
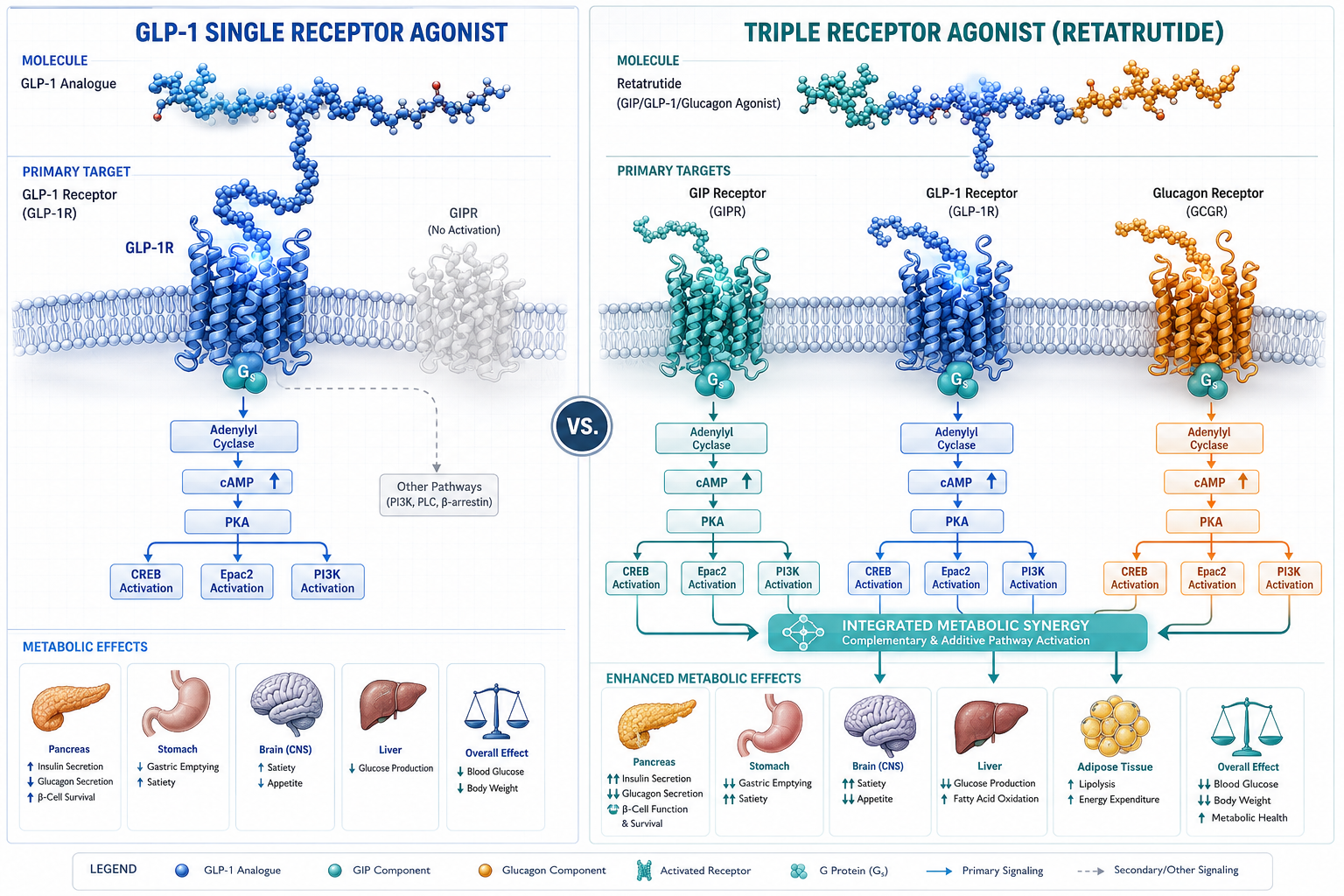
GLP-3, Retatrutide, and the Incretin Axis in Multi-Agent Stacking
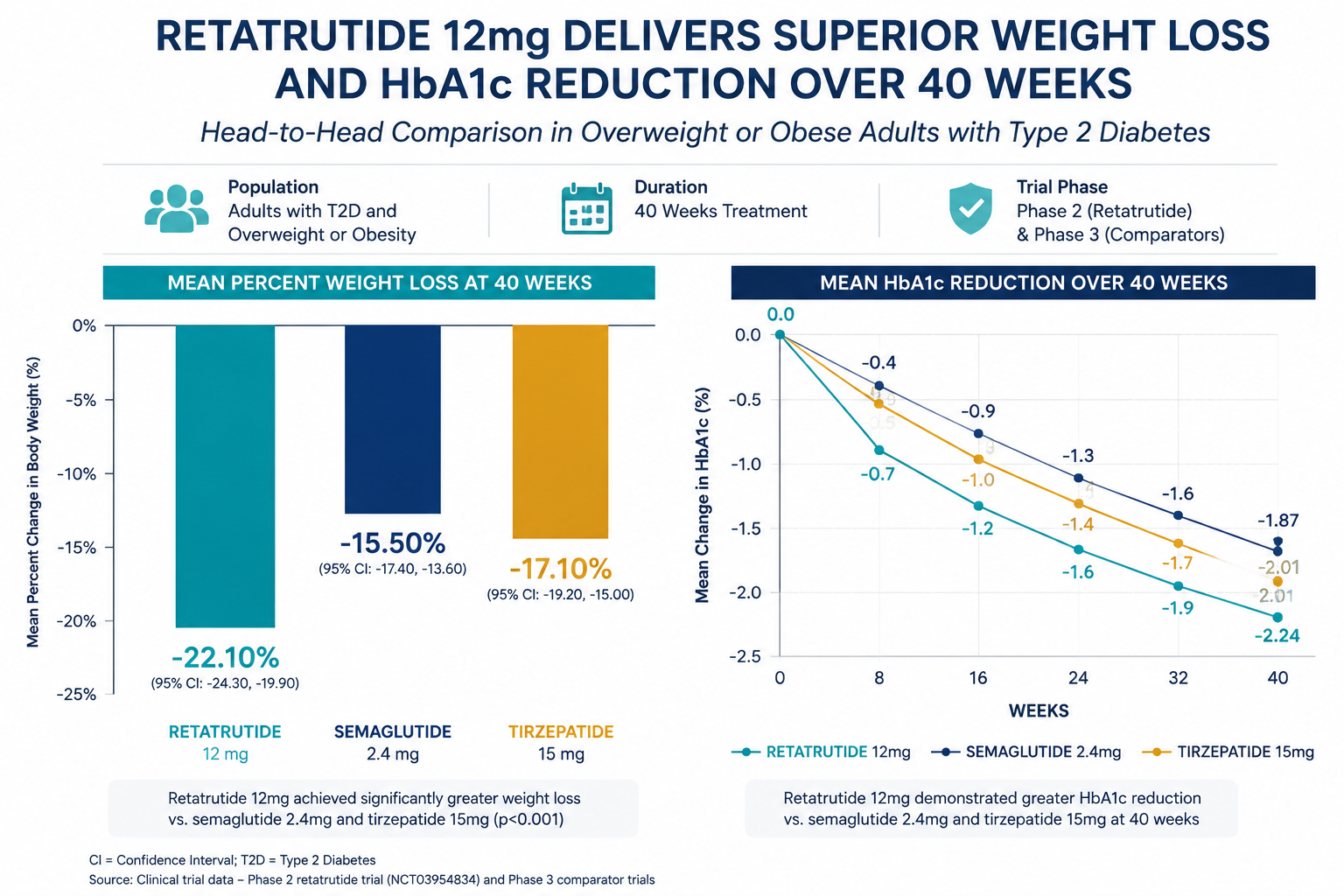
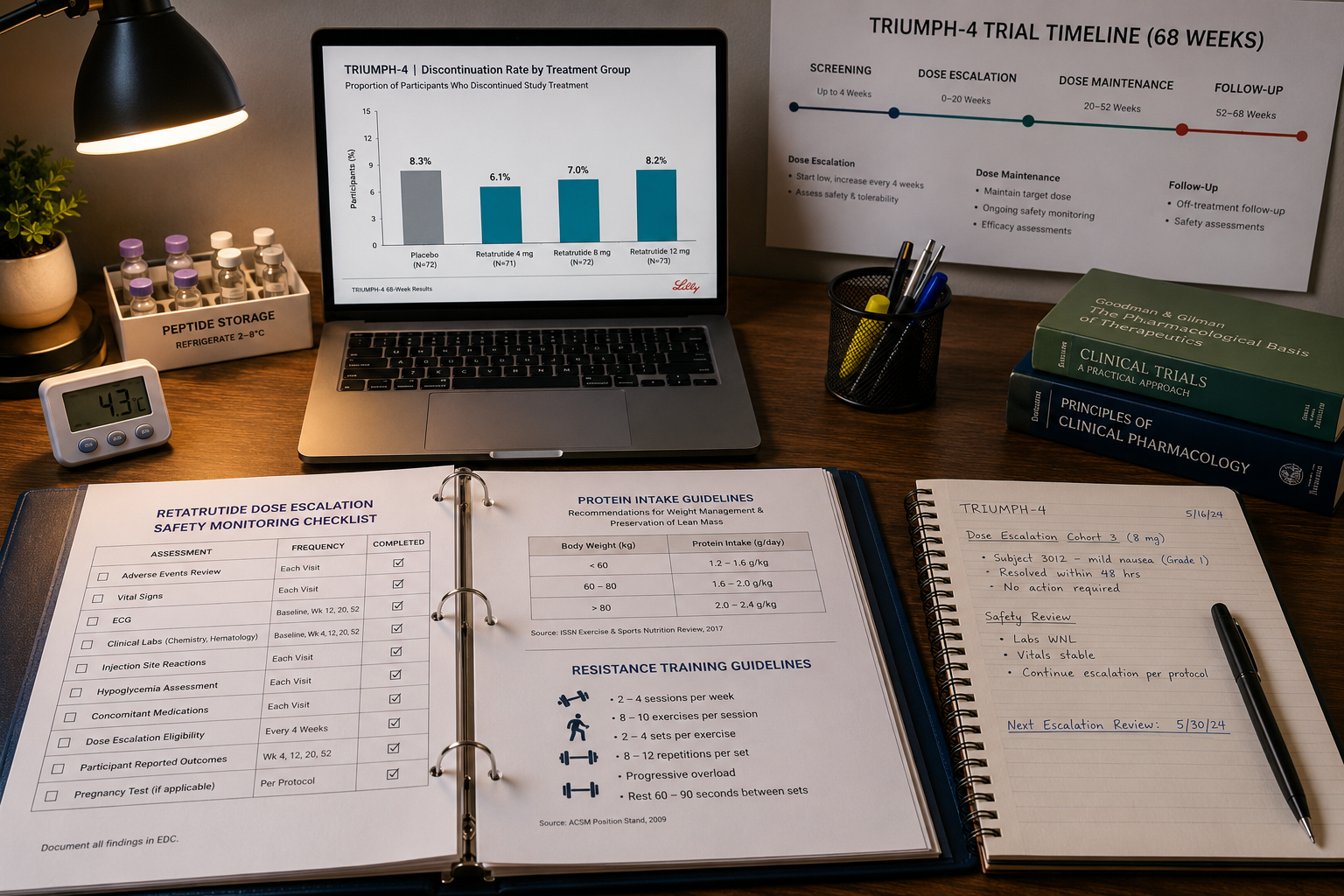
The term "GLP-3" does not correspond to a well-characterized receptor class in current peer-reviewed literature. In practice, researchers using this terminology are typically referencing retatrutide-class agents, triple agonists acting on GLP-1, GIP, and glucagon receptors simultaneously. For context on incretin-based research frameworks, GLP-1 incretin research themes provide foundational background, while GLP-3/retatrutide research covers the emerging triple-agonist landscape directly.
Why add an incretin agonist to a 5-Amino-1MQ/SLUPP332 stack?
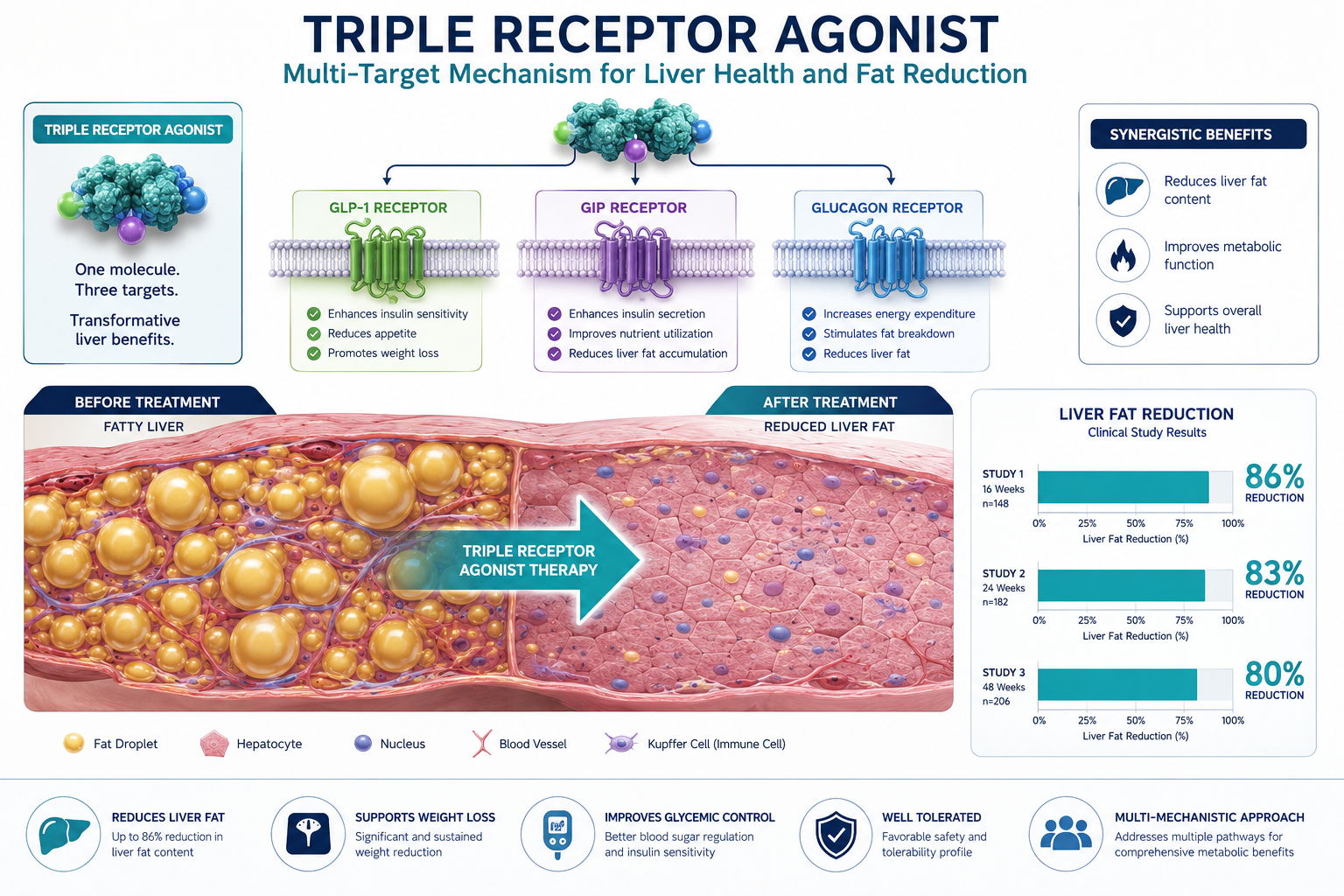
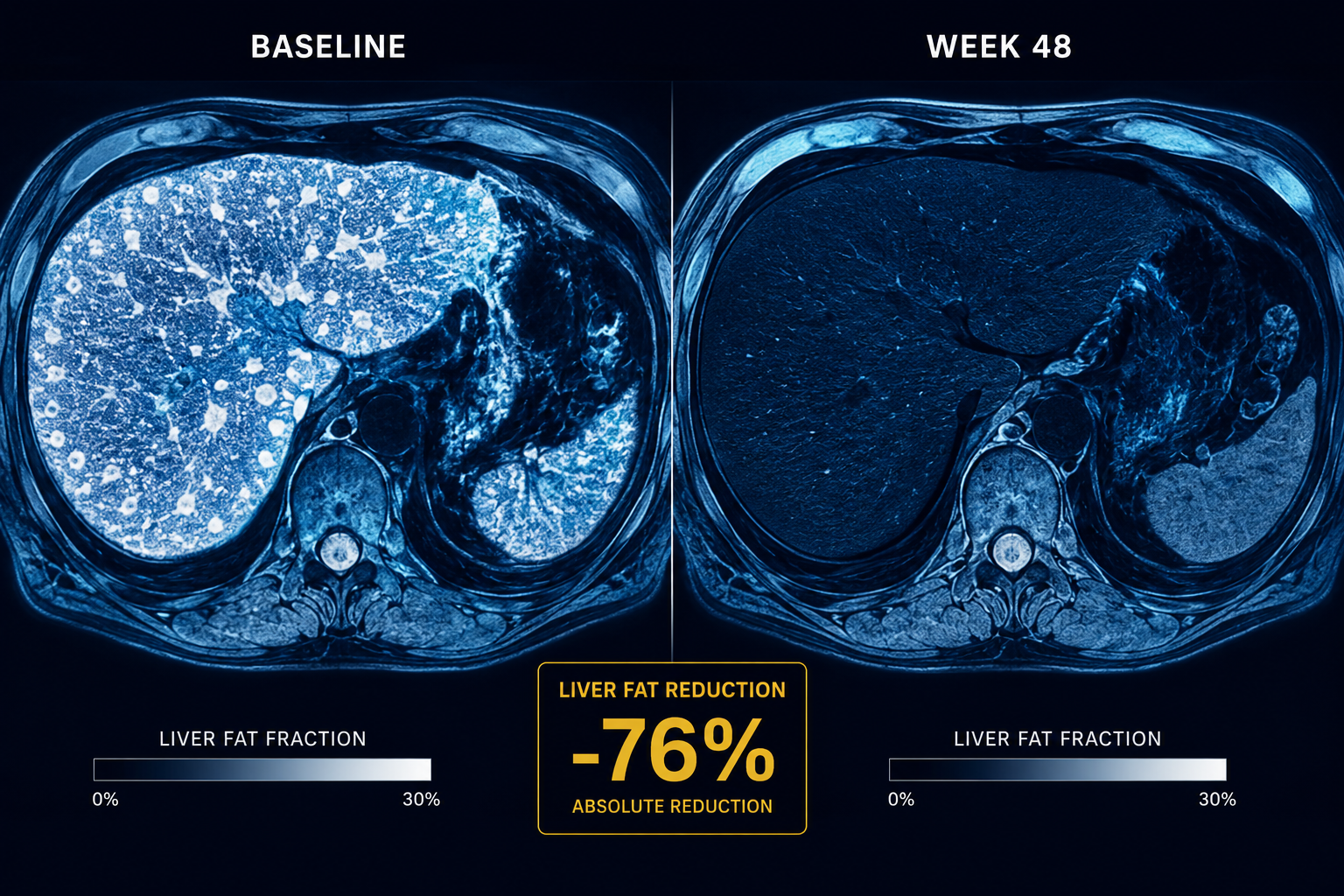
