PT-141, Tadalafil, and Sildenafil in Erectile Function Research: When Do Peptides Outperform Pills in Preclinical Models?
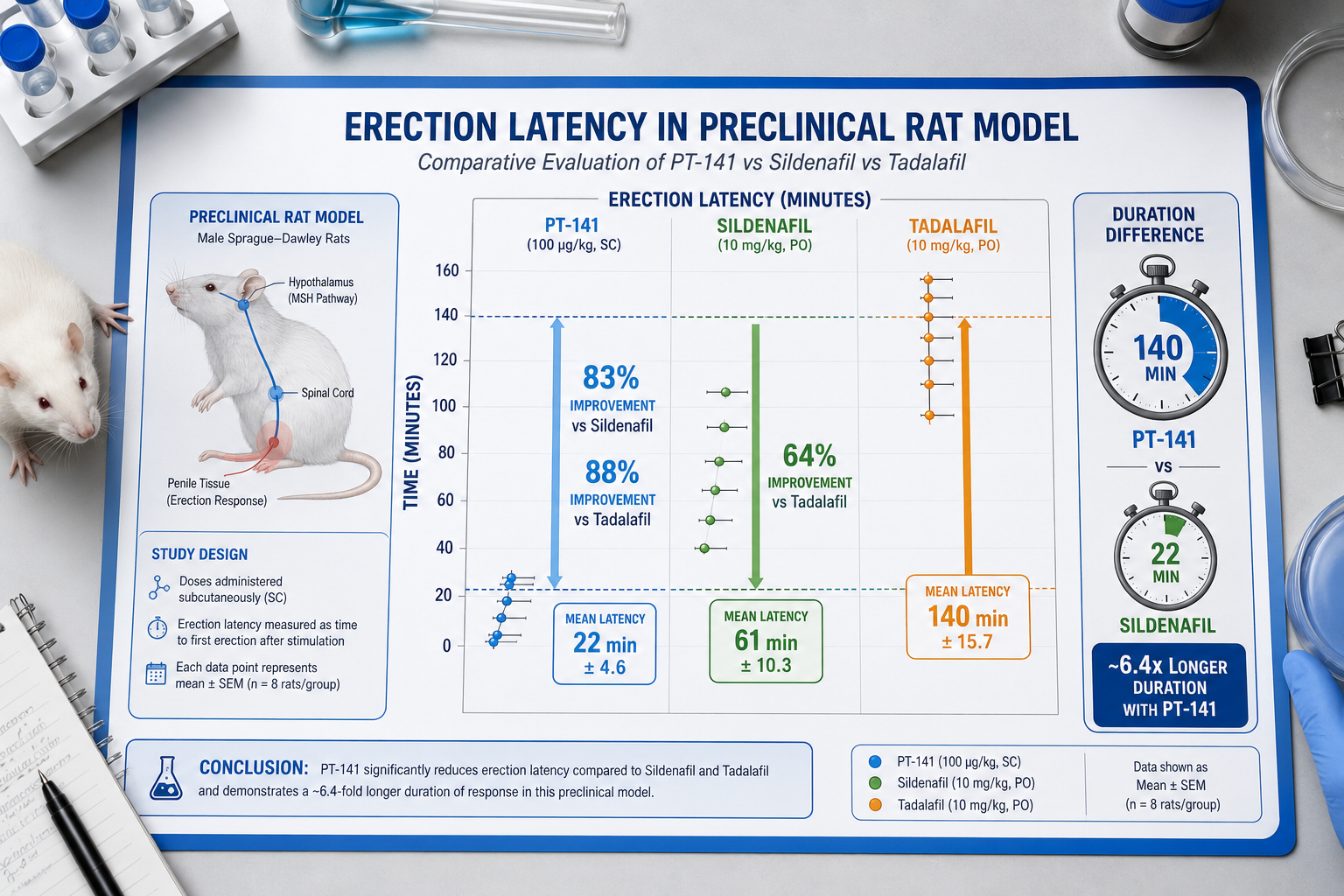
Erection duration in a PT-141-treated group ran approximately 140 minutes in controlled trials — compared to just 22 minutes in the placebo group. That single data point raises a mechanistically important question for researchers studying erectile function: does a centrally acting peptide offer advantages that peripheral vasodilators simply cannot replicate? Exploring PT-141, Tadalafil, and Sildenafil in Erectile Function Research — specifically when peptides outperform pills in preclinical models — requires a close look at receptor biology, pathway architecture, and what animal data actually show.
Key Takeaways
- PT-141 (bremelanotide) acts centrally through melanocortin receptors MC3R and MC4R, while tadalafil and sildenafil act peripherally via PDE5 inhibition.
