
Retatrutide Side Effects, Tolerability, and Dose Escalation: What the Clinical Literature Shows
Sixty percent of participants on the highest retatrutide dose reported nausea in Phase 2 trials. That single data point tells you more about managing this triple-receptor agonist than any headline about weight loss ever could. For clinicians, researchers, and informed readers, understanding Retatrutide Side Effects, Tolerability, and Dose Escalation: What the Clinical Literature Shows is the essential starting point before any other conversation about this compound.
Key Takeaways
- Gastrointestinal adverse events are the most common side effects and are strongly dose-dependent.
- Dysesthesia (abnormal skin sensation) is a unique side effect not seen with semaglutide or tirzepatide.
- Slow, structured dose escalation is the primary strategy for improving tolerability.
- Most adverse events are mild to moderate and tend to decrease after the titration phase.
- Understanding the adverse-event profile helps set realistic expectations for any research or clinical context.
The Gastrointestinal Adverse Event Profile
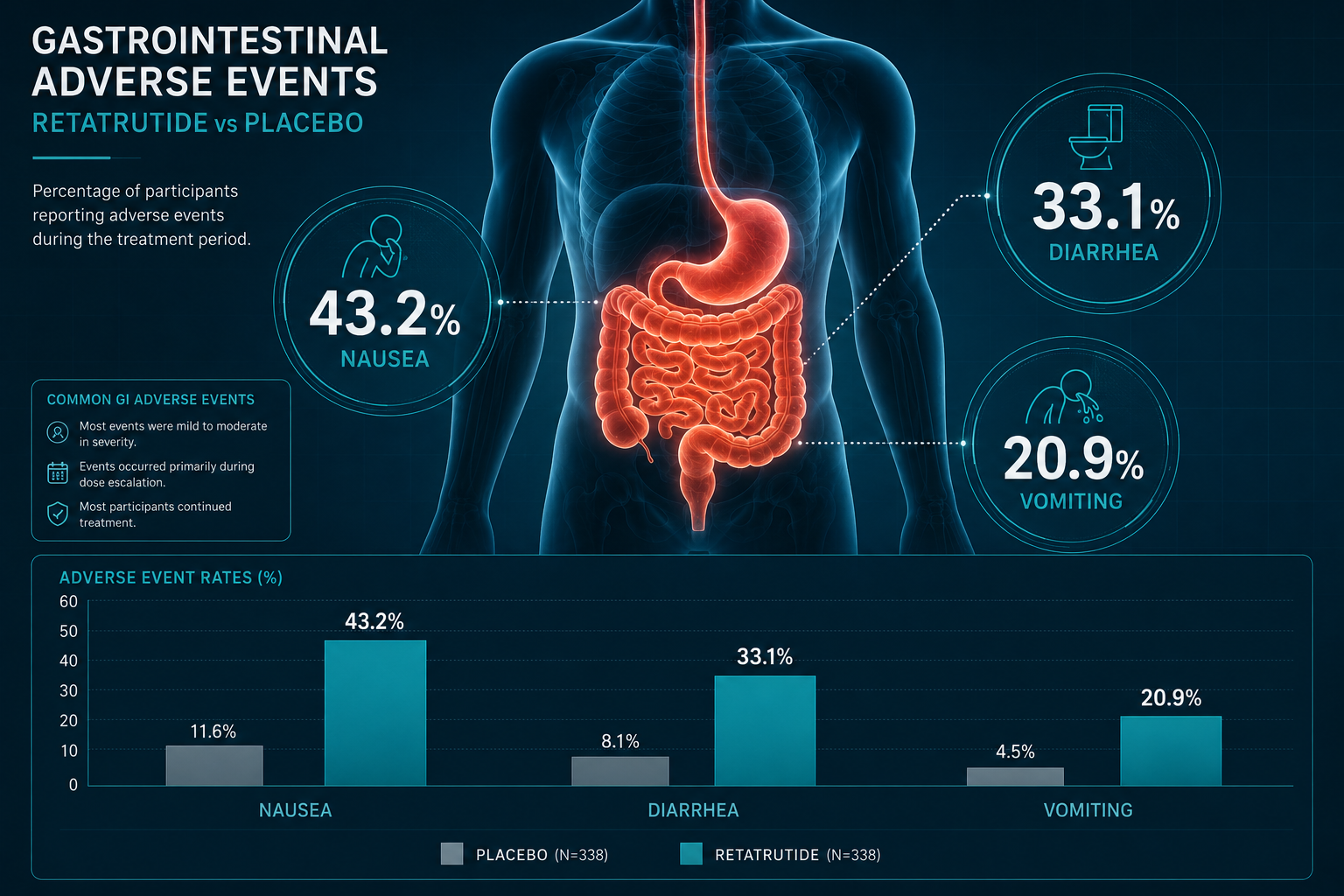
The dominant safety signal across all retatrutide trials is gastrointestinal (GI) in nature. In the TRIUMPH-4 Phase 3 trial, participants receiving the 12 mg dose reported the following rates compared to placebo:
| Adverse Event | Retatrutide 12 mg | Placebo |
|---|---|---|
| Nausea | 43.2% | 10.7% |
| Diarrhea | 33.1% | 13.4% |
| Constipation | 25.0% | 8.7% |
| Vomiting | 20.9% | 0.0% |
