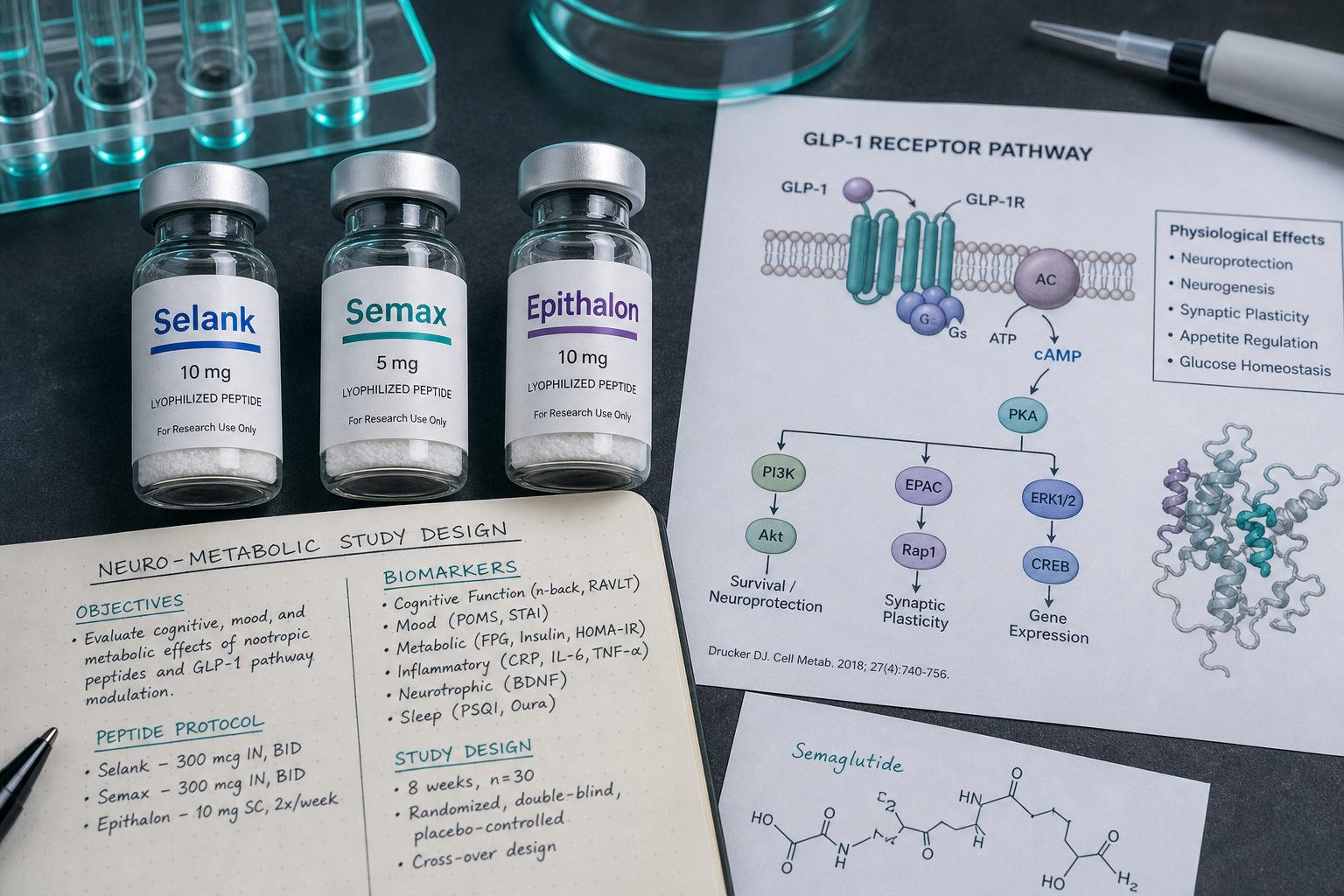
Neuroactive Research Peptides as Adjuncts to GLP‑1/GLP‑3: Selank, Semax, and Epithalon in Neuro‑Metabolic Study Designs
Fewer than 15% of subjects in GLP-1-based metabolic research protocols complete long-term study phases without reporting anxiety, sleep disruption, or cognitive fatigue, variables that rarely appear in primary endpoints but quietly shape adherence data. That gap is driving renewed interest in neuroactive research peptides as adjuncts to GLP-1/GLP-3: Selank, Semax, and Epithalon in neuro-metabolic study designs represent three candidates that researchers are increasingly pairing with incretin-based frameworks to address exactly these secondary endpoints.
Key Takeaways
- Selank, Semax, and Epithalon each target distinct neurological pathways, anxiety modulation, BDNF upregulation, and circadian/telomere regulation respectively, that may complement GLP-1 and GLP-3 metabolic protocols.
