Retatrutide and GLP-3 Biology: What Makes This Triple-Agonist Different From GLP-1 and GLP-2 Research Peptides
A single drug achieving nearly 28% body weight reduction over 18 months — matching bariatric surgery outcomes — is not a minor incremental advance. That is the headline finding driving intense scientific interest in retatrutide in 2026. Yet most discussions skip past the foundational biology. Understanding Retatrutide and GLP-3 Biology: What Makes This Triple-Agonist Different From GLP-1 and GLP-2 Research Peptides requires a clear look at receptor targets, metabolic pathways, and why adding a third agonist arm changes the equation entirely.
Key Takeaways
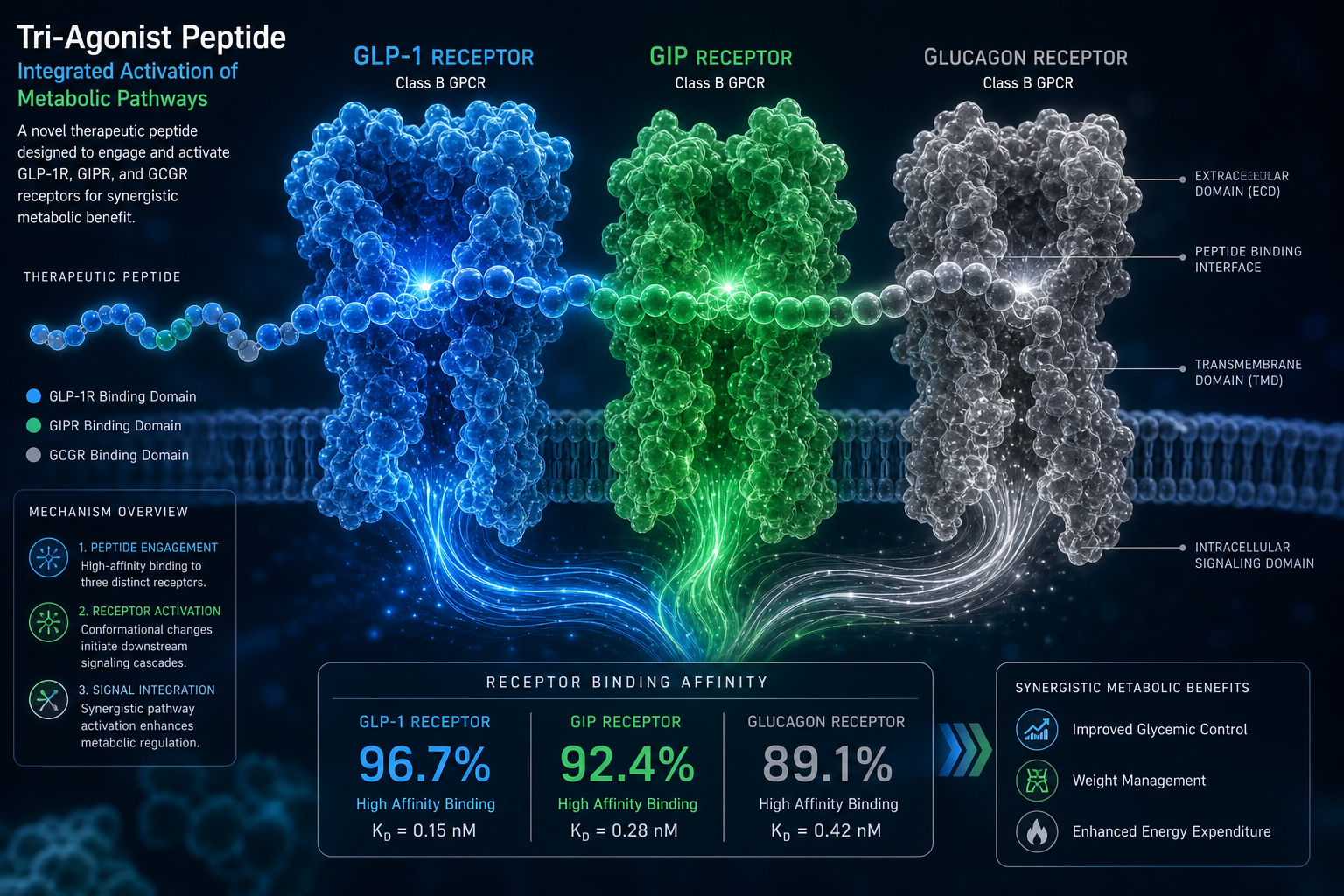
- Retatrutide simultaneously activates three receptors: GLP-1, GIP, and glucagon — a combination no approved drug currently achieves.
