Polypeptide Peptides in Endocrine and Metabolic Pharmacology: Lessons From Amlodipine, Prednisone, and Metoprolol
Three drugs, amlodipine, prednisone, and metoprolol, have shaped cardiovascular and endocrine medicine for decades. Yet their well-documented off-target effects on glucose metabolism, adrenal function, and mitochondrial signaling now serve as a compelling argument for why polypeptide peptides in endocrine and metabolic pharmacology deserve serious research attention in 2026.
Key Takeaways
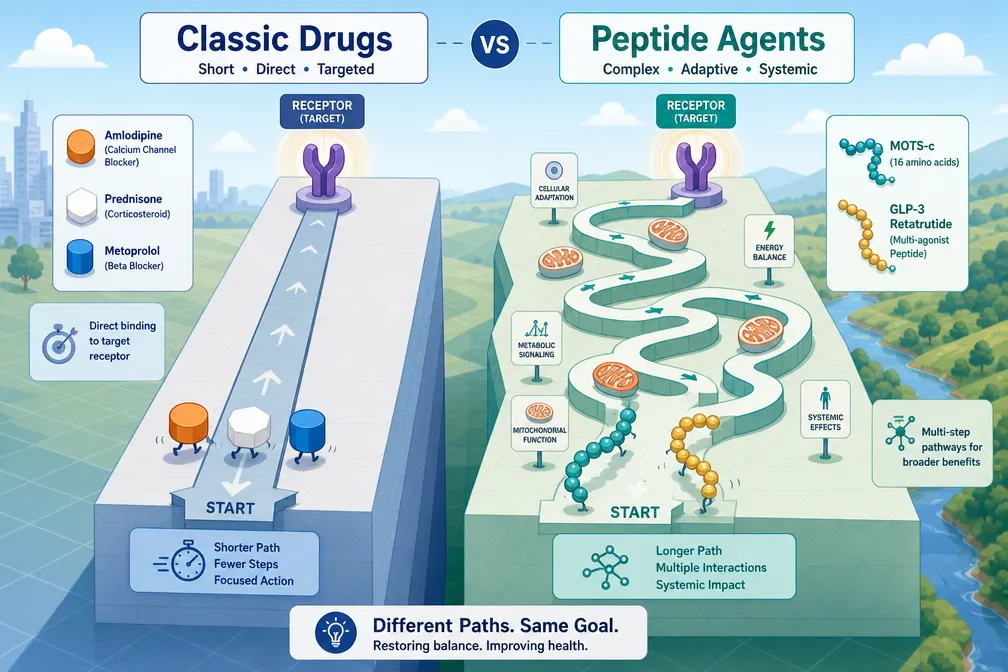