- Preclinical rodent models show PT-141 significantly increases spontaneous erection frequency through central neural pathways.
- PT-141 has demonstrated erectile responses in sildenafil non-responders, suggesting a non-overlapping mechanism.
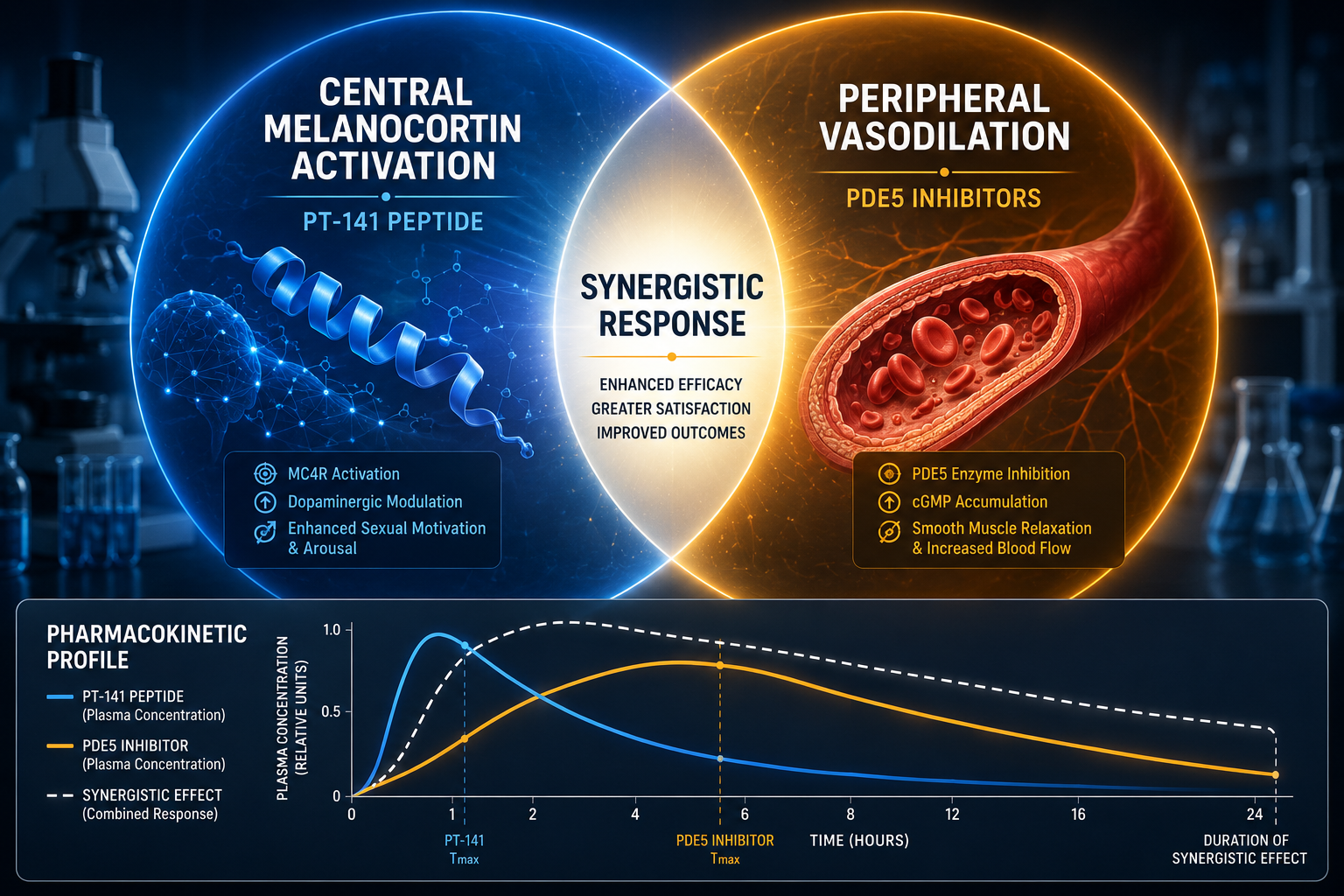
- Combination data indicate a synergistic effect when PT-141 and sildenafil are co-administered.
- Mechanistic divergence makes these compounds complementary research tools rather than simple substitutes.