- The glucagon receptor arm drives energy expenditure and fat oxidation, which is absent in both semaglutide and tirzepatide.
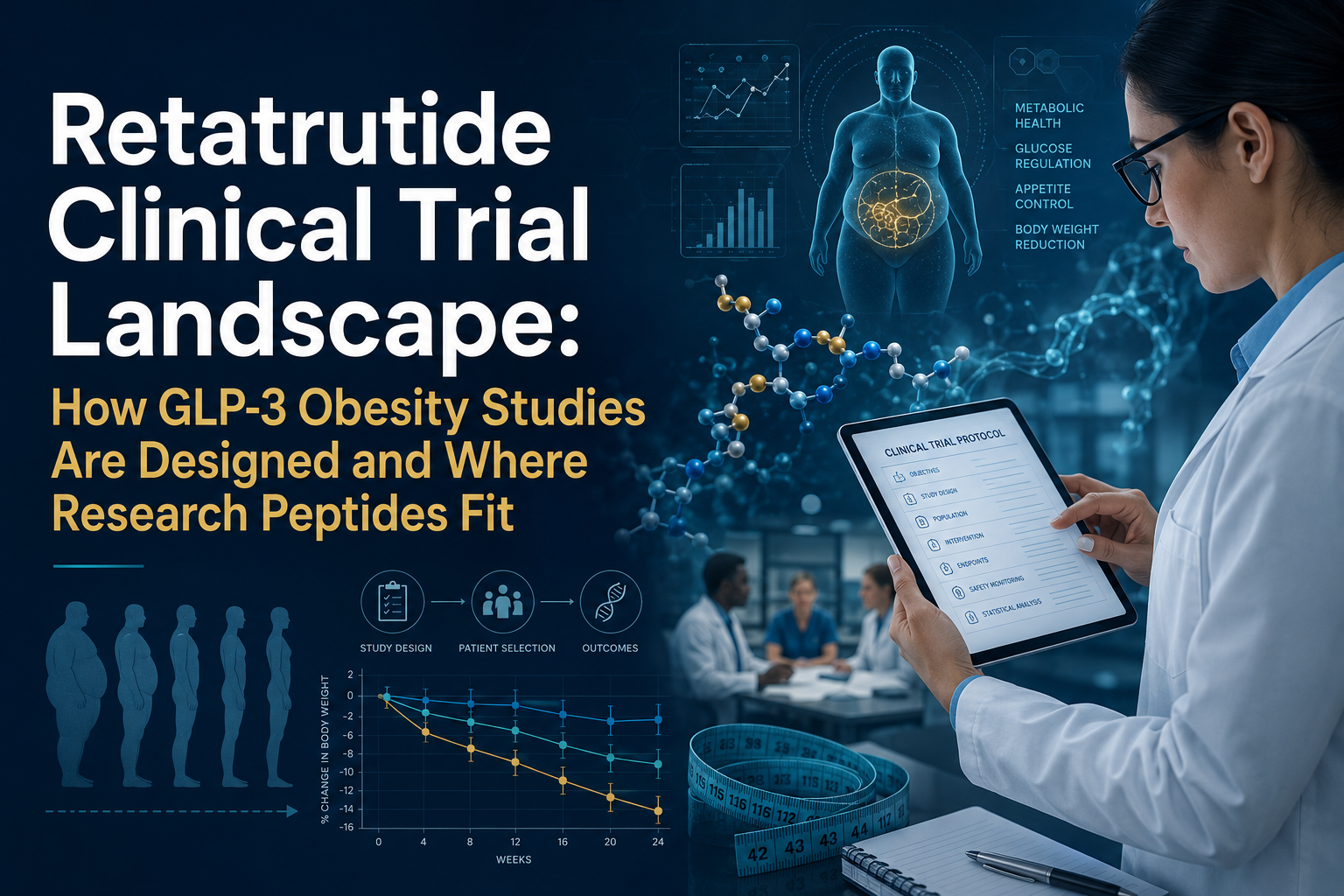
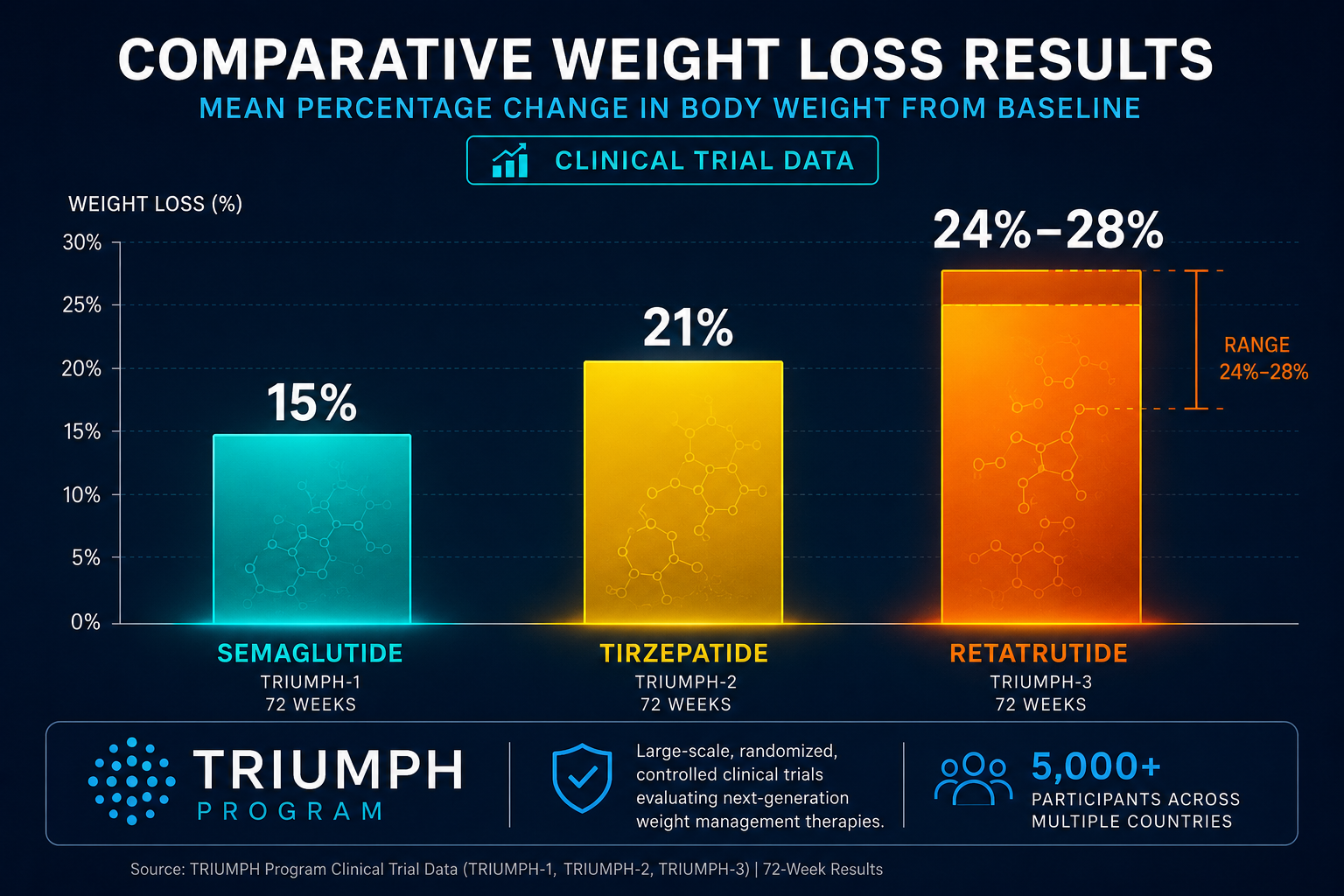
- Phase 3 data show mean weight reductions of 22–28%, placing retatrutide above existing GLP-1 therapies.
- GLP-2 is a structurally related incretin but targets gut mucosal biology, not metabolic weight pathways — making the GLP-1 vs. GLP-2 distinction critical for researchers.
