BPC-157 vs TB-500: What Each Peptide Does in Tissue-Repair Research and When Comparison Makes Sense
Over 100 preclinical studies have examined BPC-157 alone — yet researchers still routinely pair it with TB-500 in comparative models. Understanding why requires looking at what each peptide actually does at the biological level. This article examines the BPC-157 vs TB-500 question from an experimental logic standpoint: what each compound is believed to do, where their mechanisms overlap, and when a side-by-side comparison genuinely adds scientific value in tissue-repair research.
Key Takeaways
- BPC-157 is a 15-amino-acid synthetic peptide that primarily drives localized repair through angiogenesis and nitric oxide signaling.
- TB-500 is a synthetic fragment of Thymosin Beta-4 that promotes systemic healing by regulating actin polymerization and cell migration.
- Their tissue targets differ: BPC-157 favors tendons, ligaments, and gut tissue; TB-500 shows stronger signals in muscle, skin, and cardiac tissue.
- Neither peptide is FDA-approved; both are prohibited by WADA under the S0 category for non-approved substances.
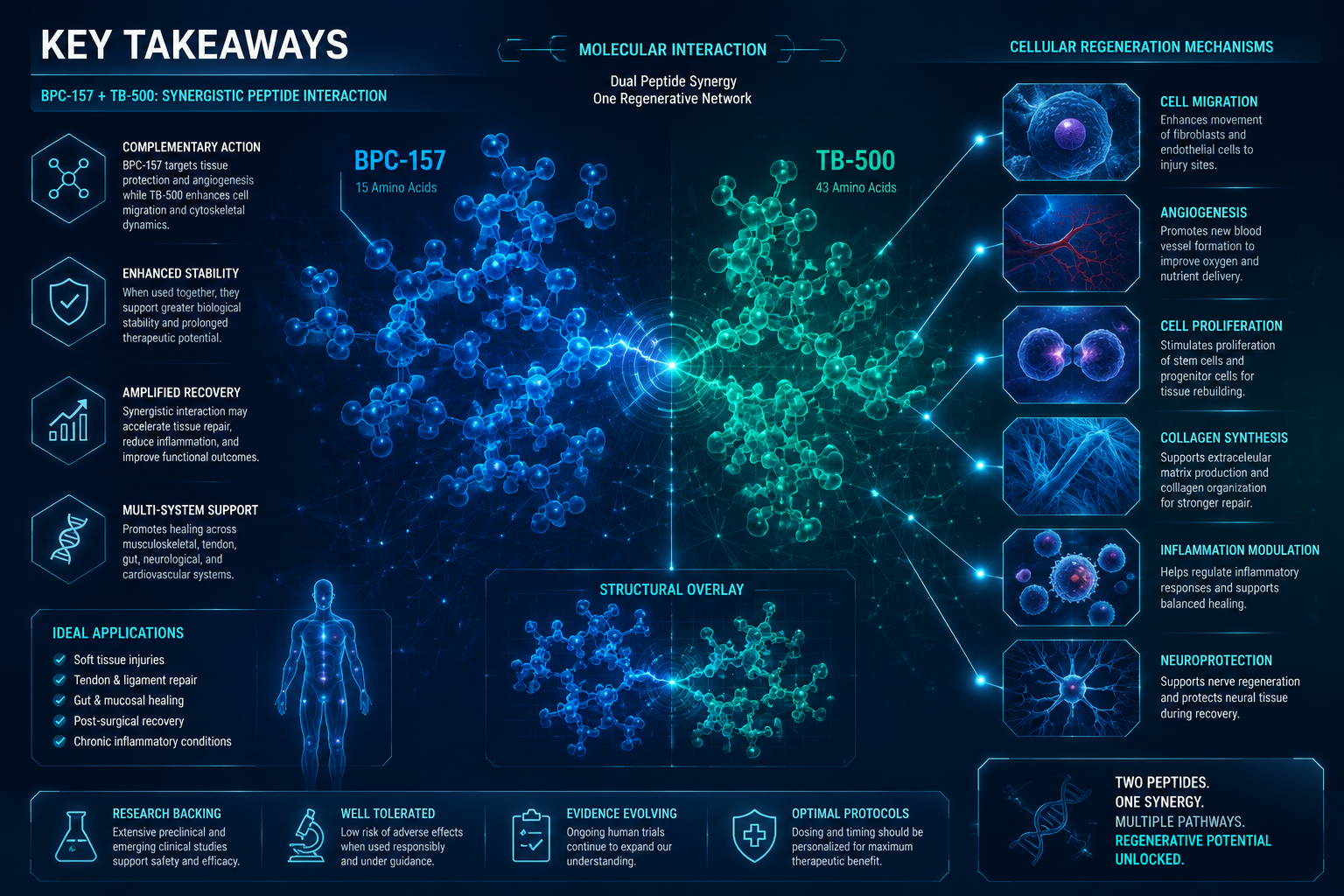
- Combination research suggests complementary, potentially synergistic effects — making the comparison scientifically meaningful rather than arbitrary.
