GLP2 Tirz Peptide: What It Is, Why the Name Exists, and How Researchers Should Interpret It
A single misread label in a research catalog can send an entire study in the wrong direction. That is precisely the risk buried inside the term "GLP2 Tirz Peptide", a shorthand that looks like it refers to the biological hormone GLP-2 but actually points to something else entirely. Understanding the GLP2 Tirz Peptide: What It Is, Why the Name Exists, and How Researchers Should Interpret It is not a minor vocabulary exercise. It is a foundational step in accurate research design.
Key Takeaways
- "GLP2 Tirz" is an informal catalog label for tirzepatide, not a reference to the biological peptide GLP-2.
- Tirzepatide is a dual agonist targeting the GLP-1 and GIP receptors, it does not act on the GLP-2 receptor.
- The "2" in GLP2 Tirz likely reflects a vendor numbering system for dual-receptor compounds, not receptor identity.
- Confusing GLP-2 with tirzepatide can lead to flawed study design and incorrect interpretation of results.
- Research-grade tirzepatide requires strict storage at -20°C and is intended for laboratory use only.
What the Term "GLP2 Tirz Peptide" Actually Means
The phrase "GLP2 Tirz Peptide" does not describe a peptide that binds to the glucagon-like peptide-2 receptor. Instead, it is an informal naming convention used by some research suppliers to catalog tirzepatide, a synthetic dual incretin mimetic.
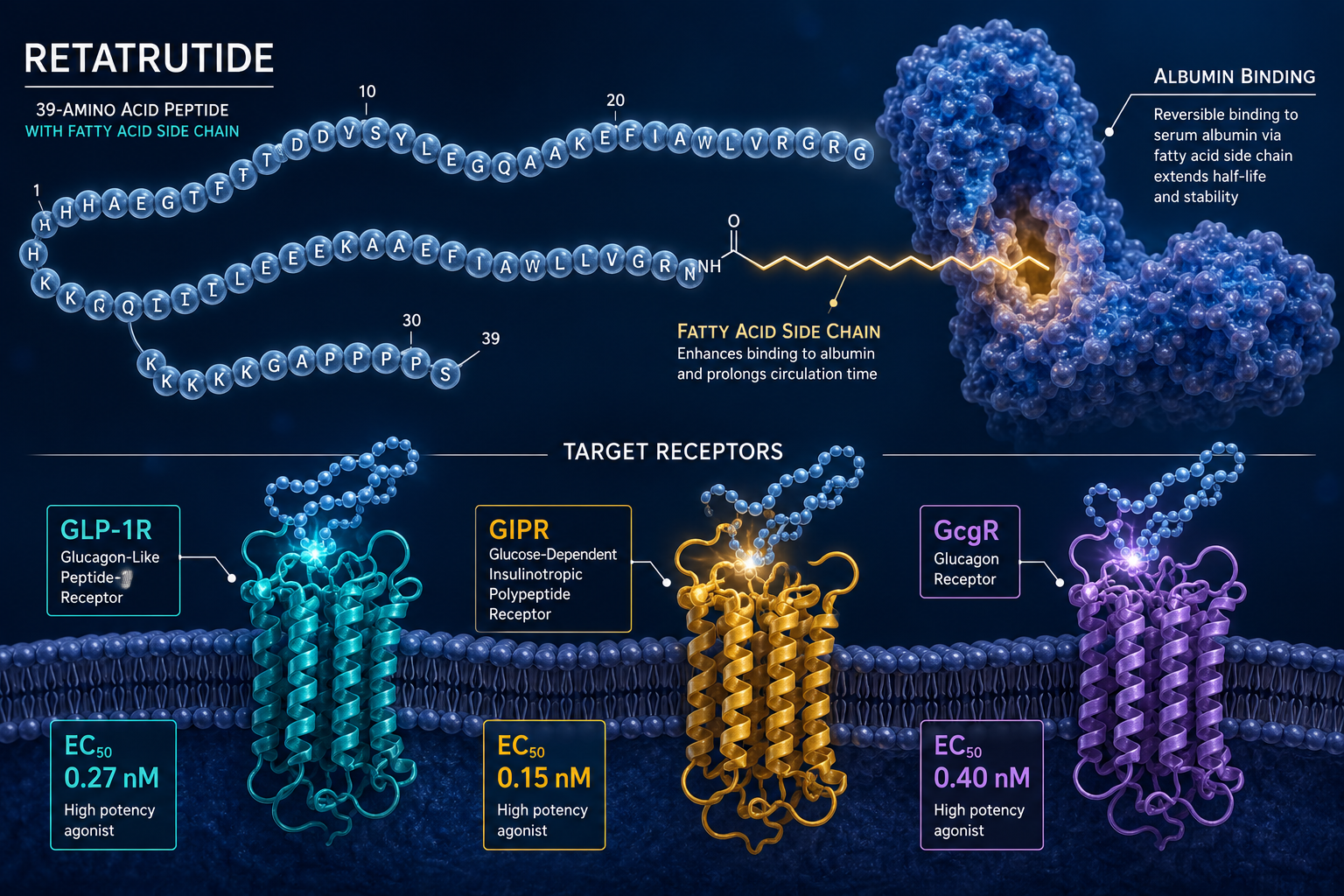
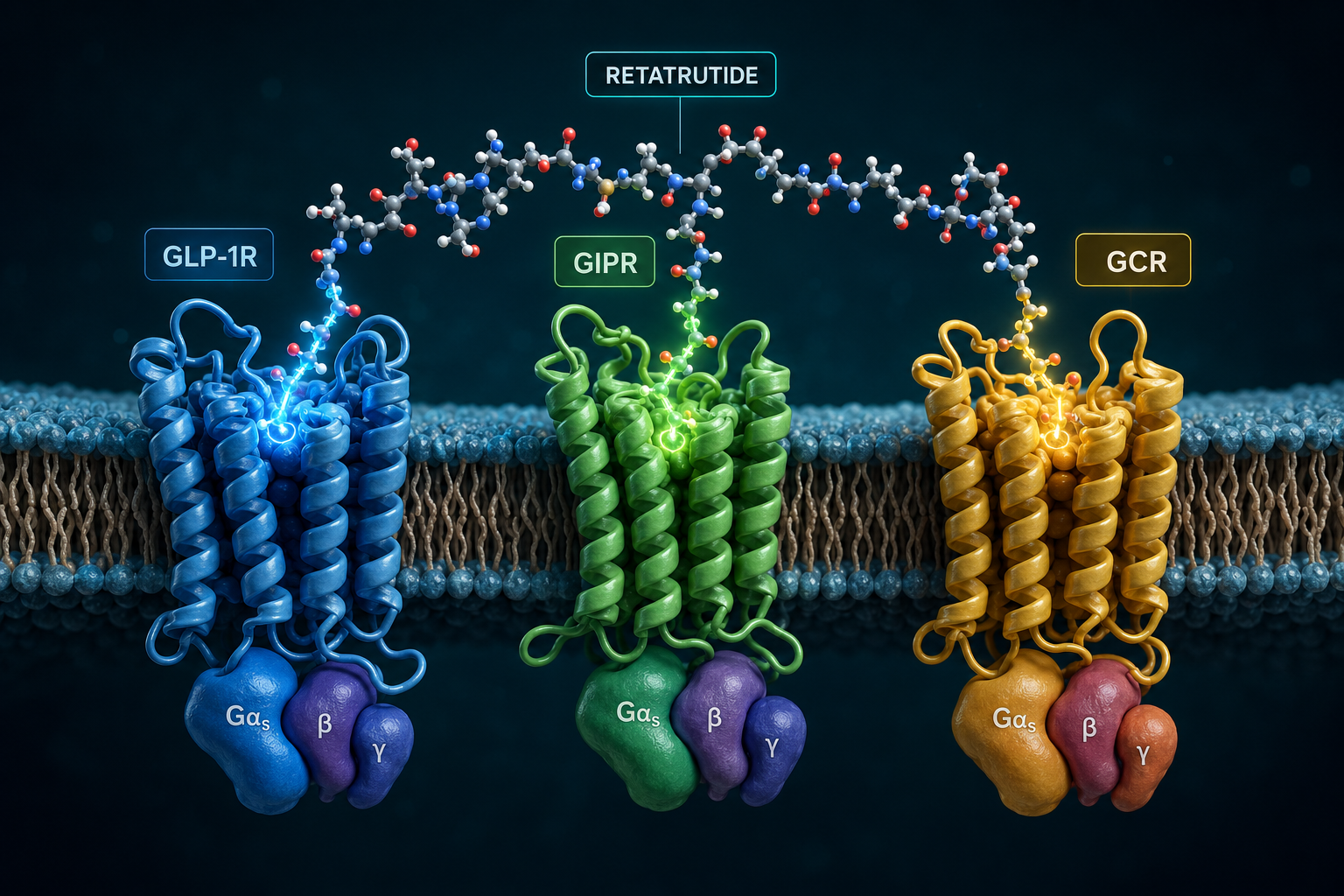