- Eli Lilly plans an NDA submission to the FDA in late 2026, with commercial approval anticipated in 2027.
Understanding the GLP Receptor Family Before Comparing Compounds
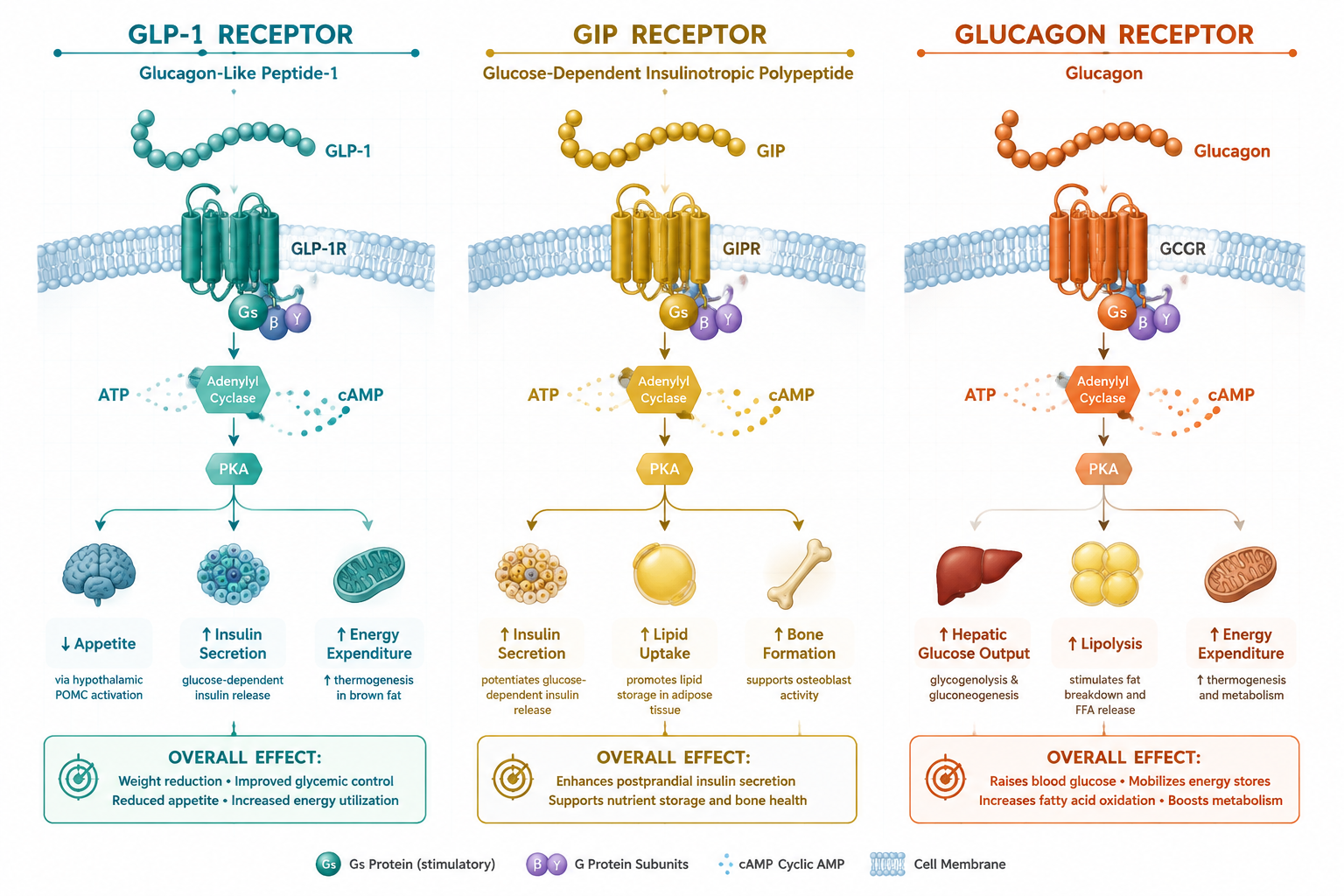
The glucagon-like peptide (GLP) family includes GLP-1 and GLP-2, both derived from the same precursor protein, proglucagon. Despite their shared origin, they act on entirely different tissues and serve different biological roles.
