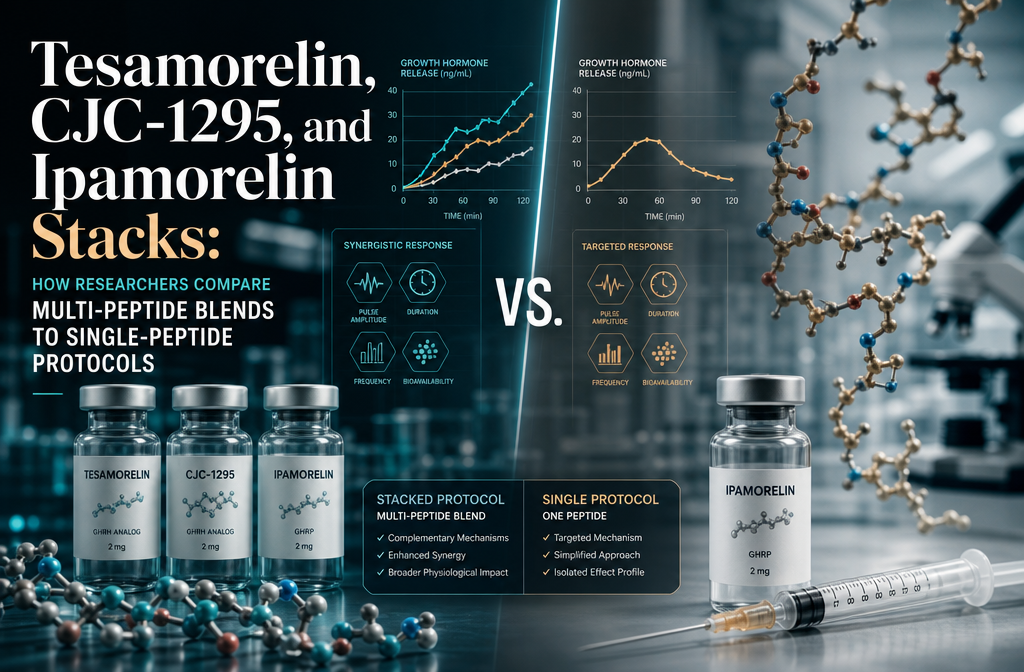
Tesamorelin, CJC‑1295, and Ipamorelin Stacks: How Researchers Compare Multi‑Peptide Blends to Single‑Peptide Protocols
{"cover":"Professional landscape format (1536×1024) hero image with bold text overlay: 'Peptide Stacks vs Single Protocols: Tesamorelin, CJC-1295 & Ipamorelin' in extra large 72pt white bold sans-serif font with dark semi-transparent overlay box, centered upper-third composition. Background shows a high-resolution laboratory research setting with glass vials, molecular structure diagrams, and soft blue lighting with white accents. Color palette: deep navy blue, crisp white, and teal highlights. Magazine cover aesthetic, editorial quality, high contrast.","content":["Detailed landscape format (1536×1024) scientific illustration showing three distinct peptide molecular structures labeled Tesamorelin, CJC-1295, and Ipamorelin arranged side by side with connecting arrows indicating GH-axis pathway activation. Background features a stylized pituitary gland diagram with GH pulse waveforms. Color scheme: clinical white, deep blue, and amber highlights. Infographic style with clean sans-serif annotations, research laboratory aesthetic, high detail.","Aerial top-down view of a researcher's desk showing a comparison chart contrasting single-peptide protocol data versus multi-peptide blend data, with bar graphs showing 17% VAT reduction figures, regulatory status badges (FDA-approved vs research chemical), and dose-sparing calculation notes on a digital tablet. Scattered research papers, a calculator, and peptide vials visible. Color palette: warm white desk surface, navy data graphics, green and red status indicators. Editorial research aesthetic.","Close-up wide-angle shot of a laboratory bench with precisely measured peptide vials arranged in a row showing dose-sparing blend formulations, a digital scale, and a research protocol notebook open to a page titled Multi-Peptide Stack Design Considerations. Soft overhead lighting with clinical blue-white tones. One vial labeled with a triple-blend formulation tag. Background shows blurred centrifuge equipment. Color scheme: sterile white, steel grey, and accent blue. High-resolution editorial quality."]