Tirzepatide is the compound's World Health Organization-assigned generic name. The "tirz-" stem signals its dual incretin activity. It was developed as a once-weekly injectable agent and works by co-activating two distinct receptors:
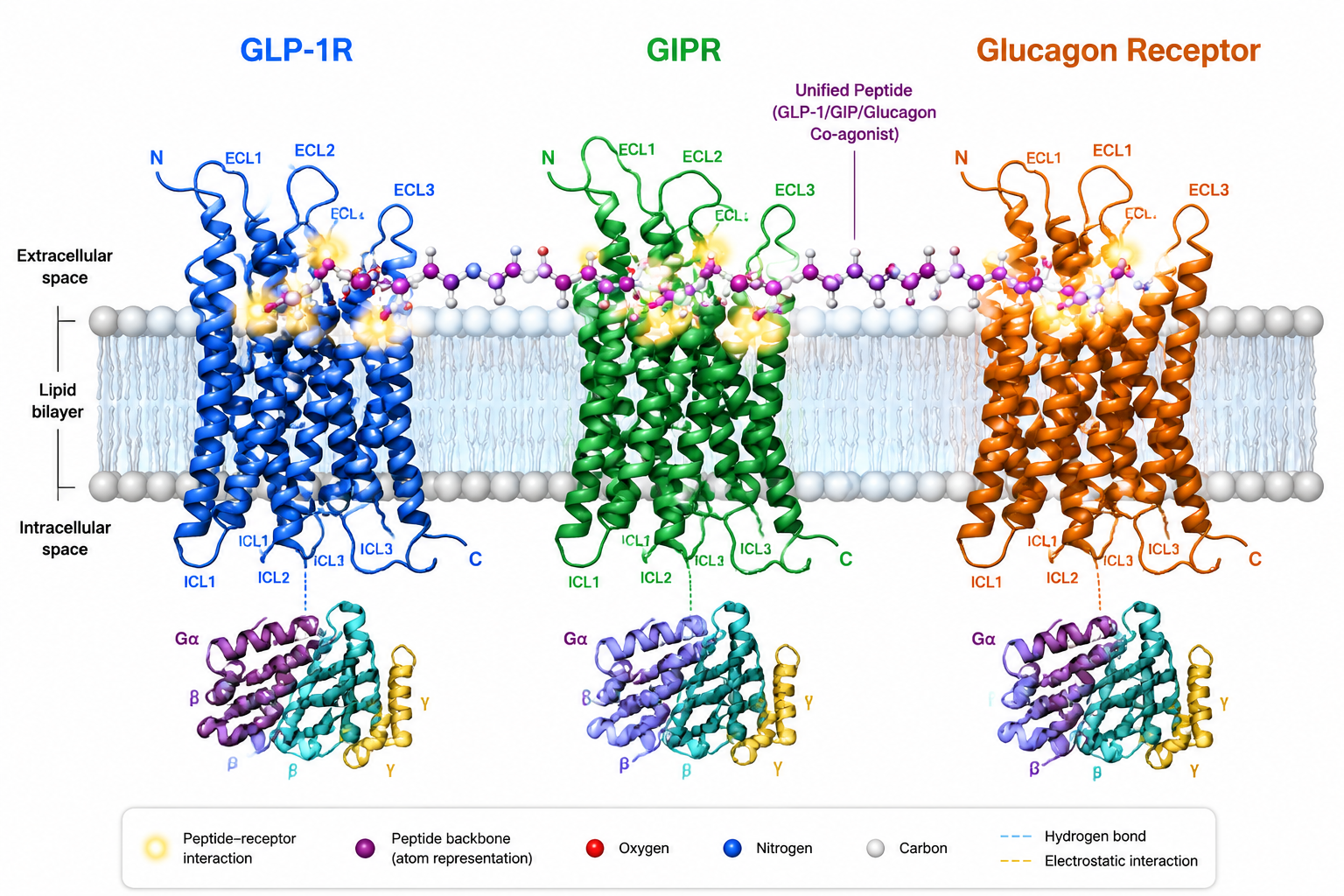
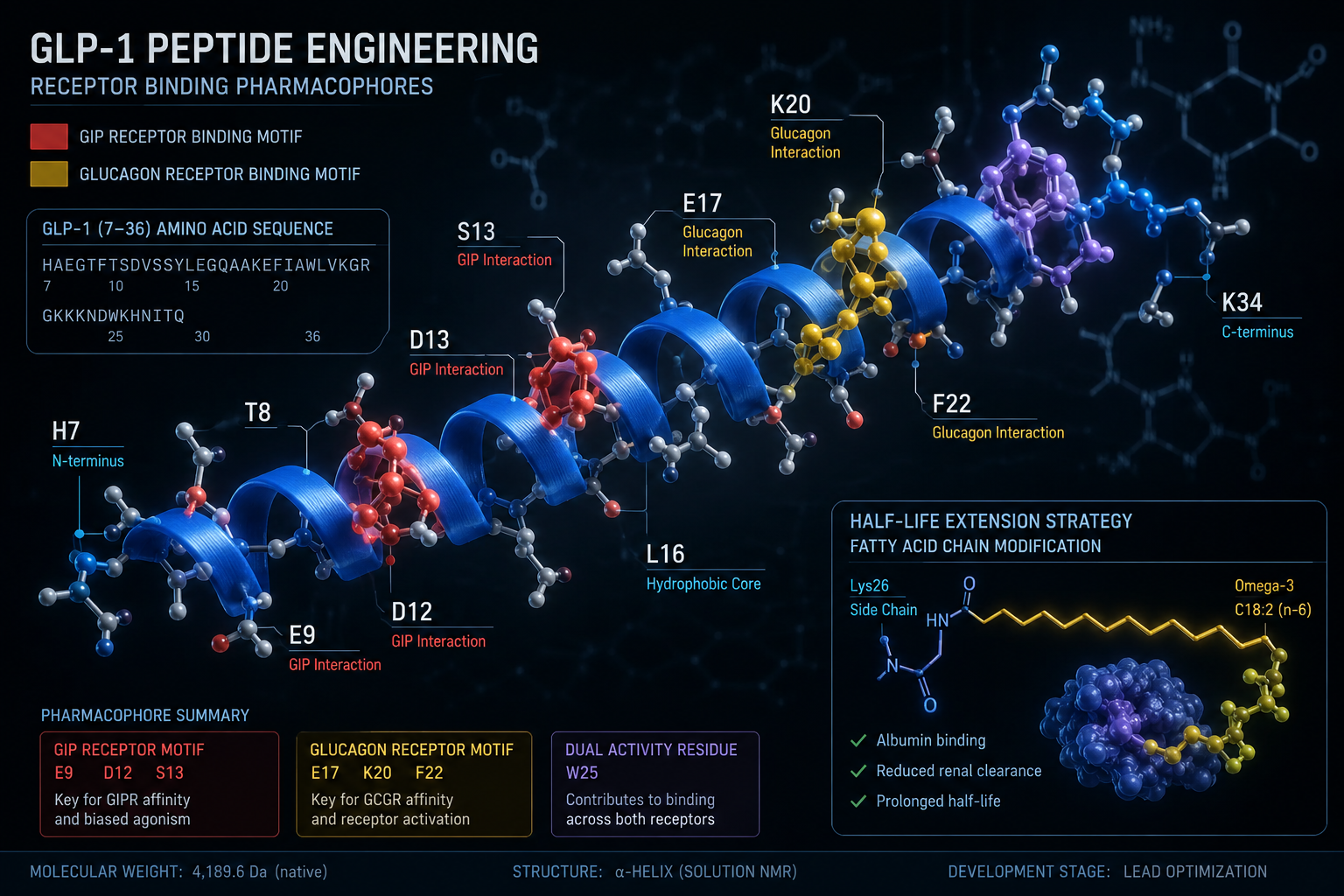
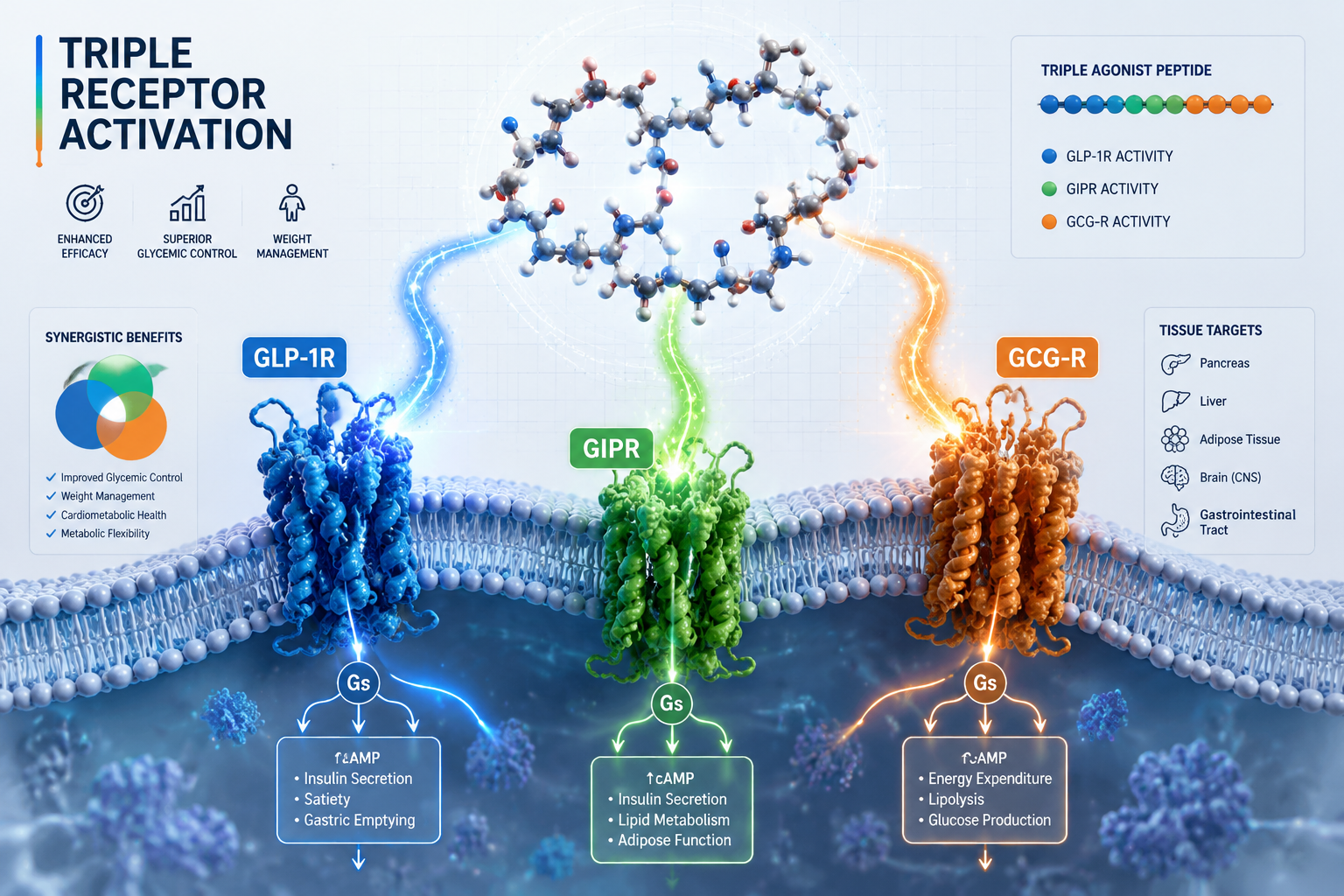
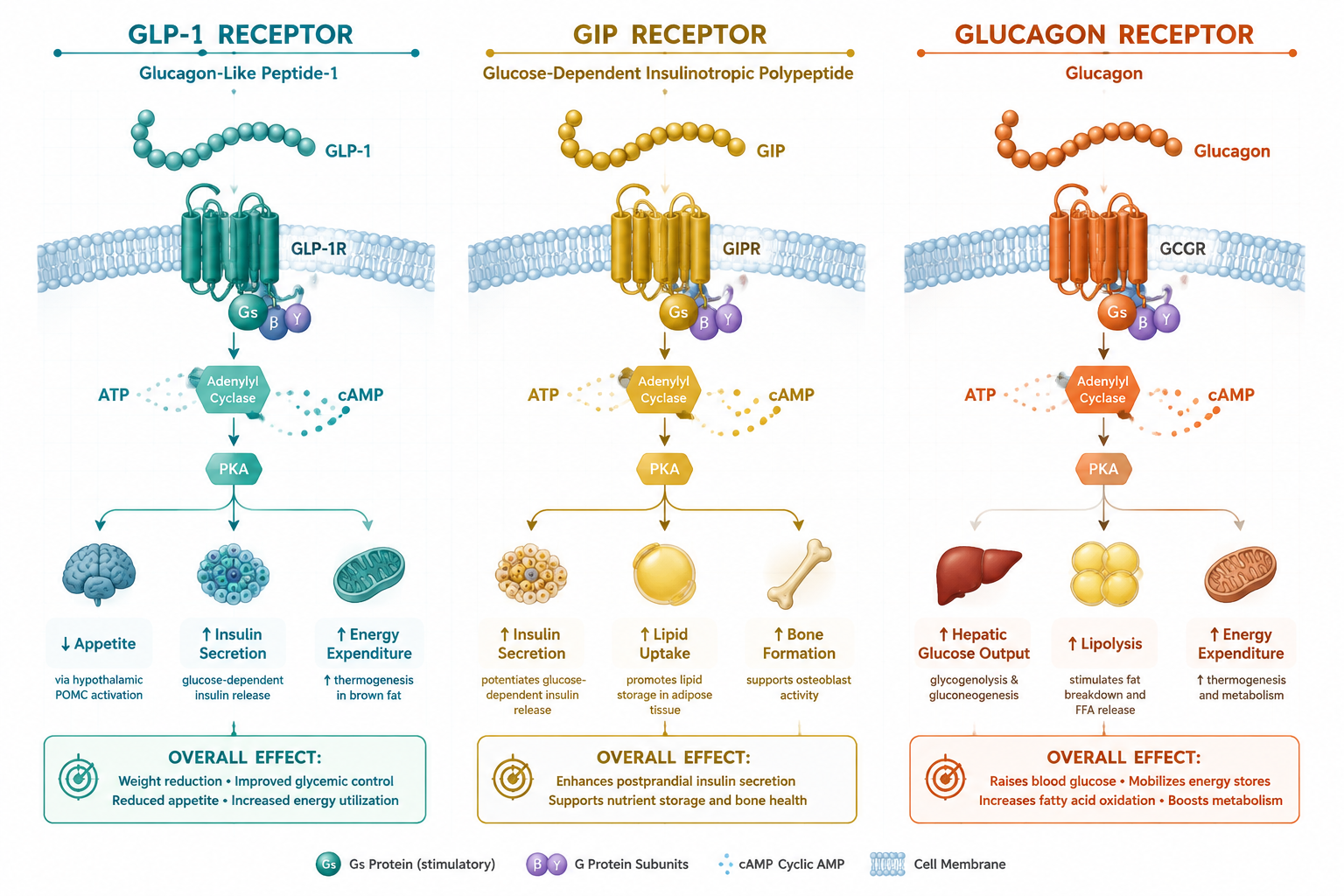
- The GLP-1 receptor (glucagon-like peptide-1), which regulates insulin secretion, appetite suppression, and gastric emptying.