| Decreased appetite | 18.2% | 9.4% |
These numbers are significant but not unexpected. Retatrutide activates three receptors simultaneously: GLP-1, GIP, and glucagon. This triple-agonist mechanism, which you can explore further through the GLP-3 retatrutide research overview, amplifies both efficacy and GI burden compared to single or dual-receptor agents.
It is also worth noting how retatrutide compares within the broader evolution of incretin-based therapies. The generations of GLP-1 receptor agonists page provides useful context for how each new class has shifted the tolerability landscape.
"The GI side effect profile of retatrutide is consistent with its mechanism but is meaningfully more pronounced at higher doses than what is observed with dual agonists."
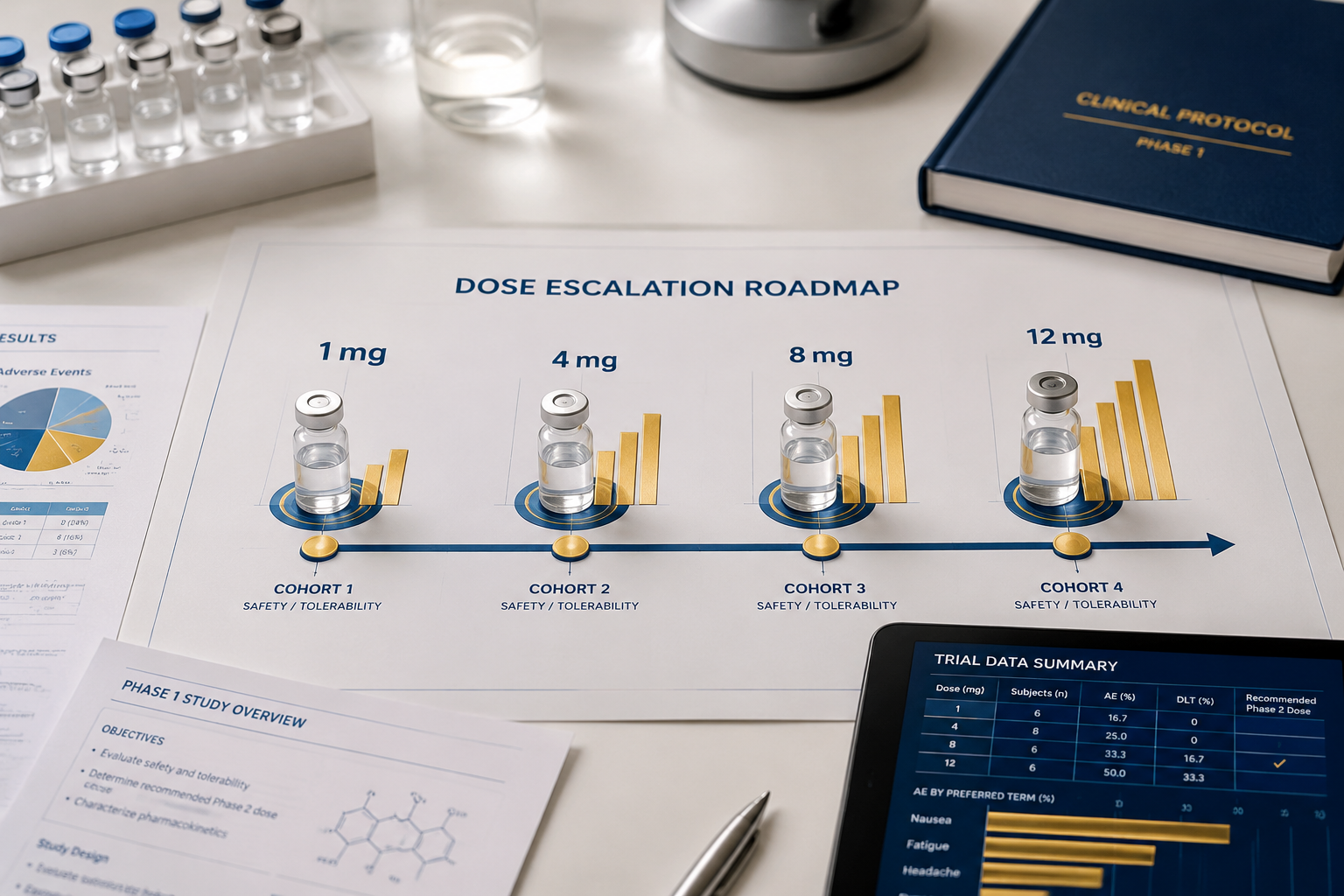
Dose-Dependent Tolerability: What the Phase 2 Data Reveals
One of the clearest findings from the TRIUMPH-1 Phase 2 trial is that side effects scale with dose. The nausea data across dose groups tells a direct story:
- 1 mg dose: 14% reported nausea
- 4 mg dose: 36% reported nausea
- 8 mg dose: 44% reported nausea
- 12 mg dose: 60% reported nausea
Diarrhea followed a less linear pattern, peaking at the 4 mg and 8 mg doses (both at 20%) before dropping slightly at 12 mg (15%), which may reflect GI adaptation over time.
This dose-response relationship is the primary reason that structured titration protocols exist. Gradual escalation allows the body to adapt to receptor activation before reaching therapeutic doses. Researchers interested in how similar peptide compounds handle titration can review CJC-1295 with DAC research findings for comparative context on incremental dosing strategies.
