

GLP-3 Retatrutide Dose Escalation: Understanding Tolerability and Side Effects in Research Studies
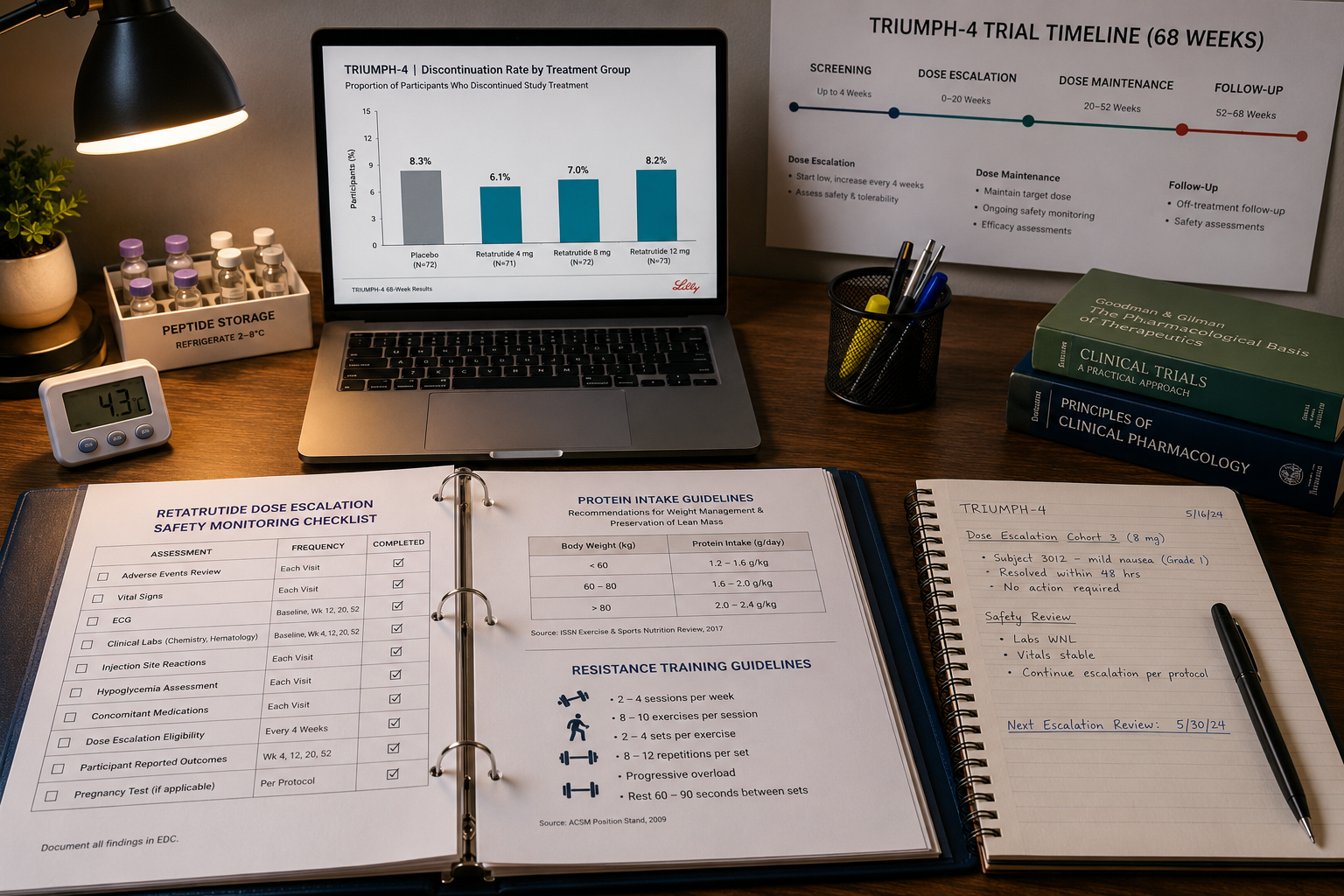
Discontinuation rates in Retatrutide research groups reached as high as 16% due to adverse events, compared to 0% in placebo groups. That single data point frames the central challenge researchers face when designing protocols around GLP-3 Retatrutide dose escalation: understanding tolerability and side effects in research studies is not optional; it is foundational to sound experimental design.