Only one peptide in the GH-secretagogue class has cleared the bar of FDA approval and multiple randomized controlled trials — and it is almost always studied alone. That single fact defines the central tension researchers face when evaluating Tesamorelin, CJC-1295, and Ipamorelin stacks: How researchers compare multi-peptide blends to single-peptide protocols reveals a sharp divide between what is clinically proven and what is mechanistically plausible.
Key Takeaways
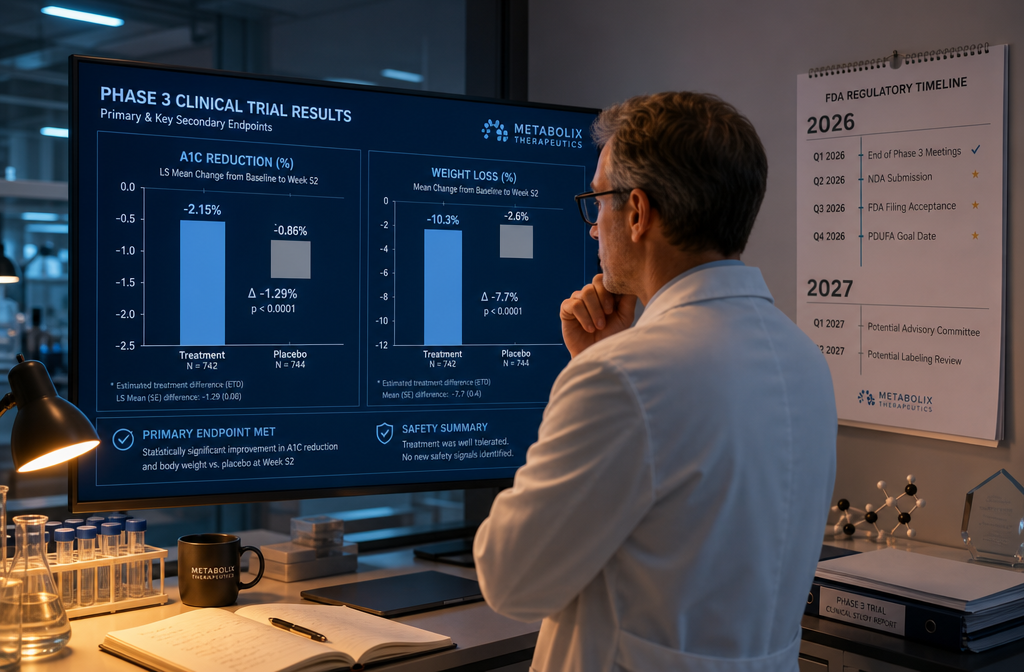
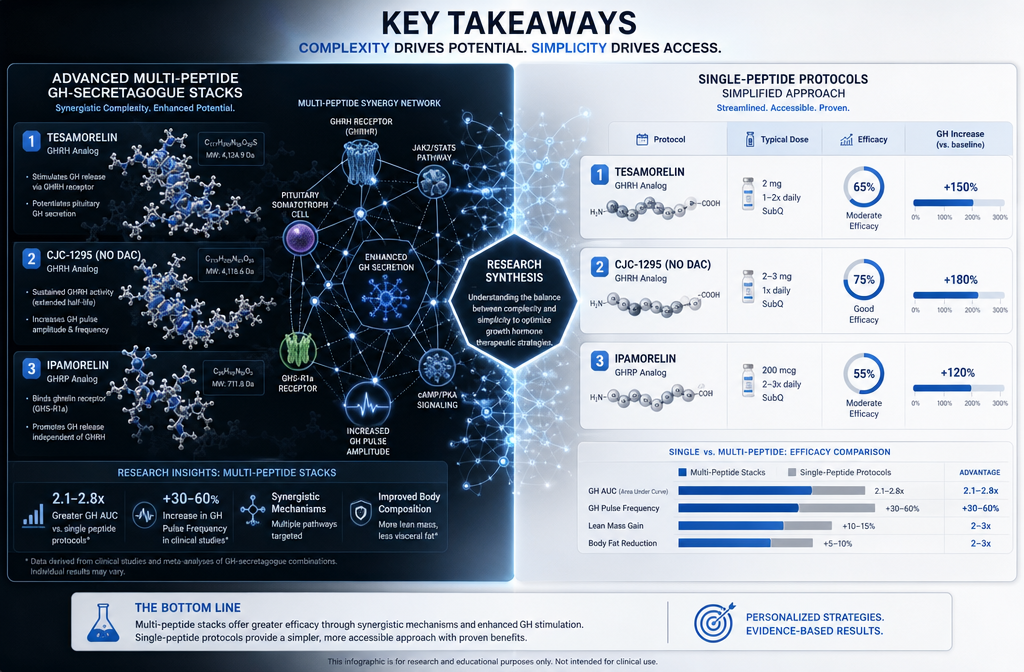
- Tesamorelin monotherapy has robust RCT evidence showing roughly 17% visceral adipose tissue (VAT) reduction at six months; no equivalent data exist for CJC-1295 or Ipamorelin stacks.