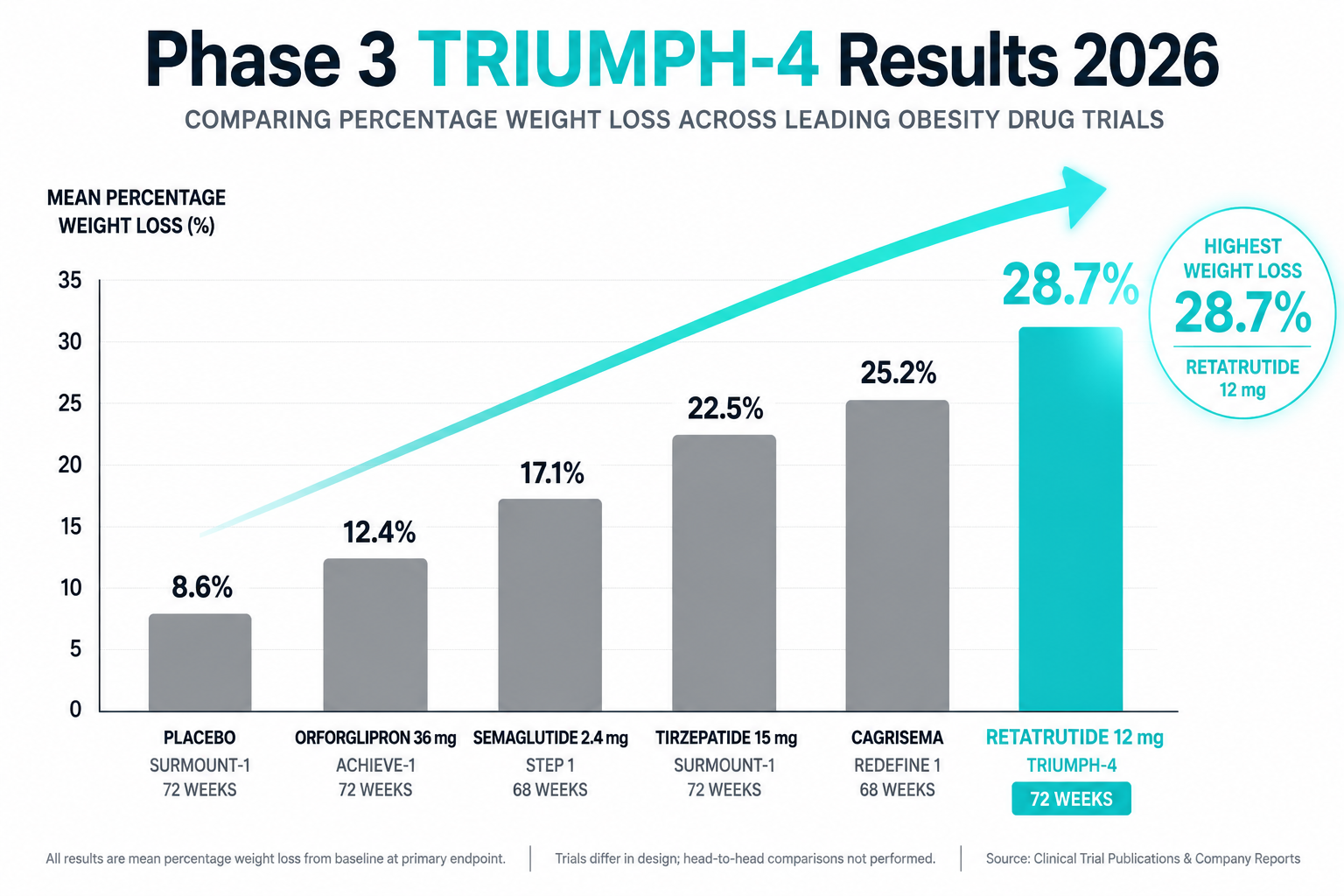
- GLP-1 receptor agonists combined with additional peptides have demonstrated up to a 32% reduction in food intake in research settings, suggesting multi-peptide synergy is a viable study design strategy.
- Both Semax and Selank are approved for medical use in Russia but lack large-scale Western randomized controlled trials, limiting regulatory standing outside that jurisdiction.
- Epithalon's influence on sleep architecture and pineal function positions it as a hypothesized adjunct for circadian-metabolic alignment in longer study windows.
- All three peptides are classified as research compounds and are subject to WADA prohibitions; researchers must account for regulatory context in study design.
Mechanisms: How Selank, Semax, and Epithalon Map to Neuro-Metabolic Pathways
Understanding why these compounds attract attention in metabolic research begins with their individual mechanisms.