Key Takeaways
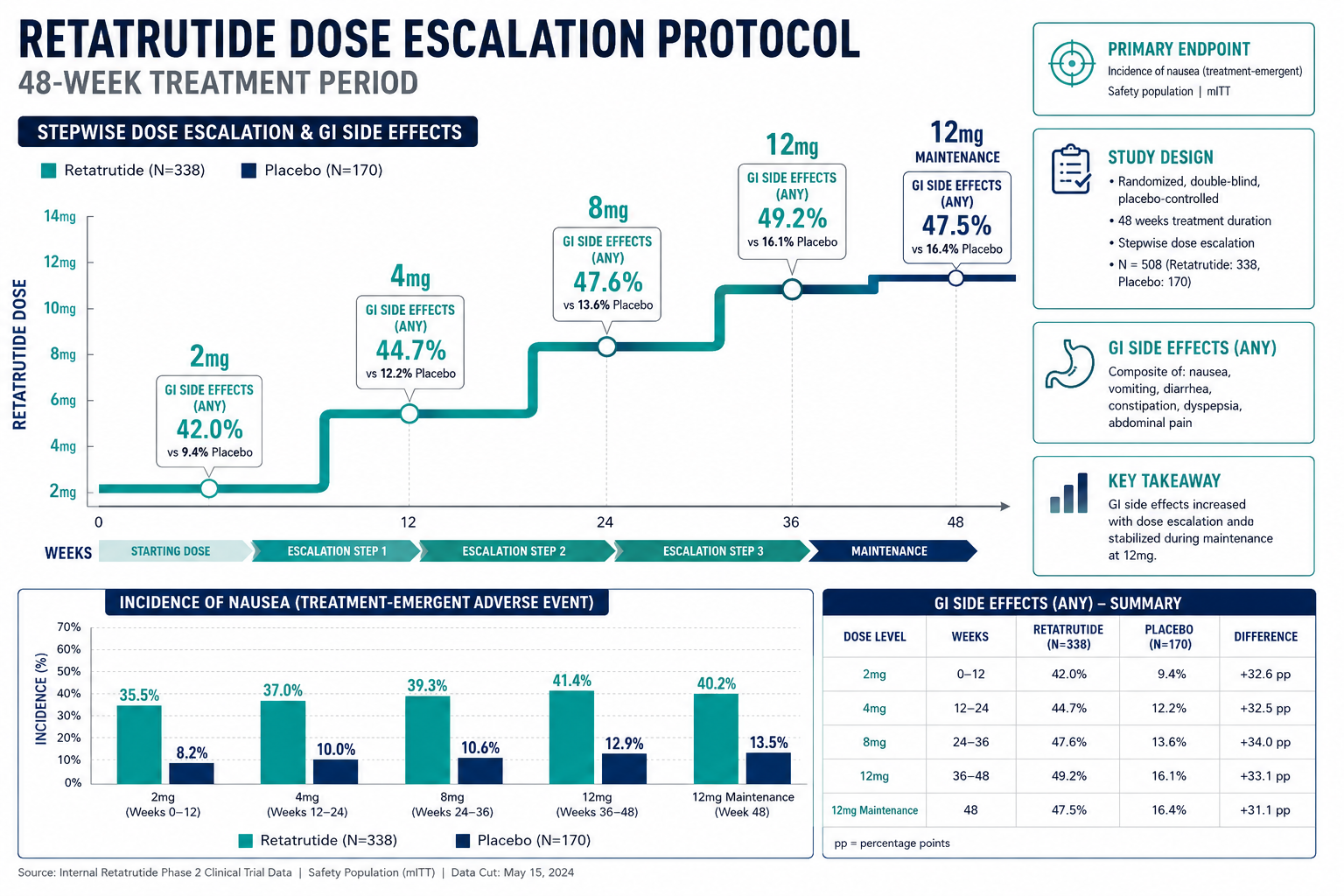
- Gastrointestinal side effects are the most common adverse events and are strongly dose-dependent, peaking during escalation phases.
- Gradual four-week dose escalation intervals significantly improve tolerability compared to rapid titration.