- CJC-1295 + Ipamorelin combinations sit in the lowest evidence tier for fat loss, classified as mechanistically plausible but clinically under-proven.
- Triple-blend stacks typically use lower individual doses than standalone protocols, reflecting a dose-sparing research strategy.
- Regulatory status differs sharply: tesa is FDA-approved for a specific indication; triple-peptide blends are research chemicals not approved for human use.
- Researchers choosing between protocols should match the peptide to the research question, not assume that more peptides equal better outcomes.
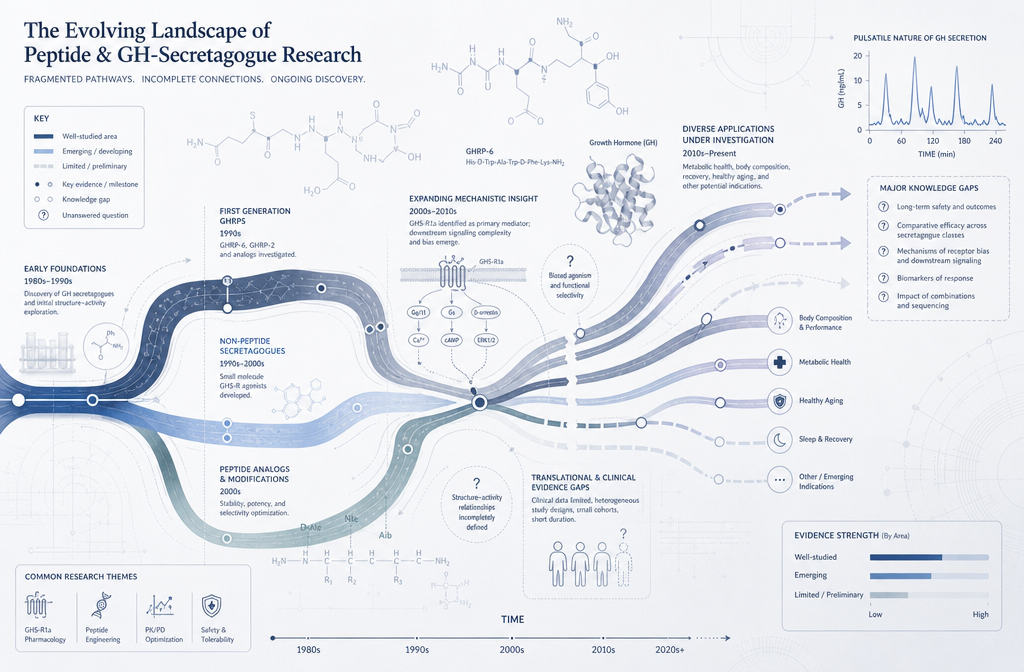
Understanding the Evidence Gap in GH-Secretagogue Research
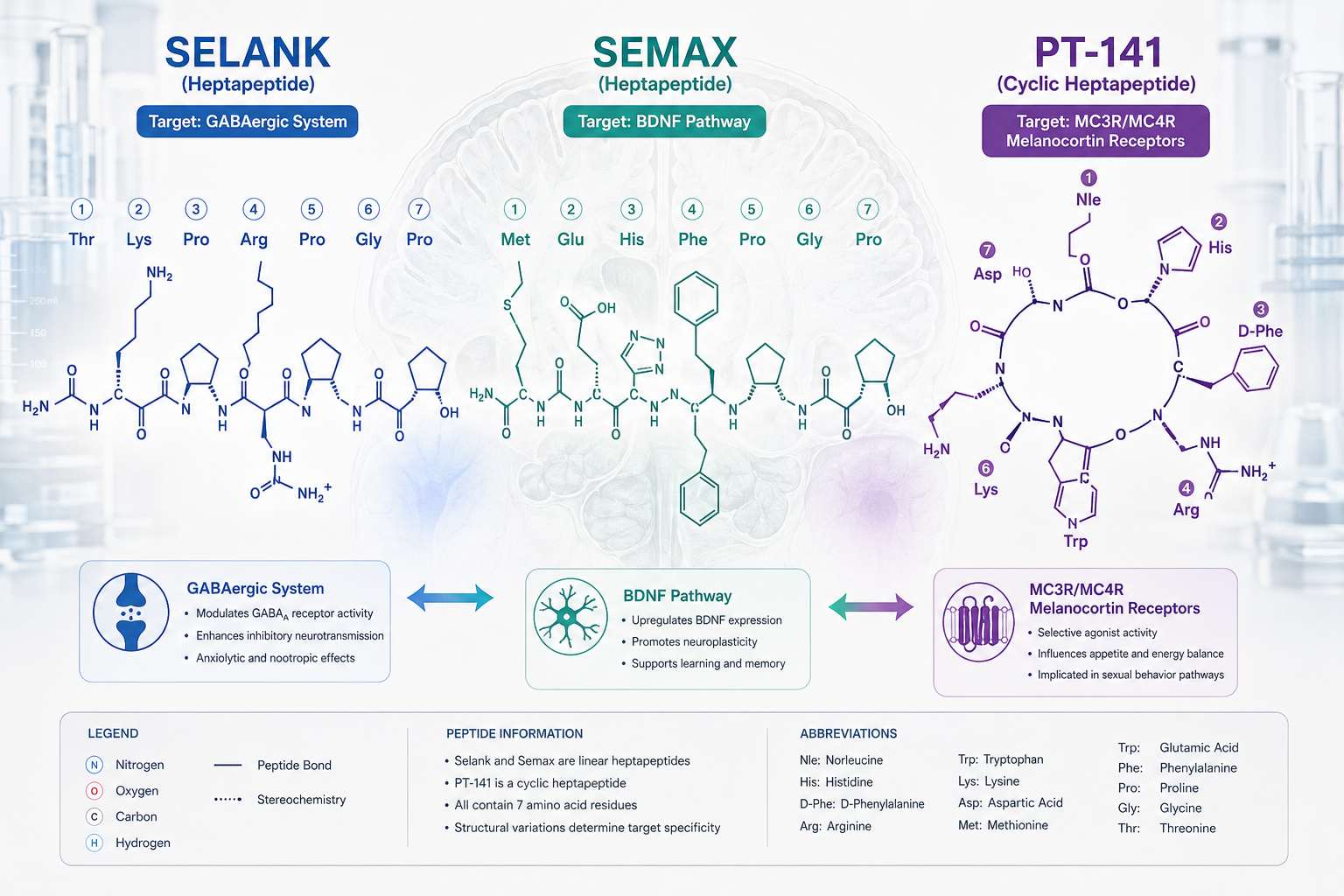
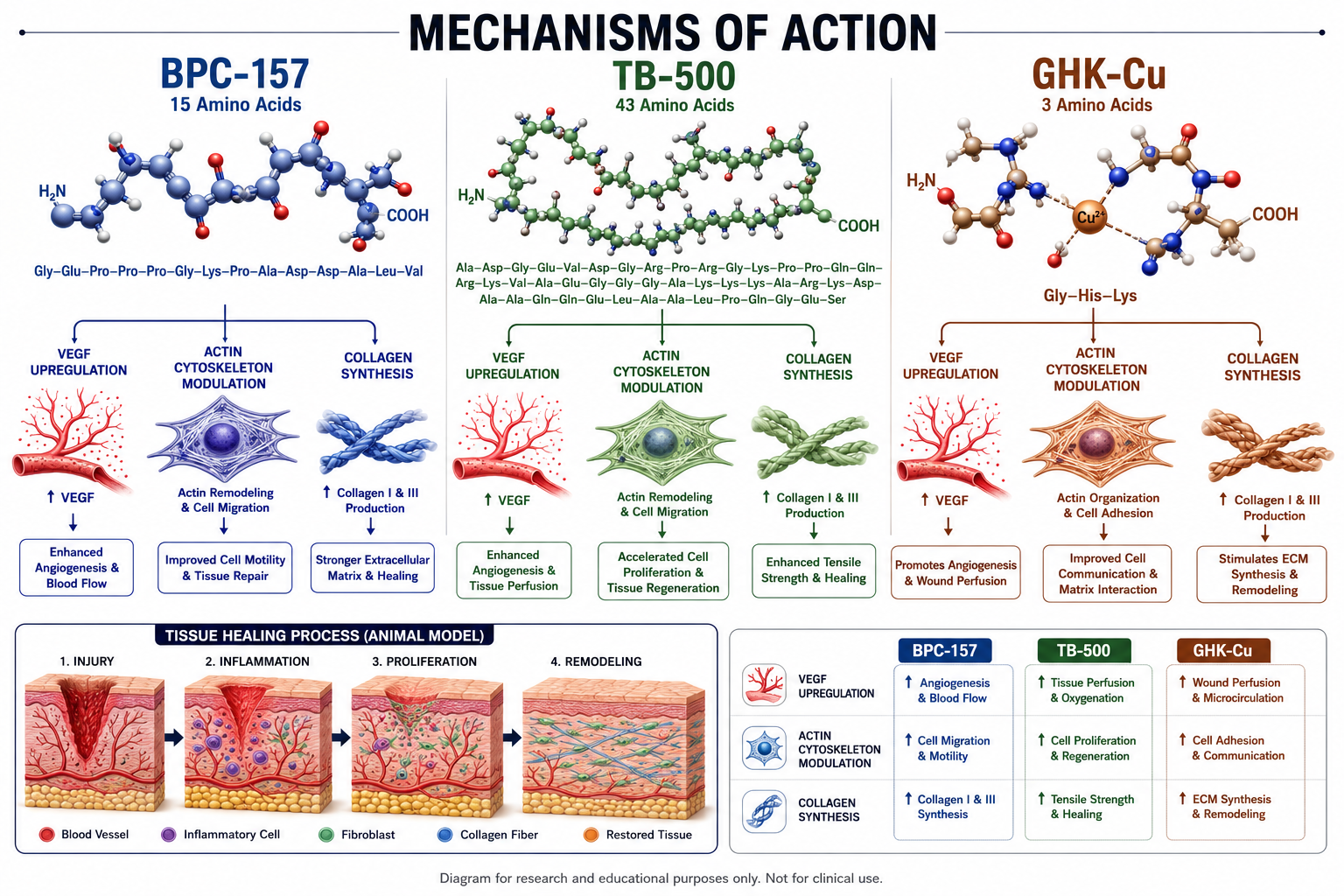
The GH axis can be stimulated through two distinct receptor pathways: GHRH receptors (targeted by tesa and CJC-1295) and ghrelin/GHS receptors (targeted by ipamorelin). On paper, combining