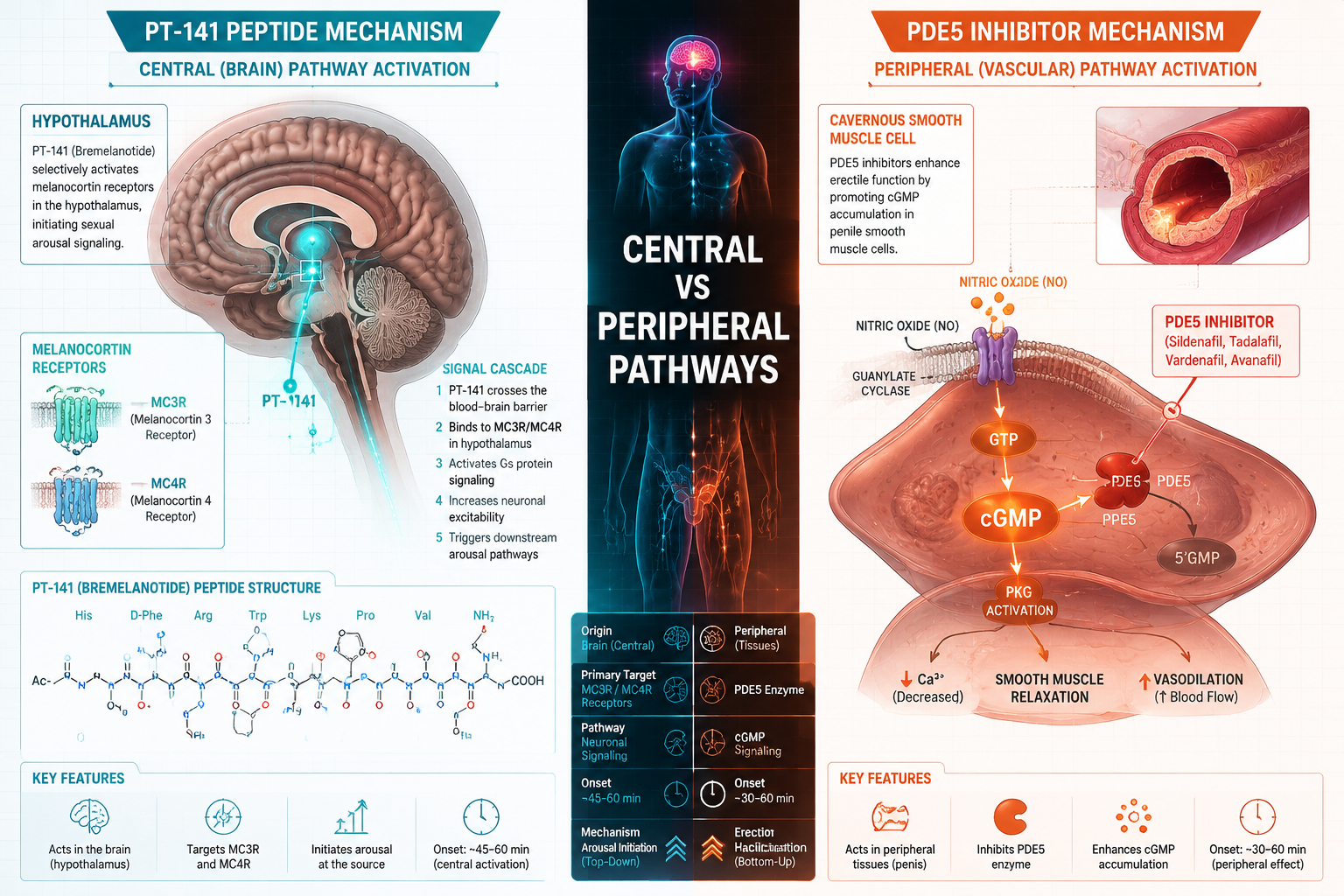
Mechanistic Divergence: Central Peptide vs. Peripheral Pill
The foundational difference between PT-141 and PDE5 inhibitors lies in where each compound acts.
Sildenafil and tadalafil both inhibit phosphodiesterase type 5, preventing the breakdown of cyclic GMP (cGMP) in penile smooth muscle. This prolongs nitric oxide-driven vasodilation and facilitates engorgement — but the pathway depends entirely on prior sexual stimulation to generate nitric oxide in the first place. Without that upstream signal, PDE5 inhibitors have limited effect.
PT-141, by contrast, is a synthetic melanocortin receptor agonist. It binds preferentially to MC3R and MC4R in the central nervous system, particularly in hypothalamic regions associated with sexual arousal circuitry. This central activation can initiate an erectile response independent of peripheral vascular priming.
"PT-141 does not require nitric oxide as a prerequisite signal — it bypasses the peripheral dependency entirely."