Retatrutide-class agents address appetite regulation and hepatic lipid flux, dimensions that NNMT inhibition and ERR agonism do not directly target. In MASLD models, the combination theoretically creates a three-axis attack on adiposity:
- Axis 1 (NNMT): Restore NAD+ metabolism in dysfunctional adipocytes
- Axis 2 (ERR): Rebuild mitochondrial capacity for fat oxidation
- Axis 3 (Incretin): Reduce caloric intake and hepatic triglyceride synthesis
Researchers exploring peptide blends for research have noted growing interest in exactly this type of complementary multi-pathway design.
MOTS-C as a Fourth Axis
MOTS-C and SLU-PP-332 combined research suggests that adding MOTS-C, a mitochondria-derived peptide that activates AMPK, may further reinforce the stack. AMPK activation overlaps with, but does not duplicate, the ERR and NAD+ pathways, potentially offering additive benefit in insulin-sensitization models.
Research Gaps and Critical Considerations for Stacking Metabolic Modulators in Adiposity Research
"Mechanistic elegance in preclinical models does not guarantee clinical translation, the history of metabolic pharmacology is filled with promising stacks that failed at the human trial stage."
This caution is especially relevant when stacking metabolic modulators: 5-Amino-1MQ with GLP-3 and SLUPP332-style blends in adiposity research represents a frontier that, as of mid-2026, lacks any published human clinical trial data for any individual component in this combination, let alone the full stack.
Critical gaps researchers must acknowledge:
- No human pharmacokinetic data for 5-Amino-1MQ or SLUPP332 combinations
- No established safety profile for concurrent NNMT inhibition plus ERR agonism