Semax is a synthetic heptapeptide derived from adrenocorticotropic hormone (ACTH). Its most studied action is the upregulation of Brain-Derived Neurotrophic Factor (BDNF) in the hippocampus and cortex. BDNF elevation activates TrkB receptors, supporting neuronal survival, synaptic plasticity, and cognitive function. In metabolic research contexts, BDNF is not merely a cognitive marker, it also plays a documented role in energy homeostasis and hypothalamic appetite regulation, making Semax a biologically plausible adjunct in neuro-metabolic designs.
Selank, also a heptapeptide but derived from the immunomodulatory peptide tuftsin, operates through a different set of mechanisms. It modulates monoamine metabolism, increases GABA release, and regulates serotonin-related gene expression. The result is anxiolytic and nootropic activity without the sedation or dependence risk associated with classical anxiolytics. Researchers studying Selank peptide benefits note its potential relevance to stress-driven eating behavior and cortisol-mediated metabolic disruption, endpoints that are rarely isolated in standard GLP-1 trials but are mechanistically significant.
Epithalon (also spelled Epitalon) is a tetrapeptide synthesized from epithalamin, a pineal gland extract. Its primary research interest centers on telomerase activation, circadian rhythm normalization, and melatonin secretion support. Disrupted sleep architecture is strongly associated with impaired insulin sensitivity and elevated ghrelin, which means Epithalon's circadian-regulatory properties carry direct metabolic relevance. Researchers exploring Epithalon peptides for sale in research contexts often frame it within longevity and metabolic aging study designs.
"The intersection of neurological stability and metabolic regulation is not incidental, it is mechanistic. Anxiety, sleep quality, and cognitive load each modulate the hormonal environment that GLP-1 therapies are designed to influence."
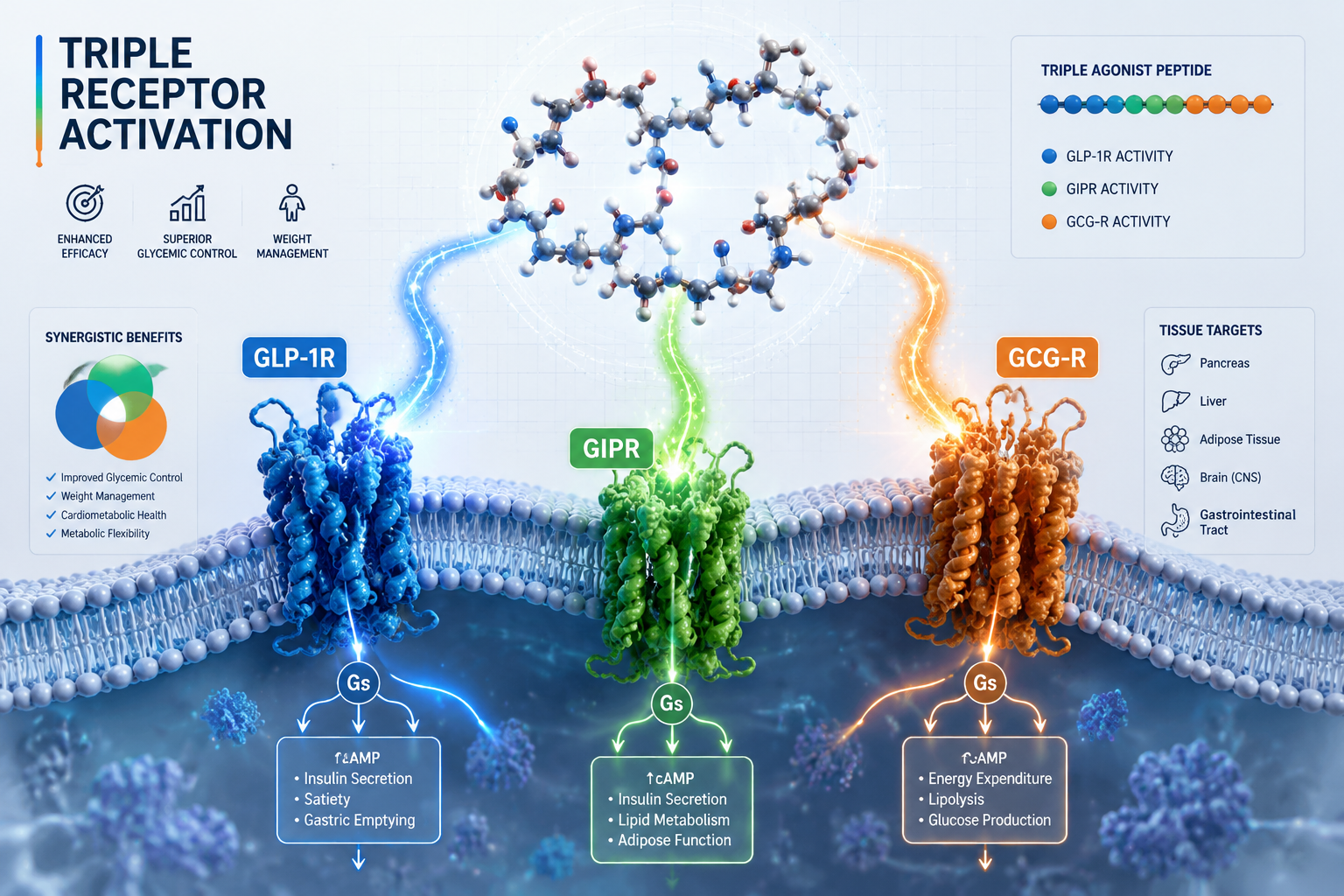
GLP-1/GLP-3 Synergy and the Case for Multi-Peptide Study Designs
GLP-1 receptor agonists have reshaped metabolic research, but their scope is expanding. Combined infusion studies using GLP-1 alongside oxyntomodulin and peptide YY have recorded a 32% reduction in food intake among obese research subjects, evidence that multi-peptide protocols can produce outcomes beyond what single-agent designs achieve.