This mechanistic split is why researchers studying neurogenic or psychogenic components of erectile dysfunction find PT-141 particularly informative as a research tool. For a broader overview of how peptides interact with neuroendocrine pathways, the PT-141 central arousal research overview provides useful context.
What Preclinical Models Reveal About PT-141, Tadalafil, and Sildenafil in Erectile Function Research: When Do Peptides Outperform Pills in Preclinical Models?
Animal models — primarily rodents — have been the primary setting for comparing these compounds mechanistically.
Rodent Erection Latency and Frequency Data
In rat studies, intranasal PT-141 administration produced a statistically significant increase in spontaneous erection frequency compared to vehicle controls. The response did not require external stimulation, which directly mirrors its central mechanism. PDE5 inhibitors in the same models show weaker spontaneous erection induction, reinforcing that their efficacy is stimulus-dependent.
| Parameter | PT-141 | Sildenafil | Tadalafil |
|---|---|---|---|
| Primary site of action | CNS (MC3R/MC4R) | Peripheral (PDE5) | Peripheral (PDE5) |
| Stimulus dependency | Low | High | High |
| Erection latency reduction | Significant | Moderate | Moderate |
| Duration advantage | Extended | Moderate | Extended (longer half-life) |
Non-Responder Models
A critical finding in the research literature involves subjects with inadequate responses to sildenafil. Subcutaneous PT-141 at 4 mg and 6 mg doses produced statistically significant erectile responses in this population. This is a mechanistically logical result: if the peripheral pathway is compromised (vascular insufficiency, receptor downregulation), central activation via melanocortin signaling offers an alternative route.
Researchers interested in PT-141 peptide for research contexts will find this non-responder data particularly relevant for experimental design.
Synergy Data and Combination Research Findings
One of the more compelling findings in this research area involves co-administration. A crossover study using 25 mg sildenafil combined with 7.5 mg intranasal PT-141 produced a significantly greater erectile response than sildenafil alone. This synergy is mechanistically coherent: PT-141 amplifies the central arousal signal while sildenafil sustains the peripheral vascular response once initiated.
This complementary profile suggests that in preclinical research designs, combining a melanocortin agonist with a PDE5 inhibitor can model the full erectile pathway — central initiation plus peripheral amplification — more completely than either agent alone.
For researchers building multi-peptide experimental frameworks, resources like the ultimate guide to peptide therapy research offer broader context on stacking and synergy considerations.
Pharmacokinetics and Practical Research Considerations
PT-141's pharmacokinetic profile adds another dimension to its research utility. Following intranasal administration, peak serum concentrations occur roughly 30 minutes post-dose, with a half-life of approximately 2 hours. This rapid onset supports time-locked experimental protocols where researchers need a predictable arousal window.
Tadalafil's much longer half-life (17–21 hours) makes it better suited for studies examining sustained vascular tone, while sildenafil's intermediate profile (~4 hours) fits acute response models.
Key pharmacokinetic comparison:
- PT-141: Onset ~30 min, half-life ~2 hours, central action
- Sildenafil: Onset ~30–60 min, half-life ~4 hours, peripheral action
- Tadalafil: Onset ~1–2 hours, half-life ~17–21 hours, peripheral action
Researchers sourcing research-grade peptides should prioritize verified purity documentation. The PT-141 for sale research page and PT-141 for sale online resources outline quality control considerations relevant to preclinical work.
Safety data from controlled studies show no significant hemodynamic changes with PT-141 at research-relevant doses, which contrasts with PDE5 inhibitors that can produce measurable blood pressure effects — an important variable to control in animal models.
For researchers also examining mitochondrial or vascular biology alongside erectile function research, SS-31 mitochondrial dynamics research offers a complementary mechanistic lens on vascular tissue health.
Conclusion
The comparison of PT-141, Tadalafil, and Sildenafil in Erectile Function Research — specifically when peptides outperform pills in preclinical models — points to one clear answer: PT-141 outperforms PDE5 inhibitors when the research question centers on central arousal mechanisms, stimulus-independent erection induction, or non-responder populations. PDE5 inhibitors remain superior tools for studying peripheral vascular amplification and sustained engorgement.
Actionable next steps for researchers in 2026:
- Design experiments that isolate central versus peripheral pathways using PT-141 and PDE5 inhibitors as mechanistic controls.
- Use non-responder models to probe the independence of melanocortin-driven arousal from nitric oxide availability.
- Consider combination protocols when the research goal is modeling the full erectile response arc.
- Verify peptide purity through certificate of analysis documentation before any preclinical use.
Understanding where each compound excels mechanistically — rather than treating them as interchangeable — produces more precise, reproducible preclinical data.