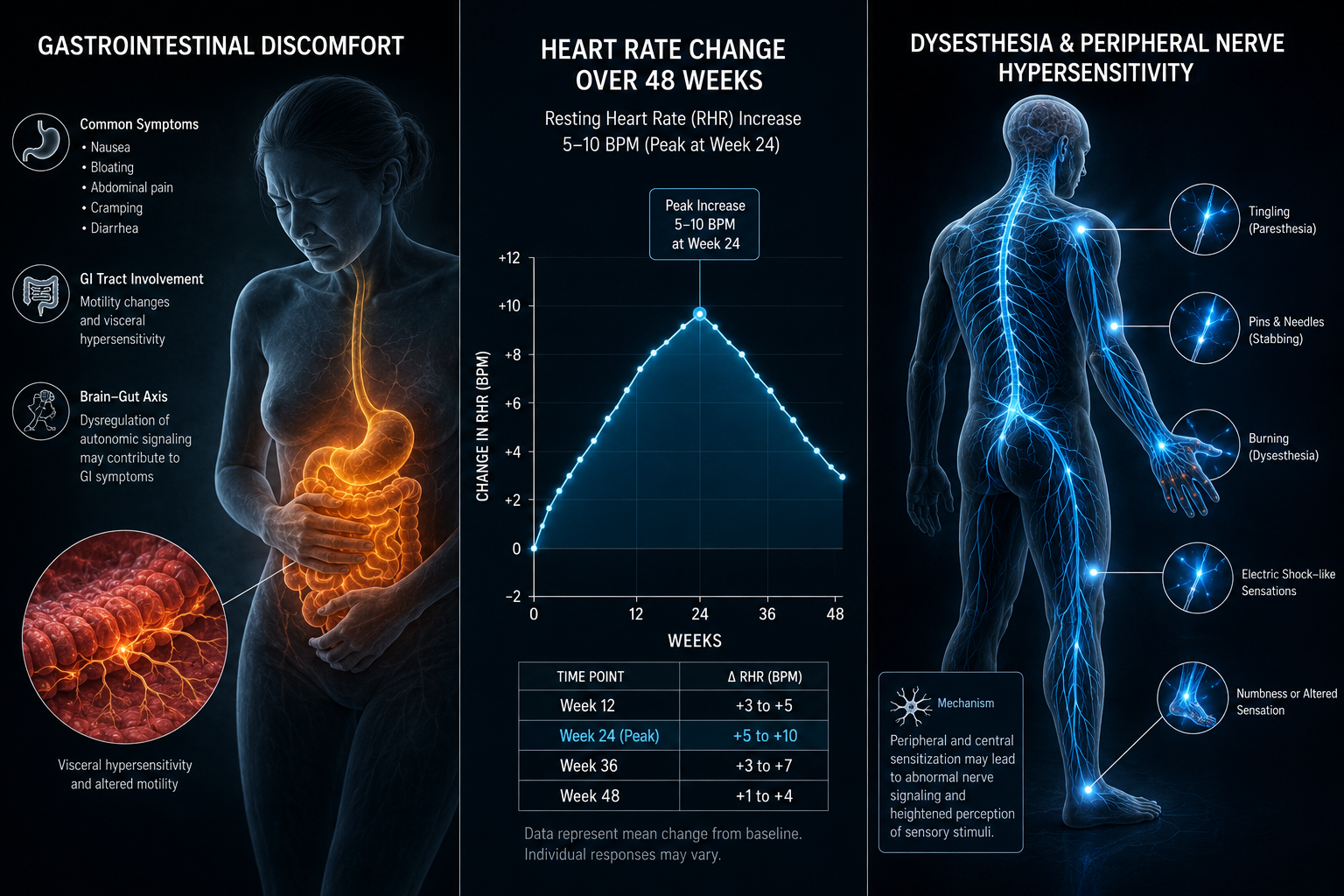
- A unique dysesthesia signal, abnormal tingling or burning, affects up to 20.9% of participants at the highest doses.
- Modest heart rate increases averaging 5 to 10 BPM have been observed, peaking around week 24.
- Approximately 25 to 40% of total weight lost may come from lean mass, making resistance training and protein intake critical protocol considerations.
Dose Escalation Protocol and the Tolerability Framework
The core principle guiding GLP-3 Retatrutide dose escalation in research settings is gradual titration. Starting at 2 mg and increasing in four-week intervals allows biological systems to adapt before advancing to higher dose tiers. This approach directly reduces the frequency and intensity of adverse events.
Retatrutide is a triple agonist acting on GLP-1, GIP, and glucagon receptors simultaneously. This multi-receptor activity drives its potent metabolic effects, but it also broadens the side effect profile compared to single-target GLP-1 agents. Researchers exploring GLP-1 and incretin research themes will recognize the GI tolerability pattern, but Retatrutide introduces additional signals not seen with earlier-generation compounds.
In the 48-week Phase 2 obesity trial, weight loss outcomes were clearly dose-dependent, reinforcing that higher doses carry both greater efficacy and greater tolerability burden. The 68-week TRIUMPH-4 Phase 3 trial further confirmed this relationship, with nausea rates of 38.1% at 9 mg and 43.2% at 12 mg, versus 10.7% in the placebo group.