both pathways makes sense — each amplifies GH pulse amplitude through a different mechanism, and preclinical data support synergistic GH release.
The problem is that synergistic GH release is a surrogate marker, not a clinical outcome. Tesamorelin's evidence base is built on hard endpoints. Pooled data from multiple randomized trials in patients with metabolic syndrome show approximately 17.2% VAT reduction at six months alongside meaningful improvements in HbA1c. These results come from tesa used as a monotherapy, not as part of a stack.
CJC-1295 and ipamorelin have no equivalent VAT-specific RCT data. Their reputation for supporting fat loss, lean mass, recovery, and sleep quality rests largely on:
- Surrogate biomarkers (IGF-1 elevation, GH pulse data)
- Small or open-label studies
- Extrapolation from tesa's mechanism
- Accumulated clinical experience rather than controlled outcomes
For researchers designing protocols, this distinction is not a minor detail — it determines what conclusions can legitimately be drawn from any experiment.
How Researchers Compare Multi-Peptide Blends to Single-Peptide Protocols: Regulatory and Dosing Frameworks
Regulatory status shapes research design as much as pharmacology does. Tesamorelin carries FDA approval for HIV-associated lipodystrophy, which means its dosing, monitoring parameters, and safety profile are well-characterized in published literature. Researchers using it off-label for visceral fat or metabolic endpoints have a defined framework to work within.
Triple-peptide blends — such as the tesa + CJC-1295 + ipamorelin 12mg blend — are explicitly classified as research chemicals not approved for human use. This status places them in a different methodological category. Researchers working with these compounds in preclinical or experimental models must account for the absence of standardized clinical dosing guidance.