- Amlodipine, prednisone, and metoprolol each interact with endocrine pathways in ways that go beyond their primary targets, producing metabolic side effects that peptide-based agents may avoid.
- Polypeptide peptides in endocrine and metabolic pharmacology offer receptor selectivity, shorter off-target profiles, and tissue-specific action that small molecules often cannot match.
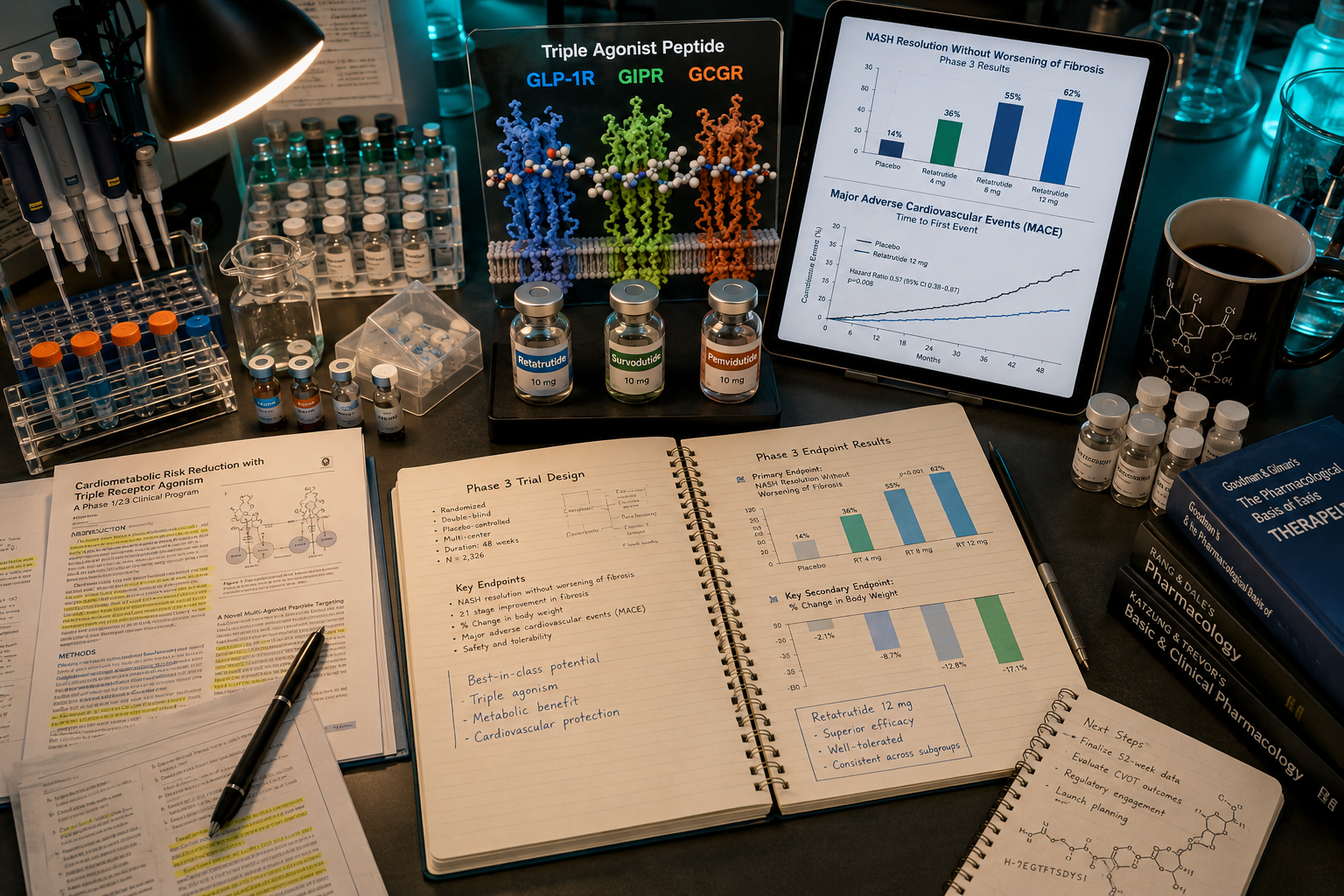
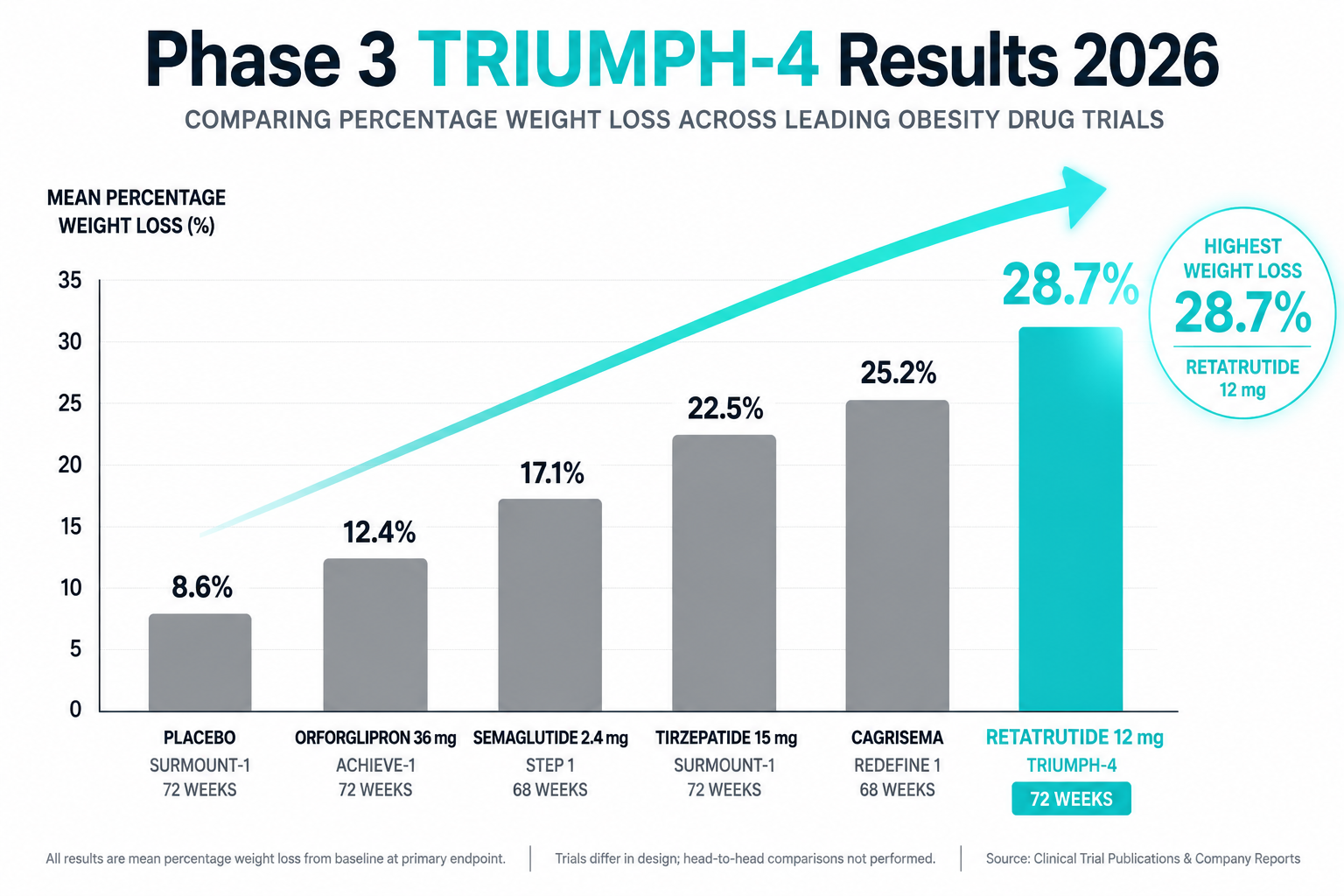
- GLP-1 receptor agonists and multi-agonist peptides represent the most clinically advanced examples of this shift, with GLP-3 retatrutide research extending the frontier.