GLP-1 is an incretin hormone released from intestinal L-cells after eating. It binds GLP-1 receptors in the pancreas, brain, and gut to suppress appetite, slow gastric emptying, and stimulate insulin secretion. This is the pathway targeted by semaglutide and, in part, by tirzepatide.
GLP-2, by contrast, acts primarily on intestinal epithelial cells. It promotes gut mucosal growth, reduces intestinal permeability, and supports nutrient absorption. GLP-2 analogs like teduglutide are studied in short bowel syndrome — not obesity or metabolic disease. Researchers exploring GLP-1 incretin research themes will recognize that GLP-2 occupies a separate biological lane entirely.
The term "GLP-3" does not refer to a formally classified endogenous hormone. In current research shorthand, it is used informally to describe the triple-agonist concept — a molecule that hits GLP-1, GIP (glucose-dependent insulinotropic polypeptide), and glucagon receptors simultaneously. For a deeper look at this emerging terminology, see the overview of GLP-3 as the newest triple-agonist concept.
How Retatrutide and GLP-3 Biology Redefine the Triple-Agonist Mechanism
Retatrutide's design is built around three coordinated receptor interactions:
| Receptor | Primary Effect | Metabolic Outcome |
|---|---|---|
| GLP-1 | Appetite suppression, slowed gastric emptying | Reduced caloric intake |
| GIP | Enhanced insulin secretion and sensitivity | Improved glucose control |
| Glucagon | Increased energy expenditure, fat oxidation | Greater caloric burn |
The glucagon receptor arm is what separates retatrutide from every approved therapy. Semaglutide activates only GLP-1. Tirzepatide adds GIP to GLP-1. Retatrutide adds glucagon on top of both.
"The glucagon component is not redundant — it targets a fundamentally different metabolic lever by increasing thermogenesis and hepatic fat clearance."
This third pathway matters because appetite suppression alone has a ceiling. Raising energy expenditure through glucagon receptor activation addresses the metabolic adaptation that often limits long-term weight loss. Researchers interested in how GIP receptor biology contributes to metabolic outcomes will find that the dual GLP-1/GIP axis in tirzepatide already outperforms GLP-1 monotherapy — and retatrutide extends that logic further.
The tradeoff is tolerability. The glucagon component contributes to a higher incidence of nausea and gastrointestinal side effects, requiring a slower dose titration compared to dual agonists.