Distinct Mechanisms: Where the Biology Diverges
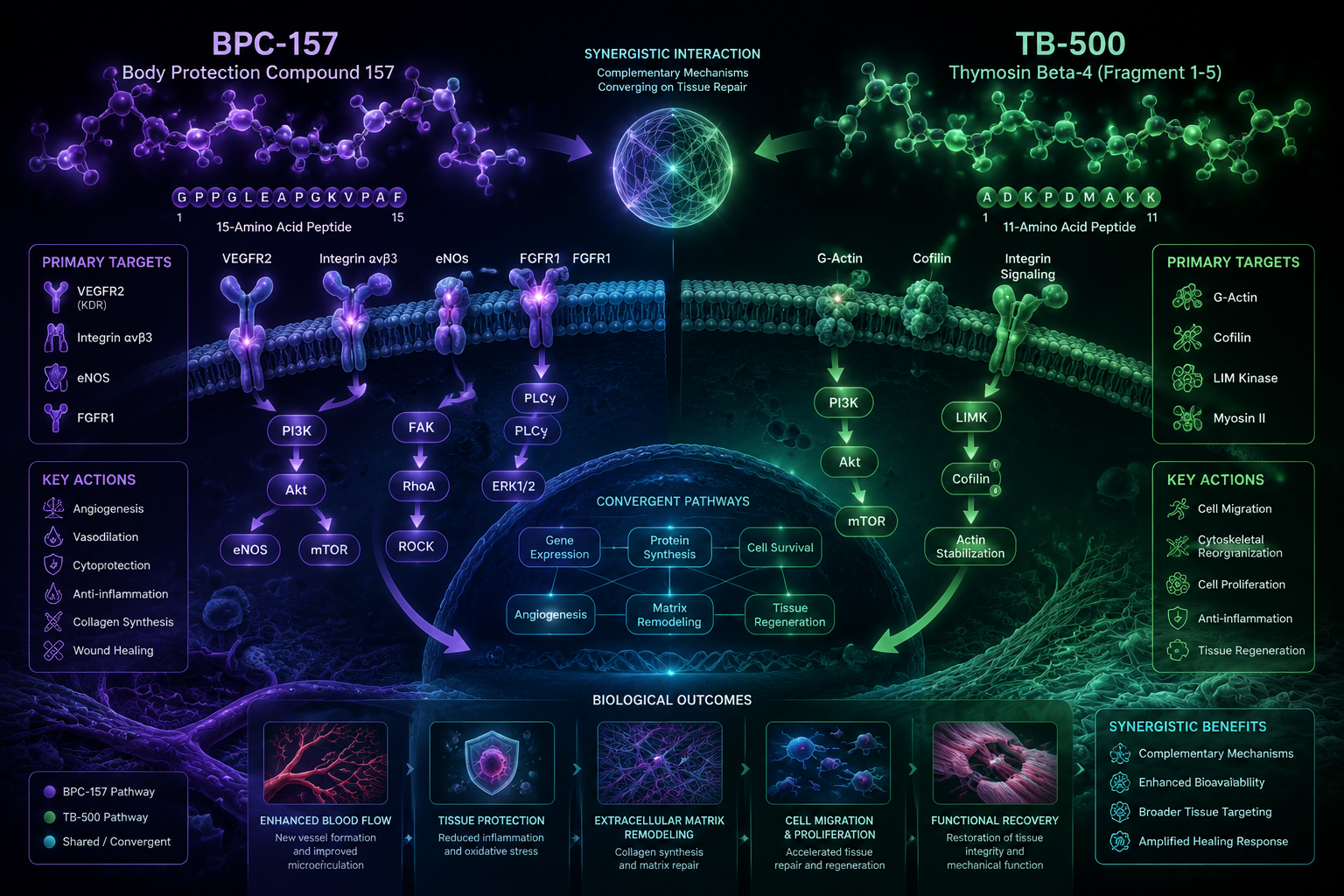
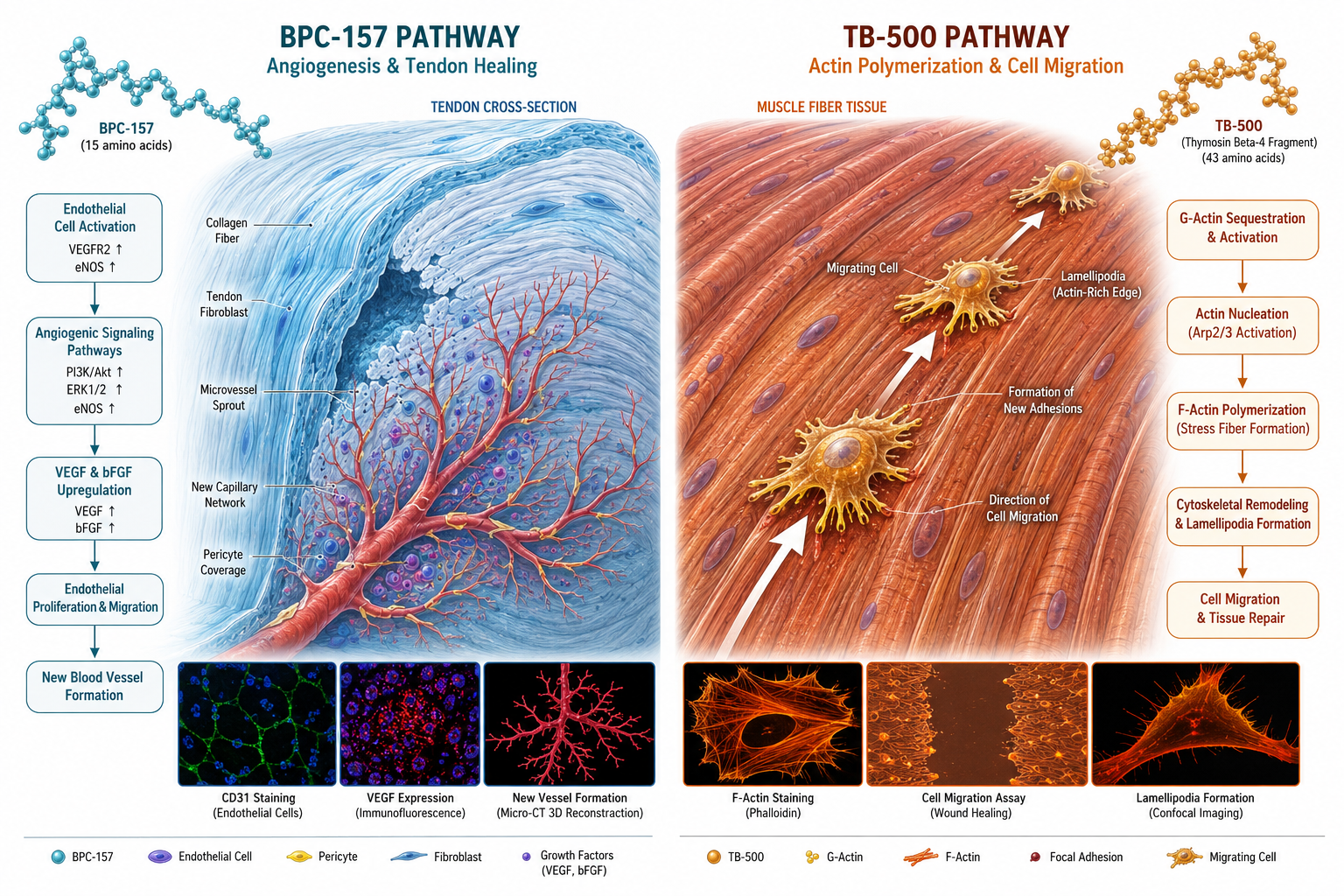
The BPC-157 vs TB-500 comparison starts with fundamentally different molecular strategies. BPC-157 is a synthetic 15-amino-acid sequence derived from human gastric juice protein. Its primary repair actions are believed to operate through angiogenesis — the formation of new blood vessels — and upregulation of nitric oxide pathways. This makes its effects highly localized. When administered near an injury site, it appears to accelerate the vascular supply that damaged tissue needs to regenerate.