When comparing the two approaches, a useful framework is the evidence tier system:
| Protocol Type | Evidence Tier | Key Data Source |
|---|---|---|
| Tesamorelin monotherapy | High | Multiple RCTs, meta-analyses |
| CJC-1295 + Ipamorelin stack | Low | Surrogate markers, case series |
| Tesamorelin + CJC-1295 + Ipamorelin triple blend | Lowest | Preclinical, mechanistic only |
Researchers exploring tesa vs ipamorelin as separate protocols will find that tesa is the evidence-based choice for visceral fat specifically, while ipamorelin-containing stacks are positioned more toward generalized recovery and lean-mass support — a distinction that should inform how any study is designed and how results are interpreted.
Practical Considerations When Designing Multi-Peptide GH Stack Protocols
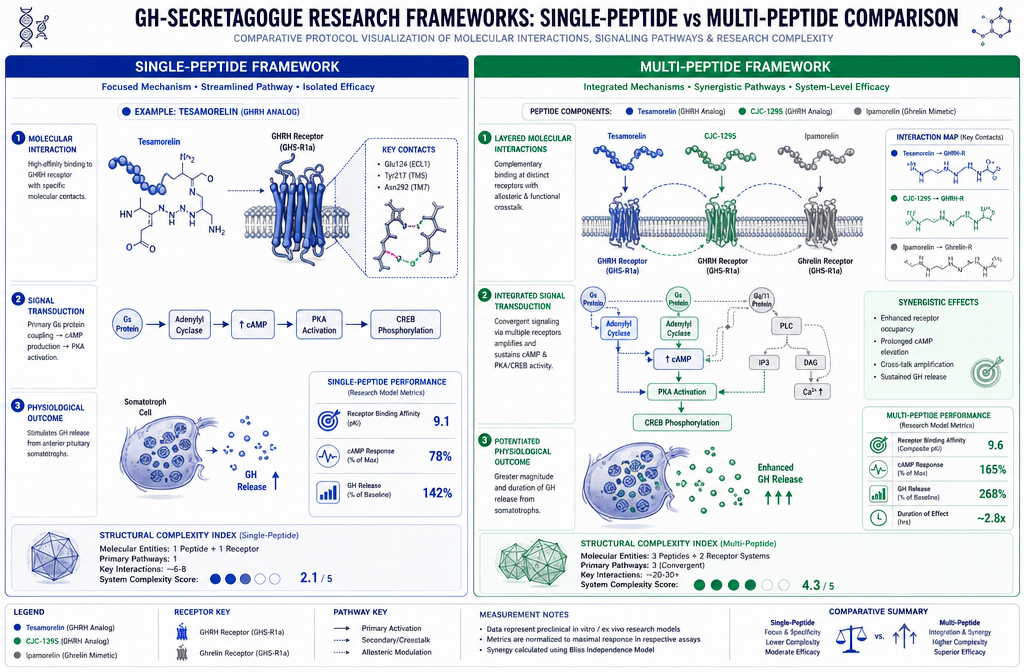
One consistent feature of triple-blend formulations is dose-sparing. Experimental profiles for the tesa + CJC-1295 + ipamorelin combination typically describe each component dosed below its usual standalone level — for example, tesa at 500–1,000 mcg alongside CJC-1295 and ipamorelin each at 100–200 mcg per administration. The rationale is multi-pathway stimulation without proportionally increasing total peptide load.
Researchers considering peptide blend research should weigh several practical factors:
- Research question specificity: If the target endpoint is visceral fat reduction, single-peptide tesa protocols have validated measurement tools and outcome benchmarks. Multi-peptide blends lack these reference points.
- Confounding variables: Stacking multiple peptides makes it harder to attribute any observed effect to a specific compound. Single-peptide protocols offer cleaner data.
- Dose-response clarity: Established tesa dosage guidance exists in the literature; equivalent guidance for triple blends does not.