- The GIP receptor (glucose-dependent insulinotropic polypeptide), which influences fat storage, insulin sensitivity, and energy balance.
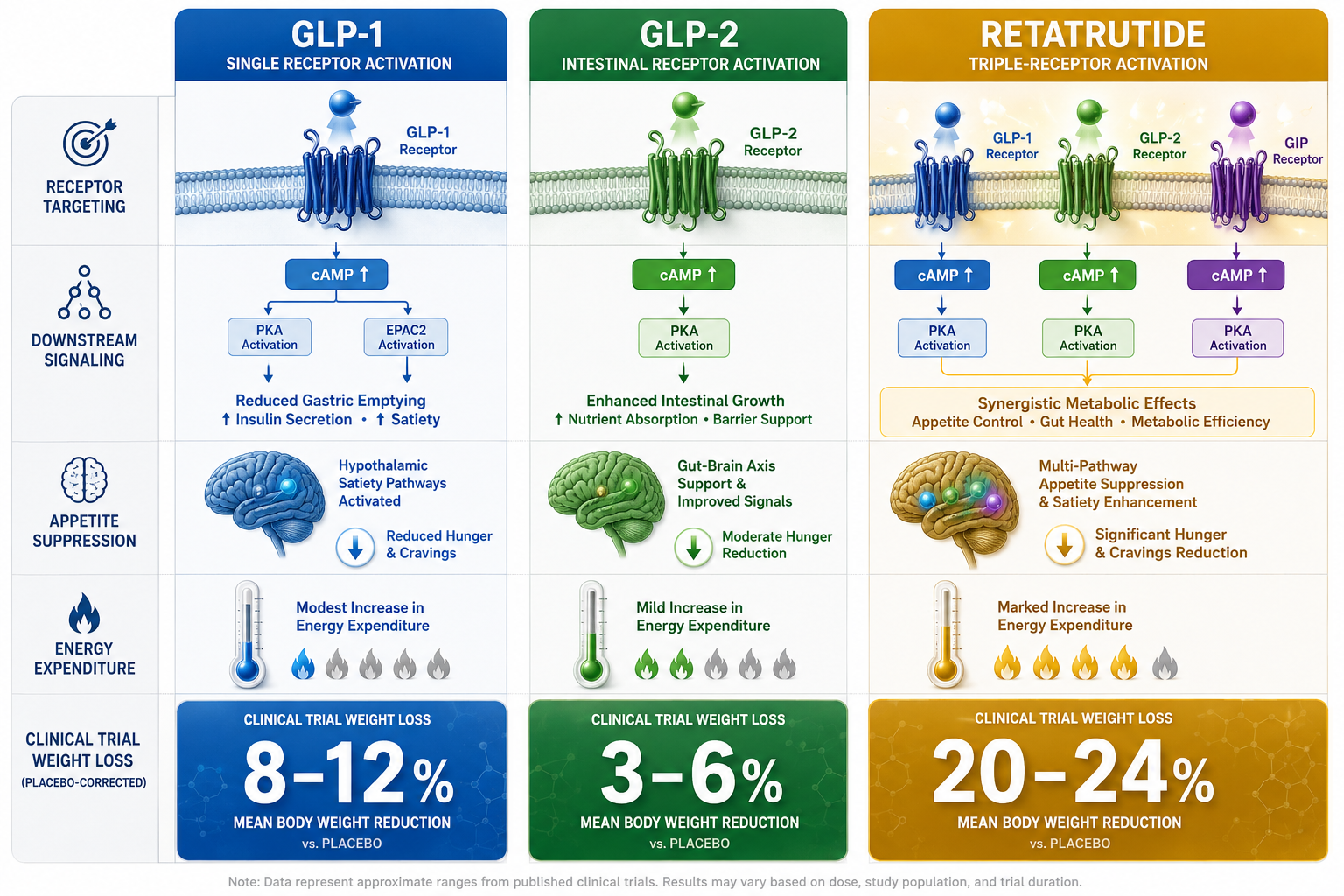
Neither of these is the GLP-2 receptor. GLP-2 is a separate peptide with a distinct biological role, it primarily supports intestinal epithelial growth and gut barrier integrity. Tirzepatide has no known affinity for the GLP-2 receptor.
"The number '2' in GLP2 Tirz does not identify a receptor subtype. It appears to reflect a vendor-assigned sequence number for dual-receptor compounds within a product catalog."
For researchers already familiar with the broader incretin landscape, the GLP-1 T research breakdown on dual receptor agonism provides useful context on how single versus dual agonism differs at the receptor level.
Why the Name Exists: Catalog Logic vs. Scientific Nomenclature
Understanding the GLP2 Tirz Peptide: What It Is, Why the Name Exists, and How Researchers Should Interpret It requires a look at how research suppliers build their catalogs.
Vendors often assign internal shorthand codes to compounds, especially those that share receptor families or structural similarities. In this case, the "GLP" prefix was applied to tirzepatide because it belongs to the incretin mimetic class. The number "2" was likely appended to distinguish it from a single-agonist GLP-1 compound (sometimes listed as "GLP1") in the same catalog.