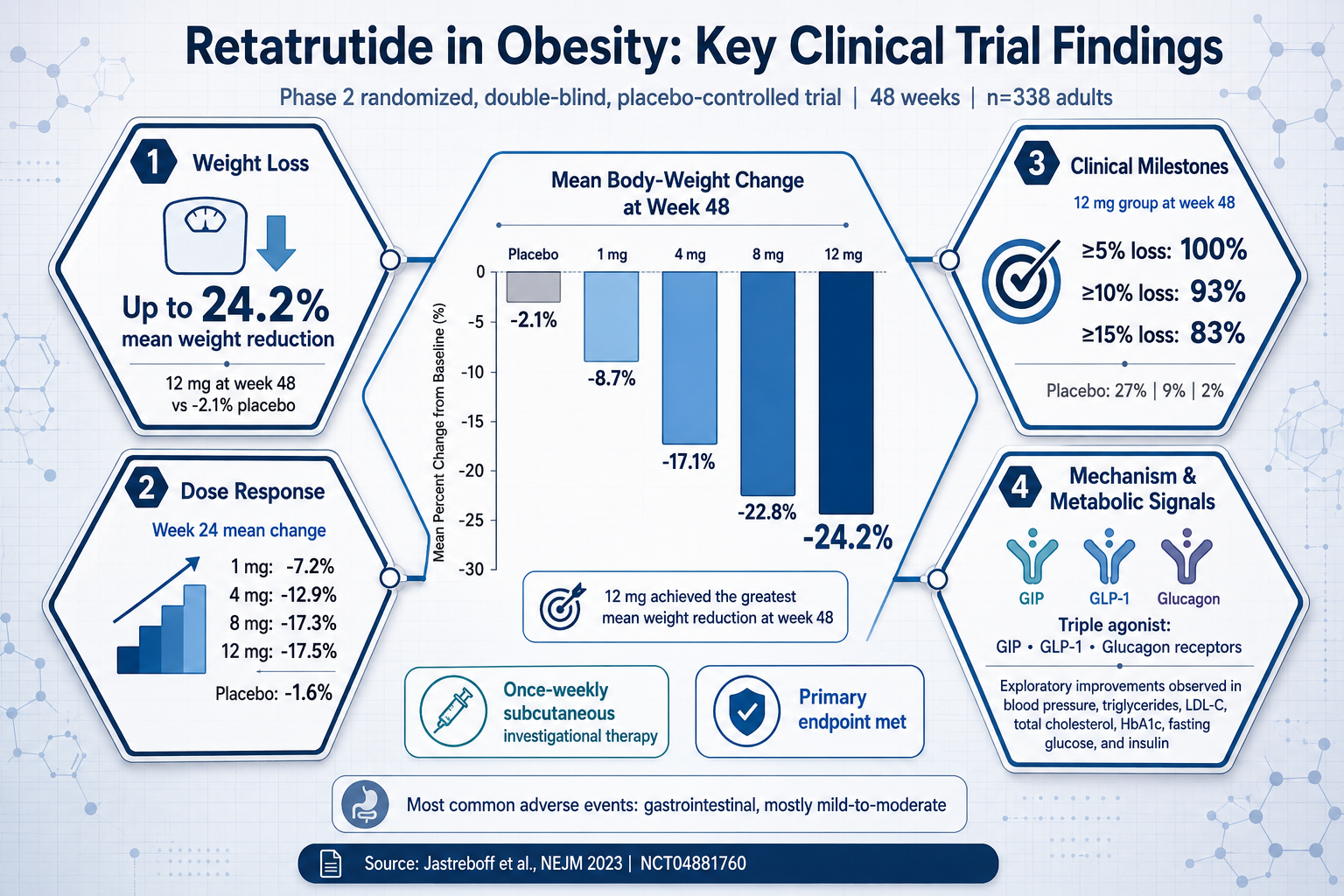
Phase 3 Data and What Retatrutide and GLP-3 Biology Mean for Research in 2026
Eli Lilly's TRIUMPH Phase 3 program is evaluating retatrutide across multiple populations:
- TRIUMPH-3: Adults with obesity, no type 2 diabetes
- TRIUMPH-4: Adults with obesity and type 2 diabetes
April 2026 readouts showed mean weight reductions of 22–24% at the 12 mg dose over 68 weeks. A separate 18-month trial reported approximately 28% average weight loss — a figure that overlaps with bariatric surgical outcomes. By comparison, tirzepatide at 15 mg achieved roughly 21% in the SURMOUNT-1 trial.
These numbers reflect a steeper dose-response curve, suggesting the glucagon receptor arm continues contributing at higher doses rather than plateauing. Researchers tracking what is new in peptide research will recognize this as a meaningful pharmacological distinction.
As of mid-2026, retatrutide remains unapproved and commercially unavailable. An NDA submission to the FDA is planned for late 2026, with potential approval in 2027. For researchers evaluating multi-pathway compounds in parallel, the GLP-3 and incretin research themes overview provides useful context on where this compound fits within the broader incretin landscape.
Those building structured research protocols may also benefit from reviewing peptide therapy benefits and research methodology to understand how multi-receptor compounds are evaluated systematically.

Conclusion
The biology behind retatrutide is not complicated once the receptor targets are mapped clearly. GLP-1 reduces intake. GIP improves insulin dynamics. Glucagon raises energy output. Together, these three pathways explain why Phase 3 data consistently outperform single and dual agonist benchmarks.
Actionable next steps for researchers and informed readers in 2026:
- Distinguish GLP-2 (gut mucosal biology) from the GLP-1/GIP/glucagon triple-agonist mechanism before comparing compounds.
- Monitor the TRIUMPH program readouts and the anticipated FDA NDA submission timeline.
- Review MOTS-c metabolic flexibility research as a complementary pathway for researchers studying energy regulation.
- Use quality testing protocols as a benchmark when evaluating any research-grade peptide compound.
Retatrutide represents a genuine step-change in metabolic peptide science — not because it is newer, but because its receptor architecture addresses limitations that single and dual agonists cannot overcome.