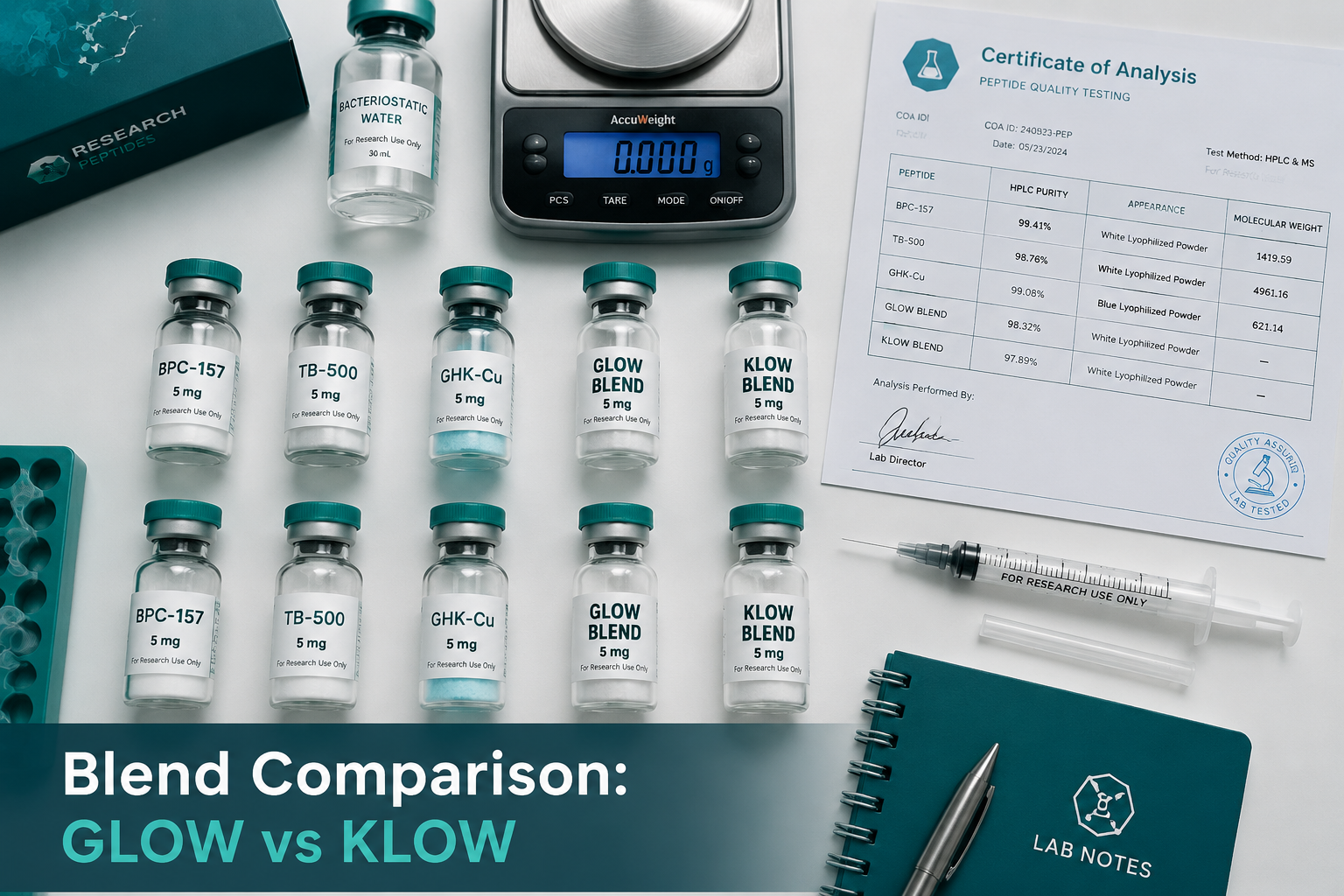
- Purity verification: Any multi-peptide blend used in research should come with third-party testing documentation. Reviewing quality testing protocols before sourcing is a critical step.
For researchers interested in broader GH-axis research design, the GH axis product line overview provides useful context on how different secretagogues fit within a structured research framework. Those exploring adjacent peptide categories may also find value in reviewing BPC-157 core peptides documentation for comparison on how single-peptide evidence builds over time.
Conclusion
The comparison between Tesamorelin, CJC-1295, and Ipamorelin stacks and single-peptide protocols ultimately comes down to matching the tool to the task. Tesamorelin monotherapy remains the gold standard for visceral fat research, backed by rigorous clinical trial data. CJC-1295 and ipamorelin combinations offer mechanistic appeal and broader GH-axis stimulation, but researchers must work with the understanding that combination data are thin and clinical outcomes are largely unproven.
Actionable next steps for researchers in 2026:
- Define the primary endpoint before selecting a protocol — visceral fat reduction favors tesa alone; recovery and lean-mass models may justify a stack design.
- Use single-peptide runs first to establish baseline response data before introducing multi-peptide complexity.
- Source only third-party tested compounds and document purity for every experimental batch.
- Treat any triple-blend result as hypothesis-generating, not confirmatory, until controlled studies exist.
The gap between mechanistic plausibility and clinical proof is where most peptide stack research currently lives. Acknowledging that gap is the first step toward designing studies that actually close it.