This creates a numbering logic that reads:
| Catalog Label | Actual Compound | Receptors Targeted |
|---|---|---|
| GLP1 Tirz | Semaglutide-type single agonist | GLP-1 only |
| GLP2 Tirz | Tirzepatide | GLP-1 + GIP |
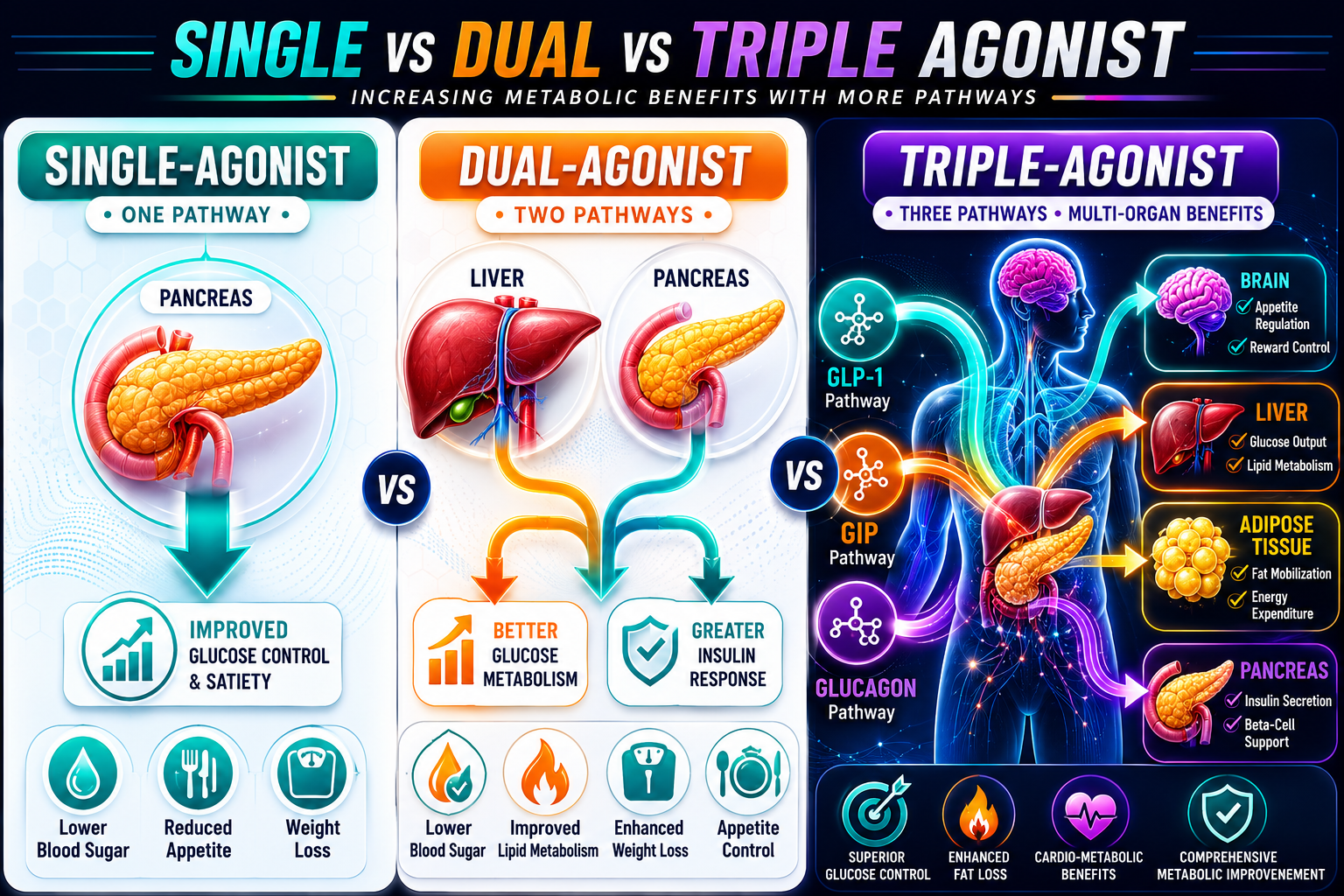
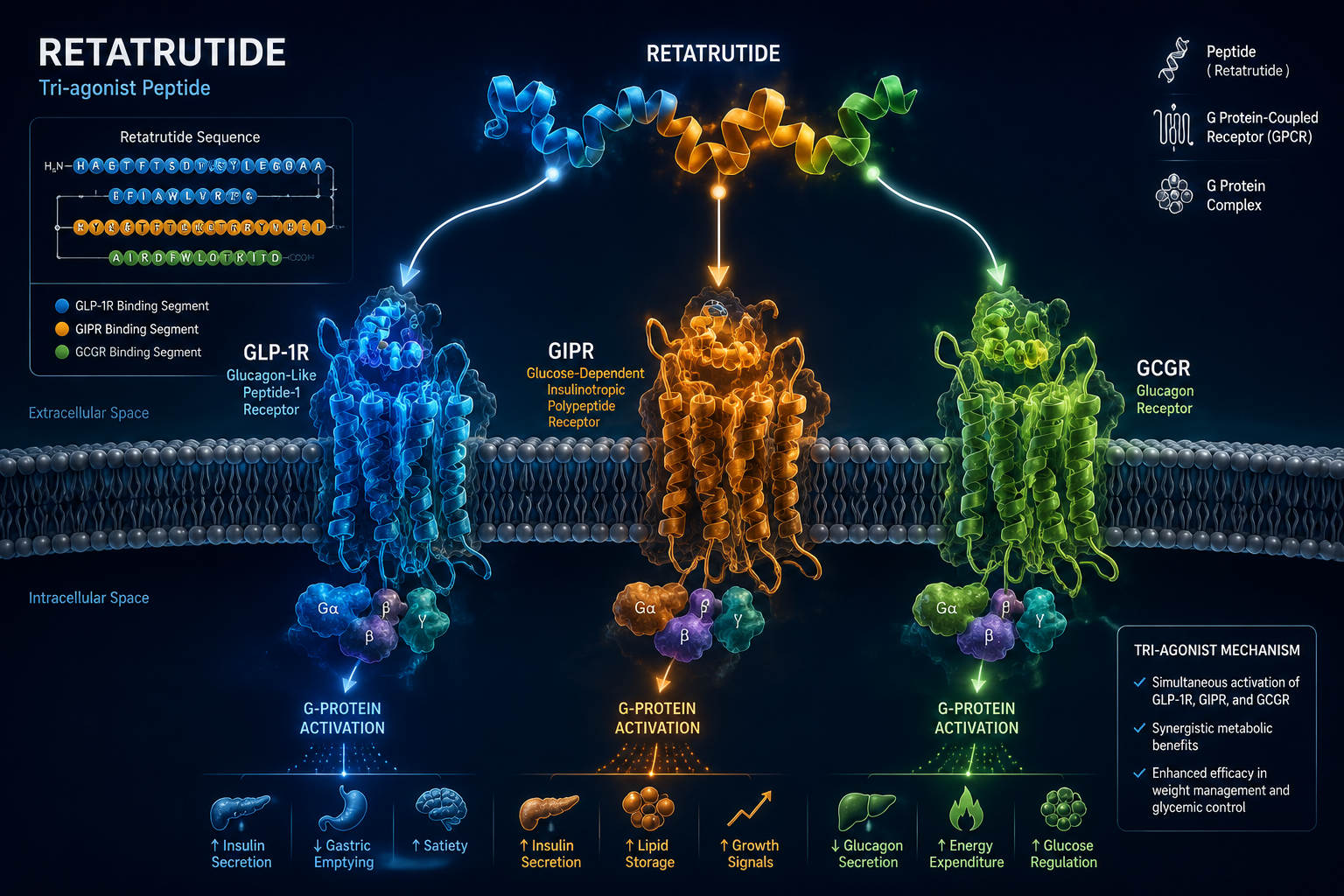
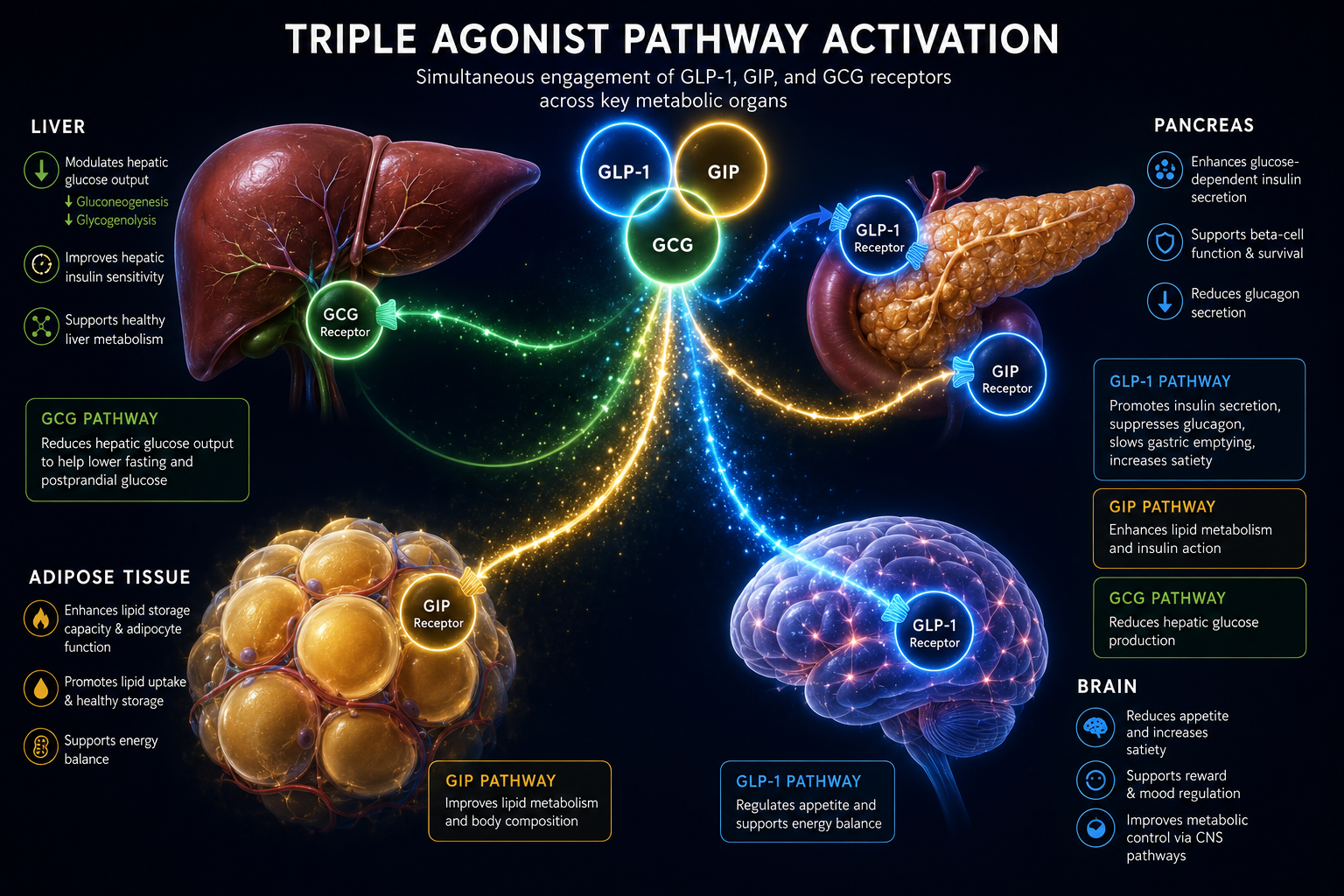
| GLP3 | Triple agonist compounds | GLP-1 + GIP + Glucagon |
The "2" in GLP2 Tirz counts the number of receptor targets, not the receptor name. This distinction is critical. Researchers who encounter this label without that context may incorrectly assume the compound interacts with the GLP-2 receptor, a completely different biological pathway.
For those exploring the next step in this progression, the GLP3 triple agonist overview explains how triple-receptor compounds extend this catalog logic further.
How Researchers Should Interpret GLP2 Tirz Peptide
Accurate interpretation of GLP2 Tirz Peptide: What It Is, Why the Name Exists, and How Researchers Should Interpret It comes down to three practical steps.
Step 1: Verify the Compound Identity
Always cross-reference the catalog label against the molecular formula and Certificate of Analysis (CoA). Research-grade tirzepatide carries the molecular formula C225H348N48O68 and a molecular weight of approximately 4,813.5 g/mol. If those figures match, the compound is tirzepatide regardless of what the label says.
Reputable suppliers provide HPLC-verified purity of 99% or greater. Reviewing the quality testing protocols for research peptides helps researchers understand what documentation to request before use.