Understanding the GIP receptor and its importance also helps explain why the GI burden of retatrutide differs from GLP-1-only agents. GIP receptor co-activation affects gastric emptying and gut motility in ways that compound the nausea signal.
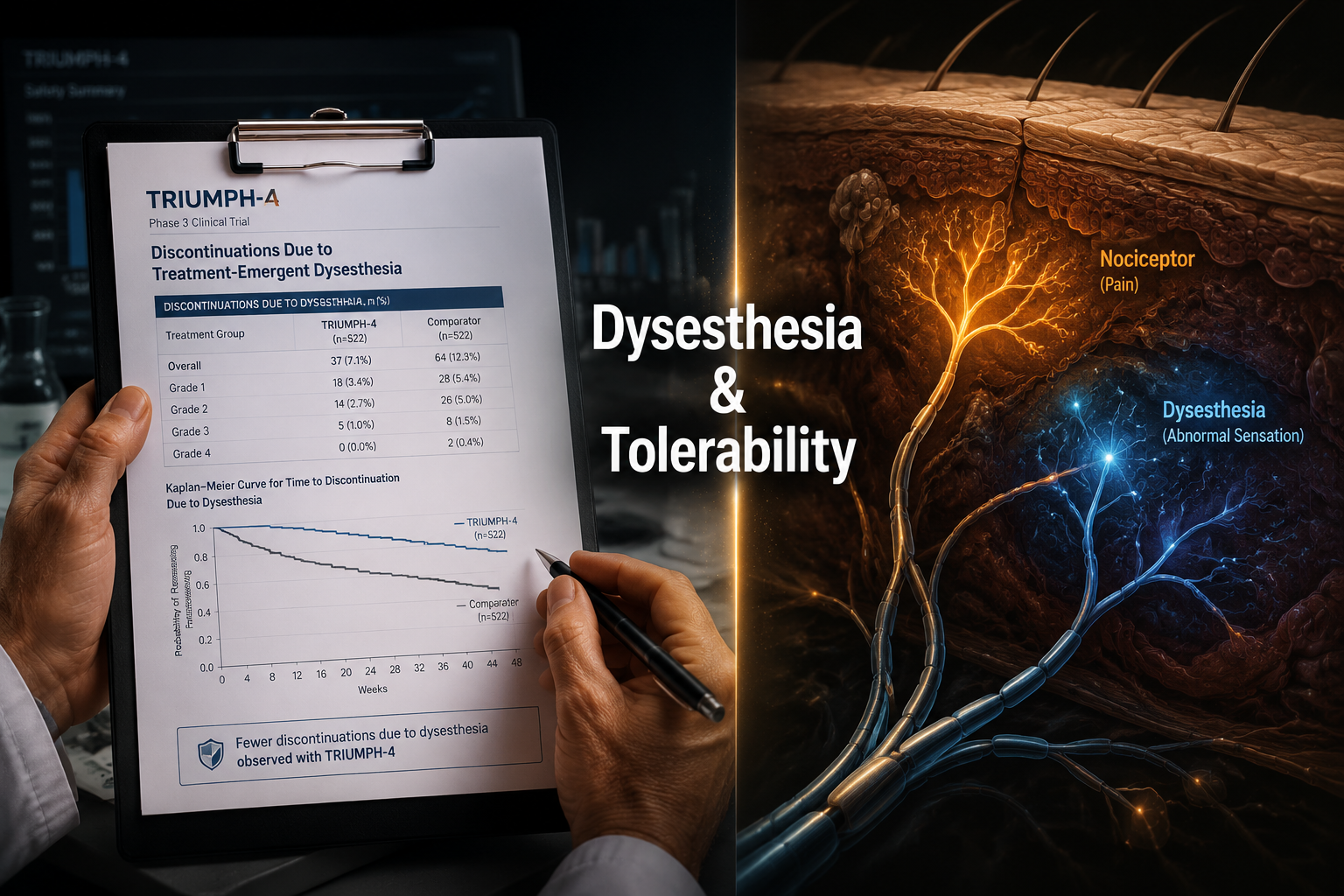
Dysesthesia and Other Notable Findings in Retatrutide Side Effects, Tolerability, and Dose Escalation
Beyond GI effects, dysesthesia stands out as a clinically distinctive finding. In TRIUMPH-4, 20.9% of participants on the 12 mg dose reported this abnormal skin sensation, compared to just 0.7% in the placebo group. This side effect has not been observed with semaglutide or tirzepatide, making it a potential marker of retatrutide's unique glucagon receptor activity.
The mechanism behind dysesthesia is not fully characterized, but it is thought to relate to the glucagon receptor's role in peripheral nervous system signaling. Most reported cases were mild and did not lead to discontinuation.
For those studying peptide compounds with overlapping metabolic and neurological effects, the metabolic modulation research lines resource offers broader context on how receptor cross-talk can produce unexpected systemic signals.
Additional findings from the clinical literature on Retatrutide Side Effects, Tolerability, and Dose Escalation: What the Clinical Literature Shows include:
- Injection site reactions (mild, consistent with subcutaneous peptide administration)
- Heart rate increases at higher doses, consistent with glucagon receptor activity
- No new cardiovascular safety signals identified in Phase 2 or Phase 3 data to date
Researchers exploring synergistic incretin mechanisms may also find the cagrilintide synergy with GLP-1 article relevant, as it addresses how combination receptor strategies influence tolerability profiles.
Conclusion
The clinical picture of Retatrutide Side Effects, Tolerability, and Dose Escalation: What the Clinical Literature Shows is one of manageable but meaningful adverse events, primarily GI in nature and clearly dose-dependent. Dysesthesia remains the most pharmacologically interesting finding, given its absence in comparable drug classes.
Actionable next steps for researchers and clinicians:
- Prioritize slow dose escalation protocols to reduce peak GI burden.
- Monitor for dysesthesia specifically, as it may be under-recognized without active questioning.
- Assess individual GI tolerance at each dose step before advancing.
- Review the full product research catalog for related metabolic peptide compounds with established tolerability data.
- Cross-reference the metabolic modulation research lines for mechanistic context when interpreting adverse event patterns.
The efficacy data for retatrutide is compelling. But sound research and clinical decision-making begins with a clear-eyed view of the safety profile, not the weight-loss headline.










Leave a Reply
Want to join the discussion?Feel free to contribute!