- Mitochondrial peptides such as MOTS-c address metabolic dysregulation at the cellular energy level, a target unreachable by classic small molecules.
- Understanding the pharmacological gaps left by legacy drugs helps researchers identify where peptide-based tools offer the greatest research value.
How Classic Small Molecules Interact With Endocrine Pathways
Amlodipine blocks L-type calcium channels in vascular smooth muscle, reducing blood pressure and myocardial oxygen demand. However, calcium signaling is also central to pancreatic beta-cell insulin secretion. Disrupting this pathway even modestly can impair glucose-stimulated insulin release, a finding that has been observed in long-term hypertension management research.
Prednisone, a synthetic glucocorticoid, binds glucocorticoid receptors with broad tissue distribution. Its anti-inflammatory power comes at a metabolic cost: stimulation of hepatic gluconeogenesis, suppression of peripheral insulin sensitivity, and disruption of the hypothalamic-pituitary-adrenal axis. These are not rare side effects, they are mechanistic consequences of how the drug binds.
Metoprolol, a beta-1 selective adrenergic blocker, reduces heart rate and cardiac output effectively. Its endocrine liability lies in masking hypoglycemic symptoms and blunting the catecholamine-driven recovery from low blood glucose, a clinically relevant concern in diabetic patients.
The pattern is consistent: each drug achieves its primary goal through a mechanism that inevitably touches endocrine or metabolic circuitry.
"The off-target metabolic effects of classic small molecules are not design flaws, they are the predictable result of targeting signaling pathways that evolution never isolated."
Polypeptide Peptides in Endocrine and Metabolic Pharmacology: The Receptor Targeting Advantage
Where small molecules bind with high affinity but low tissue selectivity, polypeptide peptides in endocrine and metabolic pharmacology operate through receptor systems that are more anatomically restricted. This distinction is not merely theoretical.
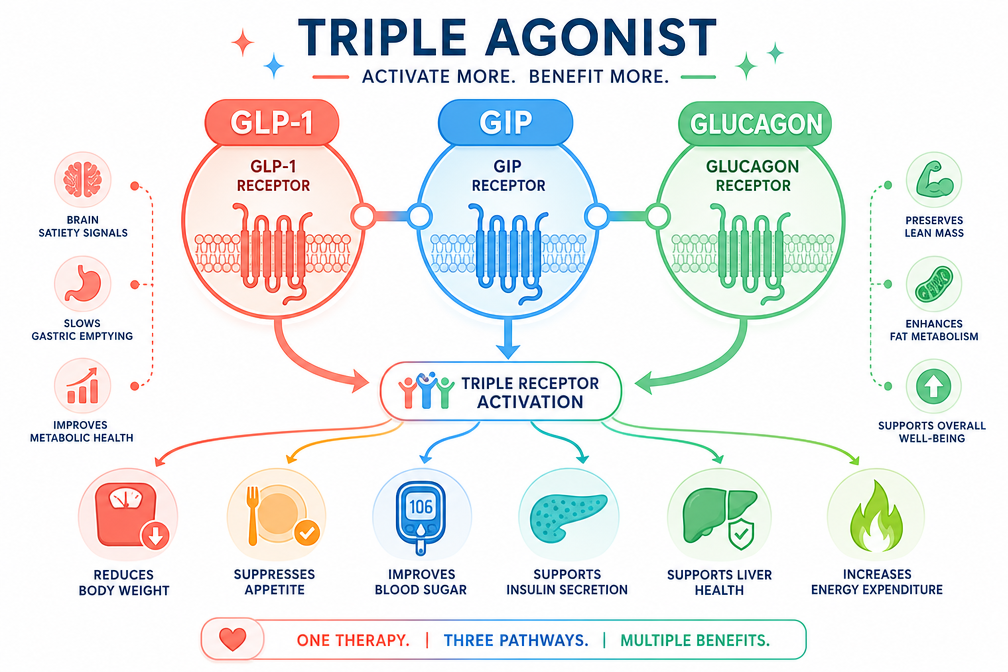
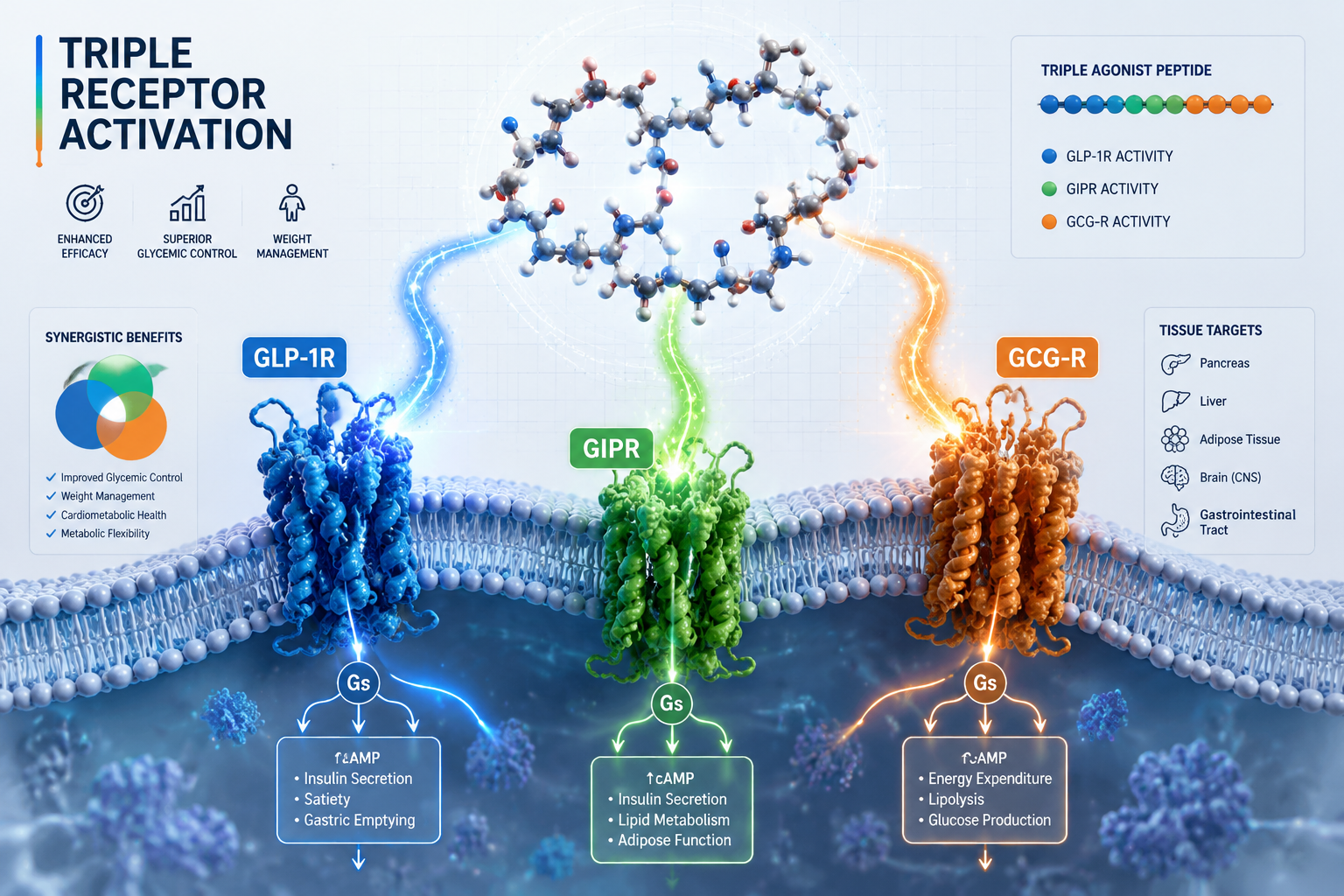
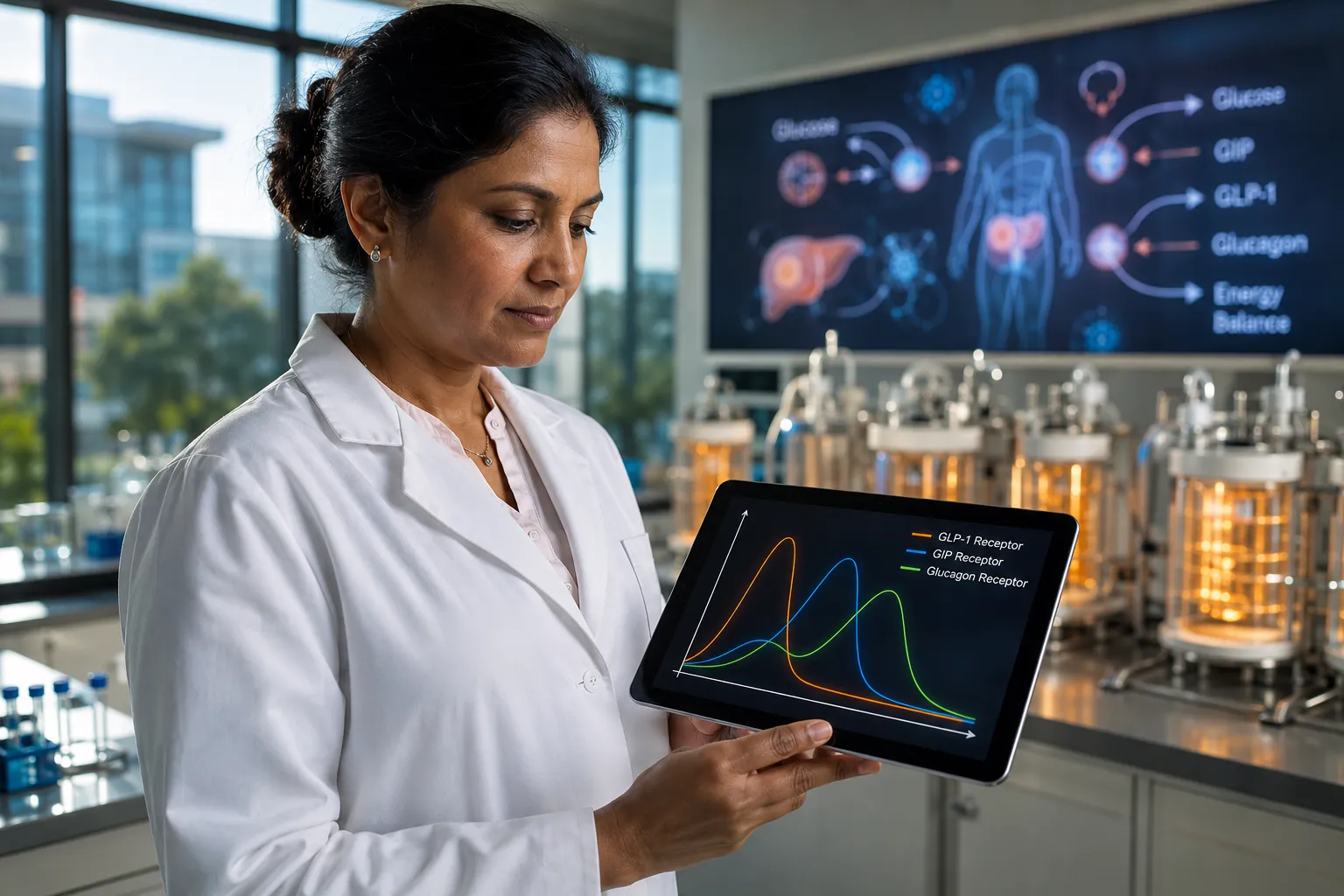
Proglucagon-derived peptides, including GLP-1, GLP-2, glucagon, and oxyntomodulin, each act on distinct receptor populations across the gut, pancreas, brain, and liver. GLP-1 receptor agonists lower blood glucose by enhancing insulin secretion only when glucose is already elevated, a glucose-dependent mechanism that eliminates the hypoglycemia risk associated with metoprolol-class drugs.