Step 2: Align Study Design with the Correct Receptor Targets
Any study designed around GLP2 Tirz should be structured around GLP-1 and GIP receptor pathways, not GLP-2. Research themes for tirzepatide include:
- Glycemic control, insulin secretion dynamics and glucose-dependent responses
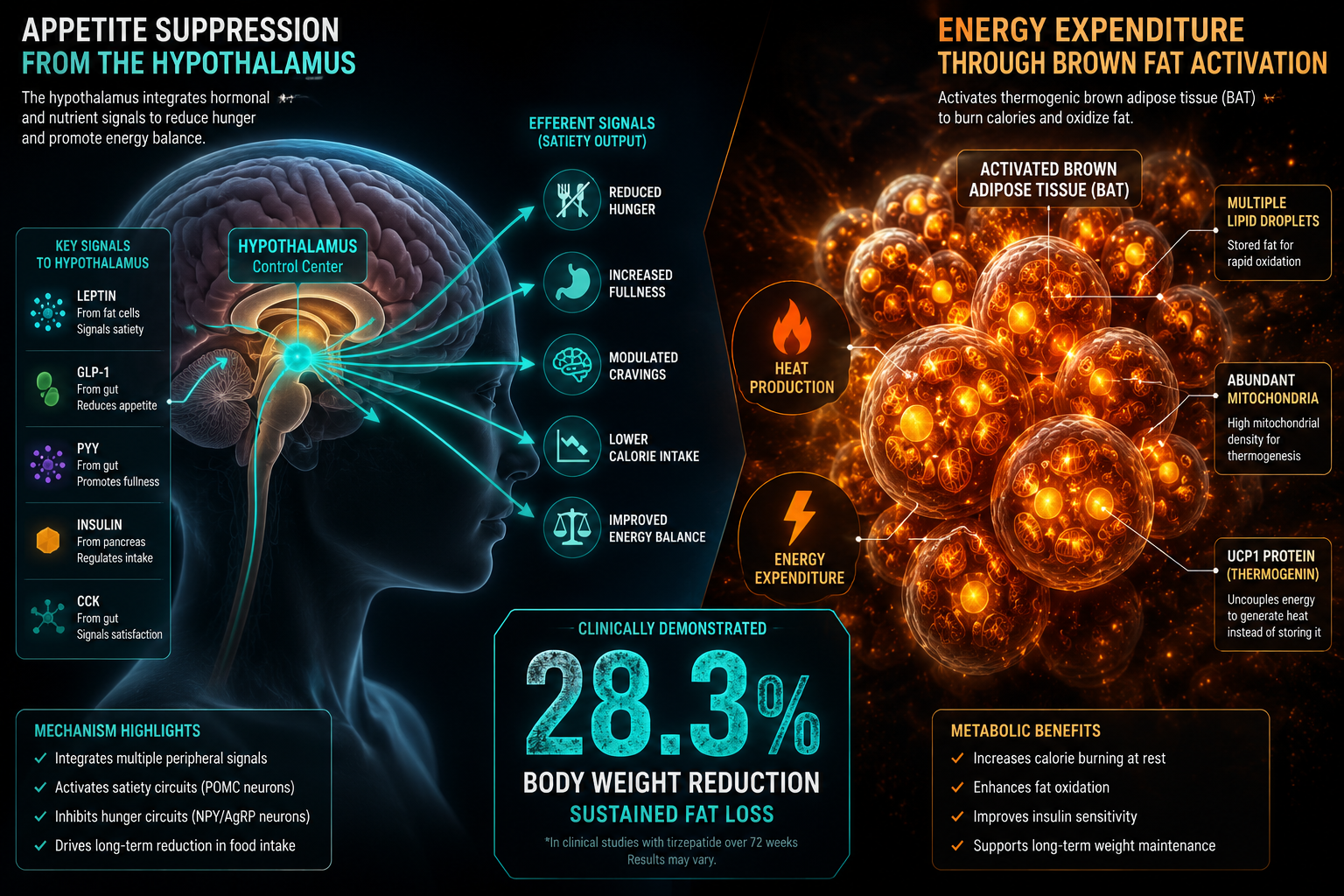
- Weight and fat mass, adipose tissue mobilization and appetite signaling
- Cardiometabolic markers, lipid profiles, blood pressure, and inflammatory indicators
Designing experiments around intestinal epithelial repair or gut barrier function, which are GLP-2 domains, would be a fundamental mismatch.
Related research into metabolic peptide mechanisms can be found in the cagrilintide synergy with GLP-1 overview, which explores how complementary compounds interact within overlapping metabolic pathways.
Step 3: Handle and Store the Compound Correctly
Tirzepatide supplied for research purposes is typically lyophilized, freeze-dried into a powder form. Proper handling requires:
- Storage temperature: -20°C in a sealed, desiccated container
- Light protection: opaque or amber vials to prevent photodegradation
- Reconstitution: sterile bacteriostatic water, used immediately or stored short-term at 4°C
Researchers interested in how other metabolic peptides are handled in similar conditions may find the GIP receptor and its importance article useful for comparative context.
Regulatory and Patent Context for 2026
Tirzepatide's patent protection extends at least through 2036. This has two practical effects on the research market. First, branded pharmaceutical versions remain under exclusive commercial control. Second, it has driven demand for research-grade compounded versions among laboratory researchers who require the compound for preclinical study.
As of 2026, tirzepatide remains classified strictly as a research compound when sourced outside pharmaceutical channels. It is not approved for human or veterinary use in research-grade form. Researchers must document its use within institutional review frameworks and comply with applicable laboratory regulations.
For those exploring how other dual-pathway or metabolic research compounds are positioned in 2026, the NAD+ energetics and longevity research themes article offers a parallel look at how complex compounds are studied within rigorous frameworks.
Conclusion
The label "GLP2 Tirz Peptide" is a vendor shorthand, not a scientific classification. It refers to tirzepatide, a dual GLP-1 and GIP receptor agonist, and the "2" counts receptor targets, not receptor names. Confusing it with the biological peptide GLP-2 is an easy mistake with significant consequences for study design.
Actionable next steps for researchers:
- Always verify compound identity through molecular weight and HPLC documentation before designing any protocol.
- Build experimental frameworks around GLP-1 and GIP receptor biology, not GLP-2 pathways.
- Store lyophilized tirzepatide at -20°C in desiccated, light-protected conditions.
- Stay current with regulatory classifications in your jurisdiction, as the research peptide landscape continues to evolve through 2026 and beyond.
Precision in terminology is not bureaucratic caution, it is the first variable in every reliable experiment.