Practical protocol guidance:
| Dose Tier | Approximate Duration | Primary Tolerability Risk |
|---|---|---|
| 2 mg | Weeks 1-4 | Minimal GI symptoms |
| 4 mg | Weeks 5-8 | Mild nausea onset |
| 8 mg | Weeks 9-16 | Moderate GI events peak |
| 12 mg | Weeks 17+ | Highest GI and dysesthesia risk |
Researchers sourcing material for metabolic studies can review the GLP-3 triple agonist research planning catalog for further context on compound availability and protocol scaffolding.
Side Effect Profile: What Research Data Reveals
Understanding the full tolerability and side effects in research studies requires examining each adverse event category individually.
Gastrointestinal Events
Nausea, vomiting, diarrhea, and constipation are the dominant adverse events. These are mild to moderate in most cases and cluster heavily during the escalation window rather than persisting at maintenance doses. Comparing Retatrutide to tirzepatide, GI event rates are measurably higher, a distinction researchers should factor into study design and participant selection criteria.
The Dysesthesia Signal
"Up to 20.9% of participants at the 12 mg dose reported dysesthesia, abnormal tingling or burning sensations, compared to just 0.7% in the placebo group."
This signal is notably absent from standard GLP-1 agonist profiles. The glucagon receptor component of Retatrutide is the suspected driver. Researchers designing longer-duration studies should include dysesthesia monitoring checkpoints, particularly at higher dose tiers. This distinguishes Retatrutide's side effect map from compounds like tesa, which carries its own distinct tolerability considerations.
Cardiovascular Signal: Heart Rate
Resting heart rate increases averaging 5 to 10 BPM have been documented, peaking near week 24 before partially attenuating. While modest, this elevation warrants baseline cardiovascular assessment in research subjects and ongoing monitoring throughout the protocol. Researchers interested in broader metabolic modulation research will find this cardiovascular signal relevant to multi-compound study design.
Lean Mass Considerations
Roughly 25 to 40% of total weight lost during Retatrutide studies is lean mass, a finding consistent across the broader GLP-1 drug class. Research protocols that do not account for this risk may produce confounded body composition data. Resistance exercise protocols and elevated protein intake are the primary mitigation strategies supported by current evidence.
For researchers examining complementary compounds that may address lean mass preservation, ipamorelin muscle and fat research themes offer relevant parallel data.
Designing Safer Research Protocols Around Retatrutide
Translating the GLP-3 Retatrutide dose escalation tolerability and side effects data into actionable protocol design requires structured decision-making.
Key protocol design checkpoints:
- Baseline screening: Cardiovascular status, GI history, and neurological baselines before initiating escalation.
- Escalation pacing: Strict four-week minimum intervals between dose increases; do not accelerate based on early tolerance.
- Adverse event monitoring windows: Heightened observation during weeks 5 through 20, when GI and dysesthesia events peak.
- Discontinuation thresholds: Pre-define stopping criteria; trial data shows 6 to 16% discontinuation rates, and researchers should plan for this range.
- Body composition tracking: Dual-energy X-ray absorptiometry (DEXA) or equivalent methods to monitor lean mass changes.
Long-term cardiovascular, renal, and oncological safety data remain incomplete pending results from the ongoing TRIUMPH-5 multi-year trial. This gap is a meaningful limitation for researchers planning extended protocols. Researchers interested in renal-adjacent peptide safety profiles may find value in reviewing SS-31 kidney health research as a comparative reference point.
Those sourcing Retatrutide for research can explore the Reta 10mg product tag for catalog options, while researchers building broader metabolic panels may also reference GLP-1 peptide product options for complementary compounds.
Conclusion
GLP-3 Retatrutide dose escalation: understanding tolerability and side effects in research studies is not a peripheral concern, it is the operational core of any well-designed Retatrutide protocol. The data from Phase 2 and TRIUMPH-4 trials provide a clear roadmap: GI events dominate the escalation window, dysesthesia is a unique and dose-dependent signal, heart rate elevations require cardiovascular monitoring, and lean mass loss demands proactive mitigation strategies.
Actionable next steps for researchers in 2026:
- Build four-week escalation intervals into every protocol from the outset.
- Include dysesthesia and cardiovascular monitoring checkpoints at weeks 12, 24, and 48.
- Define discontinuation criteria before the study begins, accounting for the 6 to 16% adverse-event dropout range.
- Pair Retatrutide protocols with body composition tracking to capture lean mass data.
- Monitor TRIUMPH-5 trial publications for emerging long-term safety data before extending protocol durations.
Researchers who treat the tolerability profile as a design input, not an afterthought, will produce more reliable, reproducible, and ethically sound data from their Retatrutide studies.









Leave a Reply
Want to join the discussion?Feel free to contribute!