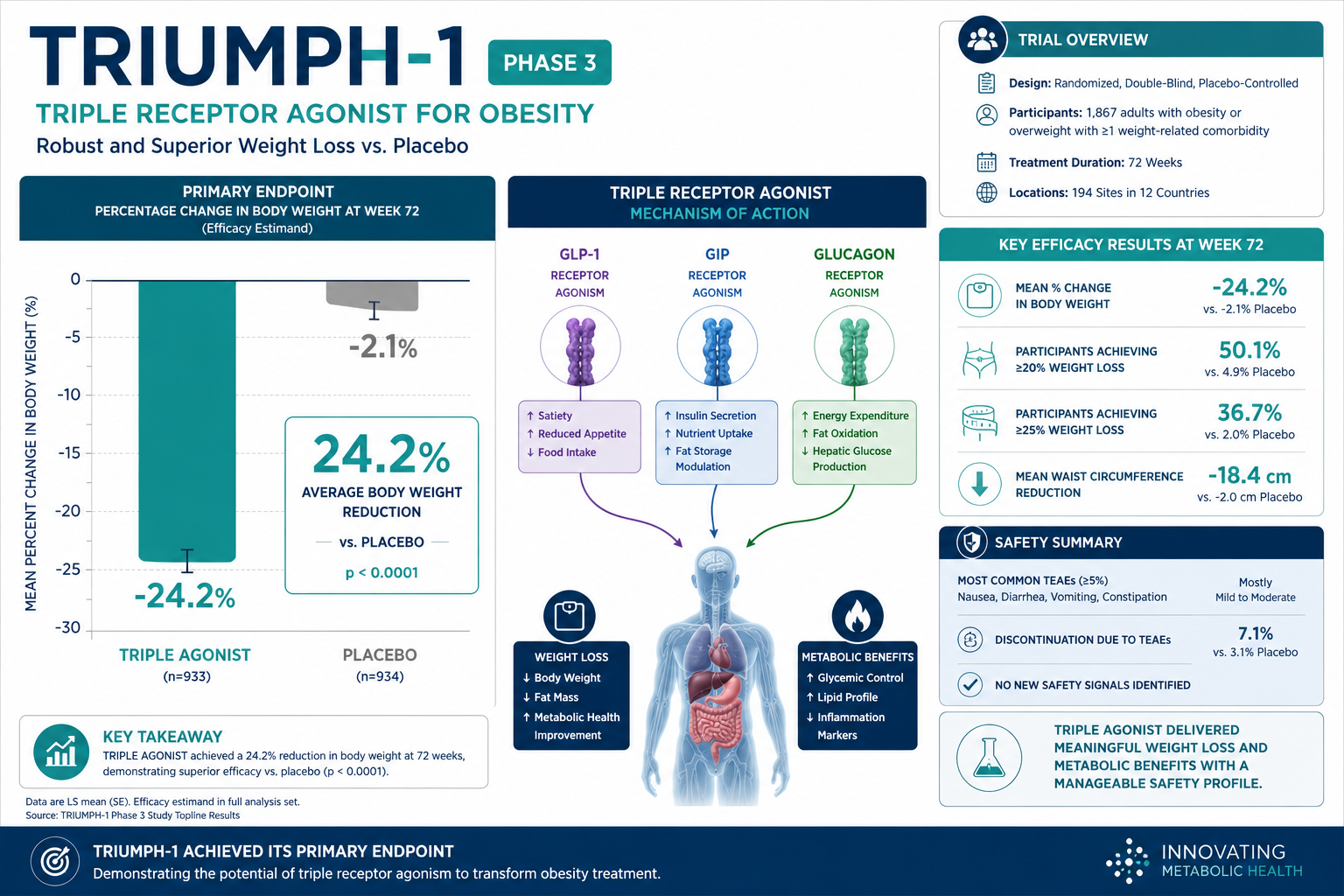
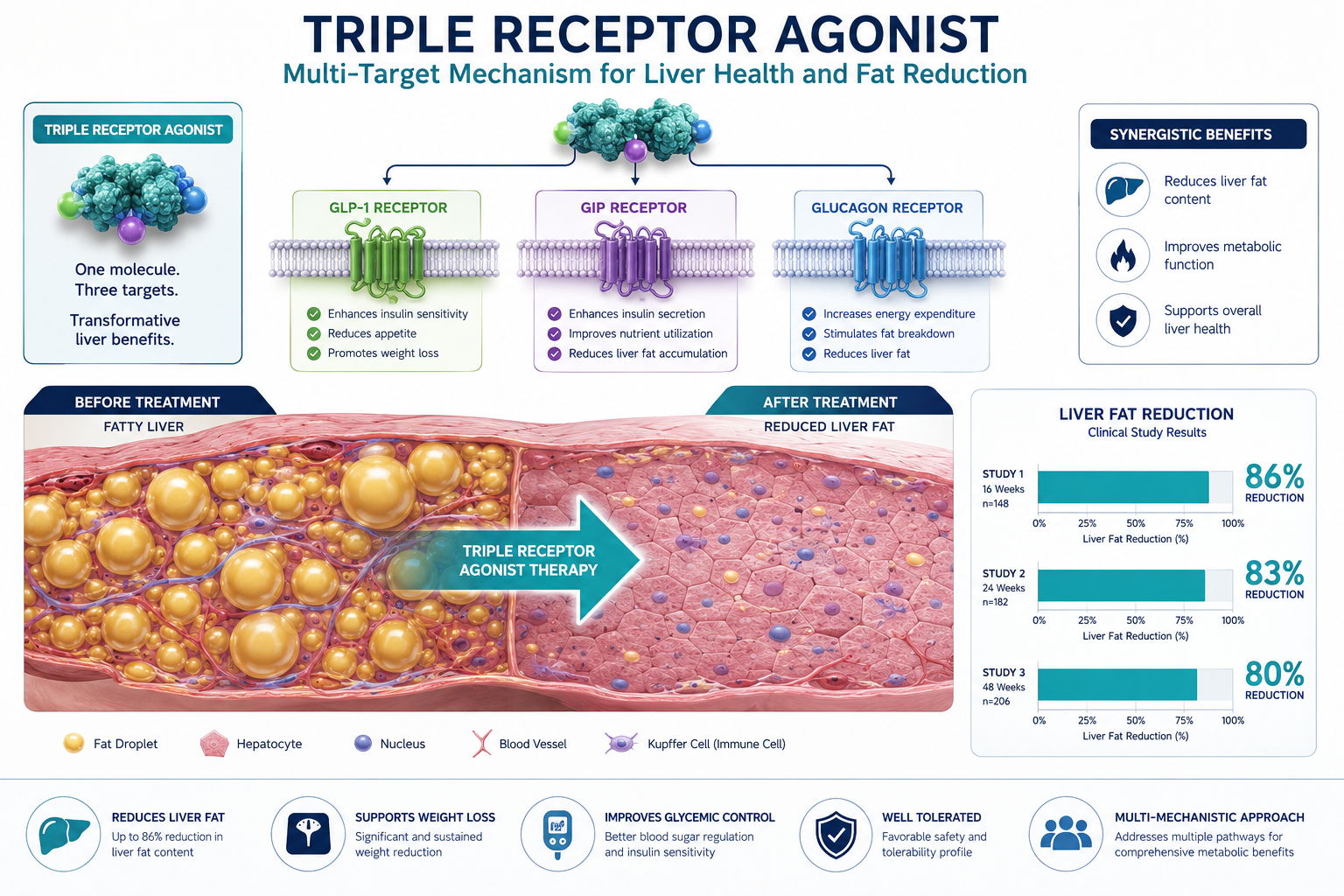
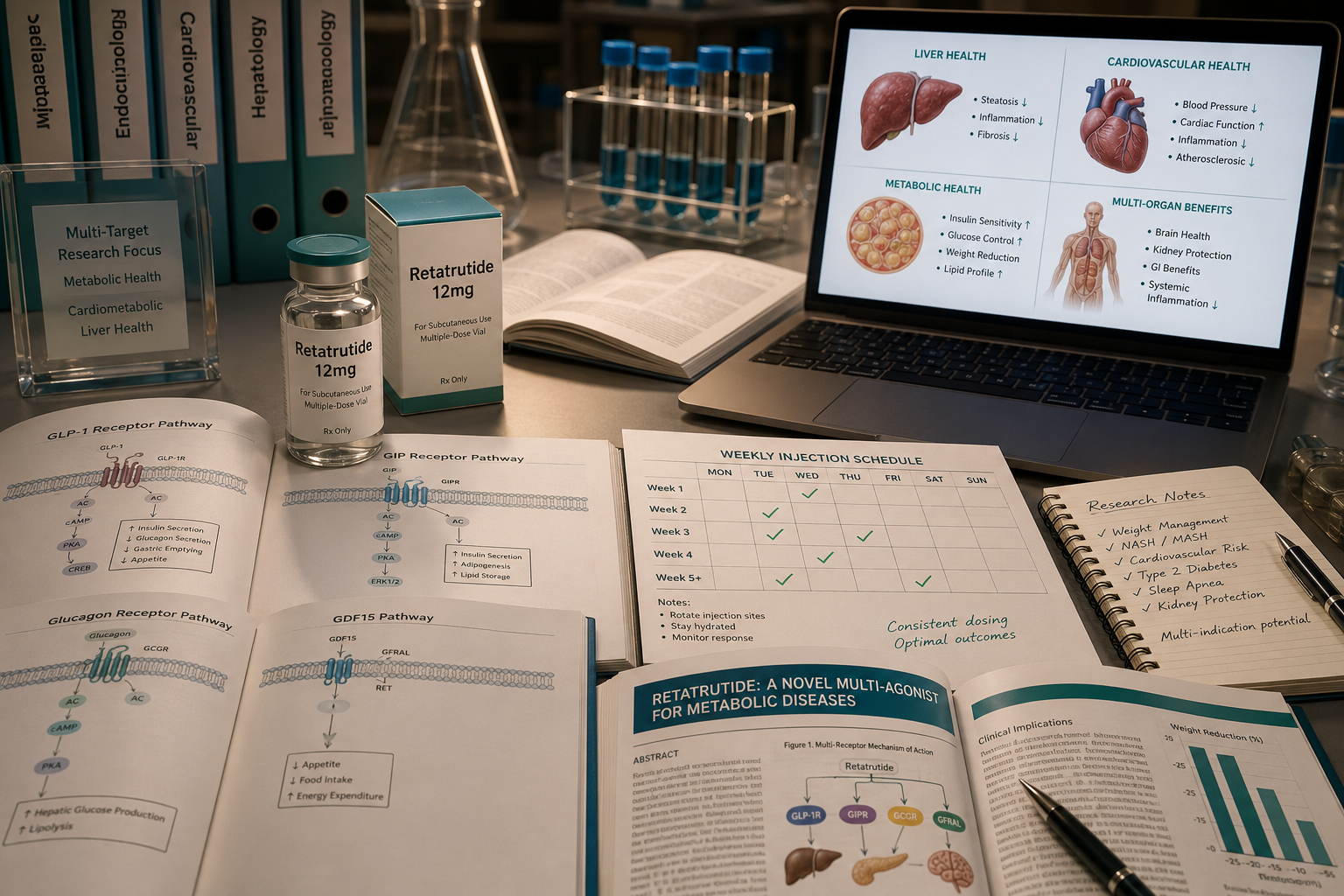
The next generation goes further. Multi-agonist peptides combine amino acid sequences from GLP-1, glucagon, and GIP hormones into single molecules with enhanced potency and extended half-lives. Research into GLP-3 retatrutide represents this frontier, targeting multiple incretin receptors simultaneously to address obesity and type 2 diabetes with a precision that prednisone-driven metabolic disruption cannot approach.
The GIP receptor plays a particularly important role here. GIP works synergistically with GLP-1 to amplify insulin secretion and may also support bone metabolism and fat storage regulation, a multi-system effect achieved without the adrenal suppression that defines glucocorticoid pharmacology.
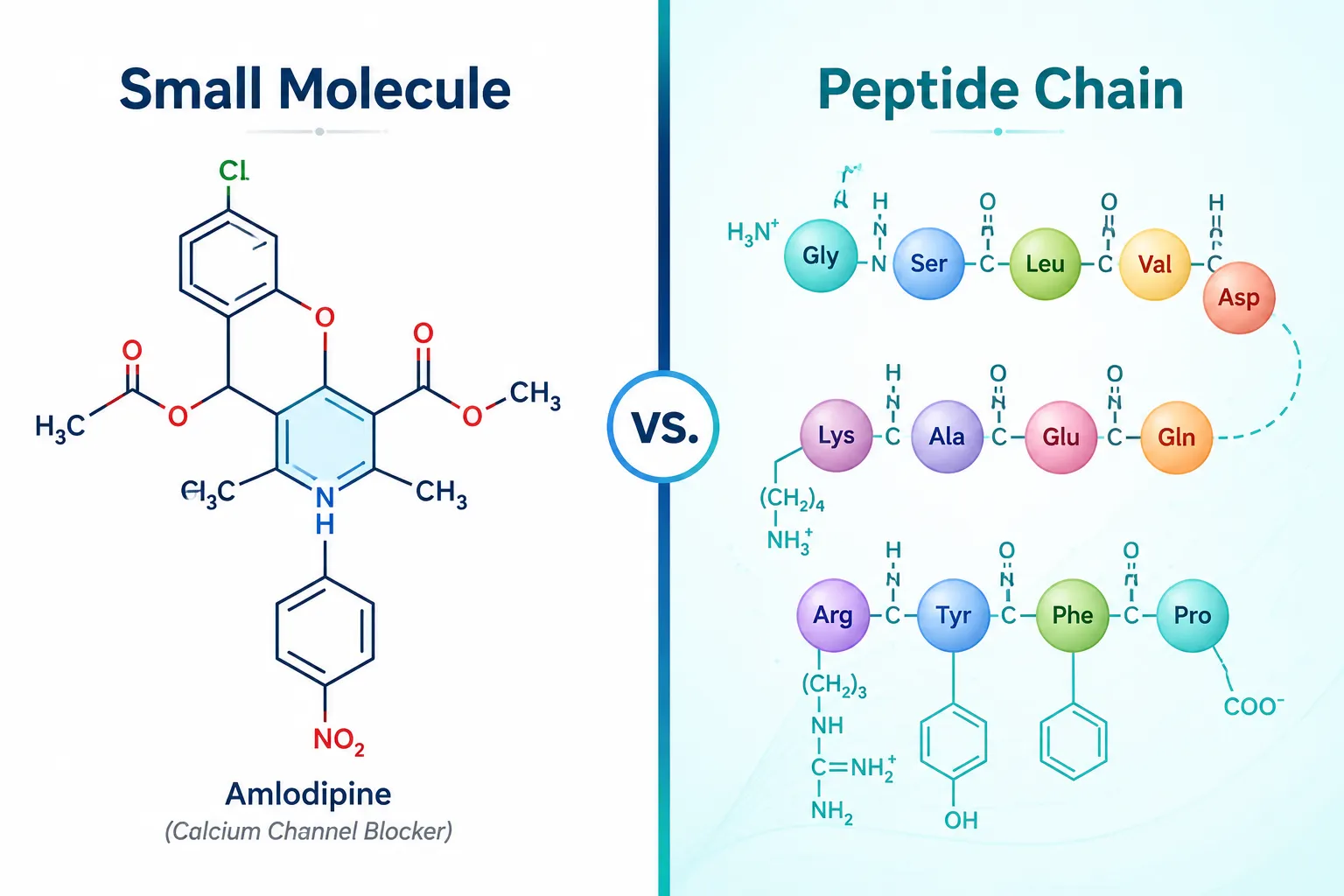
Key differences between small molecules and peptide agents:
| Feature | Small Molecules (e.g., Prednisone) | Peptide Agents (e.g., GLP-1 agonists) |
|---|---|---|
| Receptor selectivity | Broad | Tissue-restricted |