GLP-3, a lesser-studied incretin fragment, is gaining attention for its potential role in gut-brain signaling and neuroinflammation modulation. When researchers consider NAD research and GLP-3 online resources, the emerging picture is one of overlapping neuroendocrine pathways where incretin biology and neuropeptide biology converge.
The rationale for pairing Selank, Semax, or Epithalon with GLP-1/GLP-3 frameworks rests on several hypothesized interaction points:
| Peptide | Primary Research Target | Hypothesized GLP-1/GLP-3 Adjunct Role |
|---|---|---|
| Semax | BDNF upregulation, neuroprotection | Hypothalamic appetite axis support, cognitive adherence |
| Selank | Anxiolysis, serotonin/GABA modulation | Stress-eating attenuation, cortisol normalization |
| Epithalon | Circadian regulation, telomerase activation | Sleep-metabolic alignment, insulin sensitivity support |
GLP-1 infusions have also been shown to augment muscle protein synthesis in older adults, addressing anabolic resistance, a finding that becomes more relevant when paired with Epithalon's anti-aging and cellular repair research themes. For researchers interested in related metabolic peptide frameworks, AOD9604 metabolic research and 5-Amino-1MQ research data offer additional mechanistic context for multi-pathway designs.
Study Design Considerations, Safety Profiles, and Regulatory Context
Designing a neuro-metabolic study that incorporates neuroactive research peptides as adjuncts to GLP-1/GLP-3, Selank, Semax, and Epithalon in neuro-metabolic study designs specifically, requires careful attention to both safety data and regulatory standing.
Safety profiles for Semax and Selank are generally favorable in existing literature. Semax is well-tolerated, with rare adverse events limited to mild nasal irritation and transient agitation. Selank is considered non-sedative and non-addictive, with uncommon side effects including mild daytime drowsiness or dry mouth. Epithalon has a strong preclinical safety record, though long-term human data remains limited.
Critically, neither Semax nor Selank has undergone large-scale randomized controlled trials in Western research settings. Both are approved for medical use in Russia, Semax for stroke recovery and neurological disease, Selank for mild anxiety, but neither holds FDA or EMA approval. Researchers should also note that WADA classifies both Semax and Selank as prohibited substances due to their neuroenhancement potential.
For researchers building multi-peptide protocols, resources on neuroendocrine and innate immunity research themes and PT-141 neural-metabolic research themes provide useful comparative frameworks for designing endpoints that capture both neurological and metabolic variables.
Key study design checkpoints include:
- Baseline neurological assessments for anxiety, sleep quality, and cognitive function before GLP-1/GLP-3 protocol initiation
- Defined adjunct dosing windows that avoid confounding primary incretin endpoints
- Secondary endpoint tracking for cortisol, BDNF, melatonin, and inflammatory markers
- Institutional review and ethics compliance given the unapproved status of all three peptides in most Western jurisdictions
Conclusion
The convergence of neuroactive research peptides as adjuncts to GLP-1/GLP-3, Selank, Semax, and Epithalon in neuro-metabolic study designs, reflects a broader shift in how researchers are framing metabolic science. Rather than treating anxiety, cognition, and sleep as confounding variables, forward-looking study designs are beginning to treat them as mechanistically relevant endpoints in their own right.
Actionable next steps for researchers in 2026:
- Review existing GLP-1 protocol data for unreported neurological secondary variables that Selank or Semax could address in follow-up designs.
- Incorporate Epithalon into longer study windows where circadian-metabolic alignment is a measurable outcome.
- Consult institutional review boards early regarding the regulatory status of all three peptides before protocol submission.
- Explore multi-peptide synergy literature, including cagrilintide synergy with GLP-1 and GLOW blend longevity research themes, to build a comparative evidence base.
The evidence base remains early-stage, but the mechanistic logic is sound. Rigorous trial design, not speculation, will determine whether these peptides earn a formal role in neuro-metabolic research protocols.