TB-500, by contrast, is a synthetic fragment of Thymosin Beta-4, a naturally occurring protein found throughout the body. Its core mechanism involves regulating actin polymerization — the process by which cells build their internal scaffolding. By influencing actin dynamics, TB-500 enhances cell migration, which is essential for systemic wound repair. Because it distributes broadly after administration, its effects are not limited to the injection site.
Key mechanistic differences at a glance:
| Feature | BPC-157 | TB-500 |
|---|---|---|
| Origin | Gastric juice protein fragment | Thymosin Beta-4 fragment |
| Primary mechanism | Angiogenesis, nitric oxide signaling | Actin polymerization, cell migration |
| Distribution | Localized | Systemic |
| Half-life (IV, animal models) | Under 30 minutes | Not precisely established |
For researchers exploring BPC-157 angiogenesis and tendon repair mechanisms, this localized vascular focus is the defining biological signature.
Tissue Targets and Preclinical Evidence
Tissue specificity is where the BPC-157 vs TB-500 comparison becomes most practically useful for research design. BPC-157 has shown the strongest preclinical signals in tendon, ligament, and gastrointestinal tissue. Its gastric origin may partly explain its documented activity in gut-lining repair models. TB-500, on the other hand, demonstrates more consistent effects in muscle, skin, and cardiac tissue — areas where widespread cell migration drives recovery.
This tissue-level divergence is important because it shapes which model a researcher would choose when designing an experiment. A tendon repair study and a cardiac wound model are asking very different biological questions, and selecting the wrong peptide as a comparator can produce misleading null results.
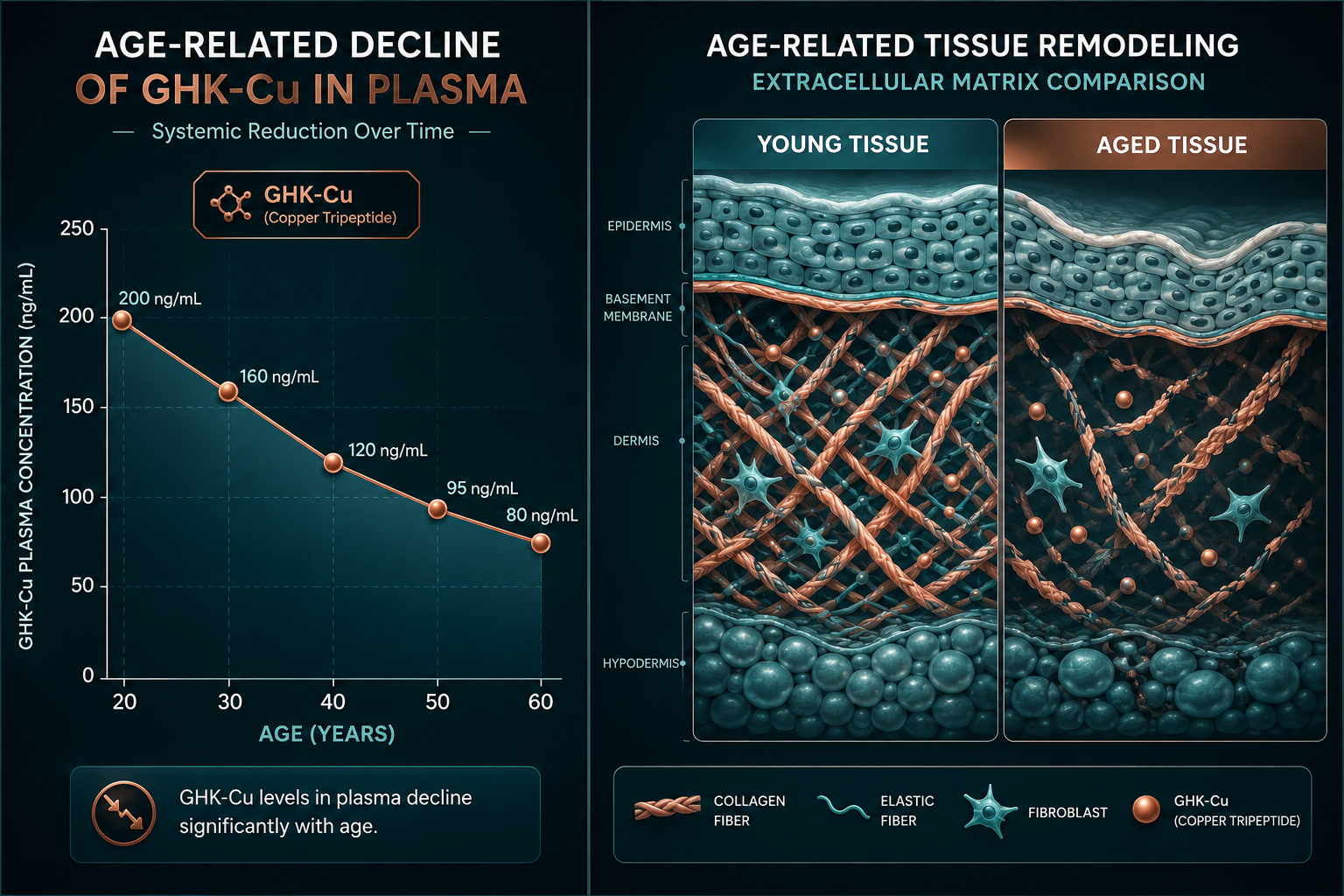
Both peptides have been studied in the context of inflammation reduction, which creates a genuine area of mechanistic overlap. This overlap is part of why top healing peptides in research contexts are often discussed together. Researchers interested in broader repair biology may also find value in examining GHK-Cu longevity and tissue research themes as a complementary reference point.

When the BPC-157 vs TB-500 Comparison Makes Sense in Research