- GLP-3 terminology ambiguity risks conflating distinct receptor pharmacologies
- Interaction effects between NAD+ elevation and incretin signaling are unstudied
Those following what is new in peptide research will note that multi-agent metabolic stacks are among the most actively discussed topics in 2026 research communities, precisely because the mechanistic rationale is strong while clinical validation lags behind.
For researchers interested in adjacent body composition modalities, tesa and body composition research offers a more clinically validated comparator framework.
Conclusion
Stacking metabolic modulators, 5-Amino-1MQ with GLP-3 and SLUPP332-style blends in adiposity research, represents one of the most mechanistically sophisticated multi-pathway approaches in current obesity and MASLD research. The theoretical framework is coherent: NNMT inhibition restores NAD+ metabolism, ERR agonism rebuilds mitochondrial capacity, and incretin-class agents address appetite and hepatic lipid flux simultaneously.
Actionable next steps for researchers:
- Prioritize single-agent preclinical characterization before advancing to combination models
- Clarify receptor nomenclature, confirm whether "GLP-3" references retatrutide-class triple agonism
- Design combination studies with clear biomarker endpoints (NAD+/NADH ratio, mitochondrial density, hepatic triglyceride content)
- Monitor the clinical trial registry for first-in-human studies on NNMT inhibitors, anticipated in the near term
- Apply rigorous quality control standards to any research-grade compounds used in experimental models
The science is promising. The clinical evidence is not yet there. That gap is precisely where rigorous, well-designed research belongs.