| Metabolic off-target effects | Common | Reduced |
| Half-life engineering | Limited | Highly modifiable |
| Glucose-dependent action | No | Yes (GLP-1 class) |
Adrenomedullin, a 52-amino acid peptide hormone, further illustrates the endocrine complexity peptides can address. It regulates cardiovascular tone and lymphatic function while also inhibiting insulin secretion in a dose-dependent manner, a finding that positions it as both a research target and a cautionary example of peptide pleiotropy.
Mitochondrial Peptides and the Metabolic Gap Left by Legacy Drugs
Neither amlodipine, prednisone, nor metoprolol addresses cellular energy metabolism at the mitochondrial level. This is a significant gap. Chronic glucocorticoid use, in particular, impairs mitochondrial biogenesis and increases reactive oxygen species production, effects that accelerate metabolic aging.
This is precisely where mitochondrial-derived peptides enter the research conversation. MOTS-c, encoded within mitochondrial DNA, regulates glucose uptake, fatty acid oxidation, and insulin sensitivity through AMPK activation. Its mechanism operates entirely outside the receptor systems targeted by classic cardiovascular drugs, making it a complementary rather than competing research tool.
SS-31 peptide research addresses a related problem: mitochondrial membrane integrity under oxidative stress. Where prednisone-induced metabolic disruption increases oxidative burden, SS-31 targets cardiolipin on the inner mitochondrial membrane to preserve electron transport chain function.
For researchers exploring body composition and visceral adiposity, conditions worsened by long-term glucocorticoid exposure, tesa offers a growth hormone-releasing hormone analog that specifically reduces visceral fat without the broad hormonal disruption of steroid-class drugs.
Non-incretin peptide systems are also gaining traction. Apelin, spexin, and meteorin-like protein (METRNL) each interact with energy balance pathways that small molecules have historically ignored, opening new drug discovery targets for metabolic disease research.
For those examining AOD-9604 metabolic research, the lipolytic fragment of growth hormone provides another example of how peptide engineering can isolate a single metabolic function, fat mobilization, without replicating the full hormonal cascade of its parent molecule.
Conclusion
The lessons from amlodipine, prednisone, and metoprolol are not arguments against small-molecule pharmacology. They are a precise map of where that pharmacology ends and where polypeptide peptides in endocrine and metabolic pharmacology begin. Each classic drug reveals a metabolic vulnerability, impaired insulin secretion, adrenal suppression, blunted glycemic recovery, that modern peptide research is systematically designed to address.
Actionable next steps for researchers and clinicians:
- Review the receptor selectivity profiles of any metabolic intervention against the endocrine off-target effects documented in glucocorticoid and beta-blocker literature.
- Explore mitochondrial peptide tools such as MOTS-c and SS-31 for research models involving oxidative stress or insulin resistance secondary to classic drug exposure.
- Track multi-agonist peptide development, particularly GLP-1/GIP/glucagon tri-agonists, as the most clinically proximate evolution of endocrine peptide pharmacology.
- Use the pharmacological gaps in legacy drugs as a framework for identifying where peptide-based research tools add the most mechanistic value.
The field is not replacing its foundations. It is building precisely where those foundations show their limits.