Not every study benefits from comparing these two peptides directly. The comparison makes the most experimental sense under three conditions:
- Overlapping injury context — When the target tissue receives input from both vascular supply (BPC-157's domain) and cell migration (TB-500's domain), a head-to-head model can isolate which mechanism contributes more.
- Combination hypothesis testing — Preclinical data suggest that using both peptides together may produce synergistic repair outcomes. Testing this requires understanding each compound's independent effect first.
- Systemic vs. localized repair questions — When a study needs to distinguish between localized and body-wide healing responses, these two peptides serve as useful biological contrasts.
Regulatory context matters here. Neither BPC-157 nor TB-500 is FDA-approved. BPC-157 holds a Category 2 bulk drug substance classification, and both are prohibited under WADA's S0 category. Any research use must account for these regulatory boundaries.
For context on how other repair-relevant peptides are positioned in research, the oral BPC-157 research overview and longevity peptide research themes offer useful framing. Researchers sourcing verified compounds may also want to review lab-tested peptides to ensure research-grade purity standards.
Conclusion
The BPC-157 vs TB-500 comparison is not a matter of which peptide is "better." It is a question of biological fit. BPC-157 operates locally through vascular and nitric oxide pathways; TB-500 acts systemically through actin dynamics and cell migration. Their tissue targets differ, their pharmacokinetics differ, and their research applications reflect those differences.
Actionable next steps for researchers:
- Define the target tissue and injury type before selecting a comparator model.
- Review the preclinical literature for each peptide's specific tissue signals before designing combination studies.
- Confirm regulatory classification in the relevant jurisdiction before initiating any research protocol.
- Prioritize verified, purity-tested compounds to ensure data integrity across experimental runs.
The comparison makes scientific sense when the research question genuinely spans both localized and systemic repair biology. In those contexts, studying these two peptides together is not redundant — it is the most informative approach available.