The Science Behind Glow Blend Peptide: Collagen, Antioxidants, and Skin Research Applications
Collagen loss accelerates at roughly 1% per year after age 25, a biochemical reality that has driven intense research into peptide-based interventions. The science behind Glow Blend Peptide: collagen, antioxidants, and skin research applications sits at the intersection of molecular biology and dermal tissue research, combining several well-studied bioactive compounds into a single formulation designed for investigative use. Understanding how each component works, and why the combination matters, reveals a compelling scientific rationale.

Key Takeaways
- Glow Blend is a research-grade peptide formulation containing GHK-Cu, BPC-157, TB-500, and related compounds in a combined 70 mg vial.
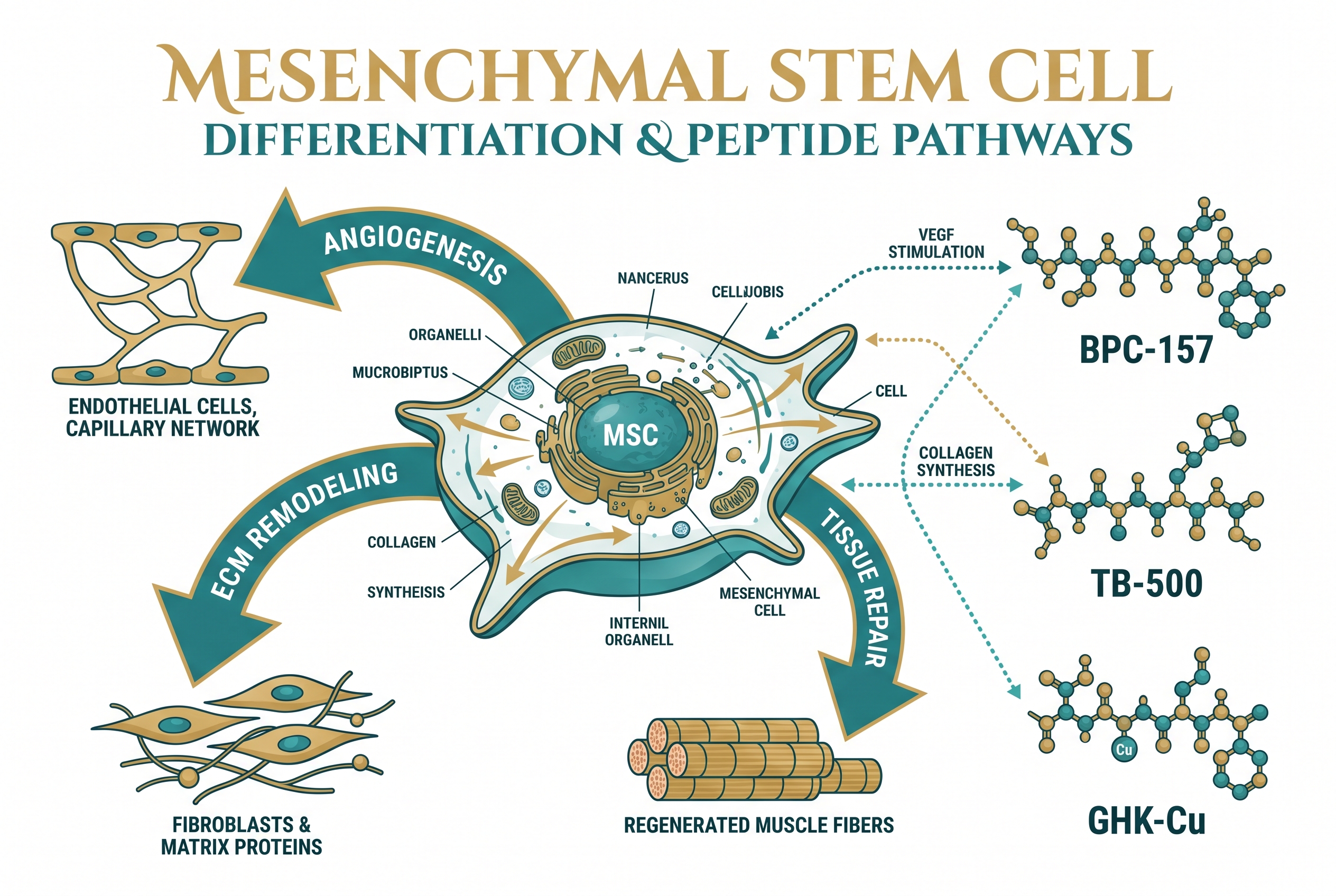
- GHK-Cu is the primary collagen-stimulating agent, activating fibroblast activity and extracellular matrix remodeling.
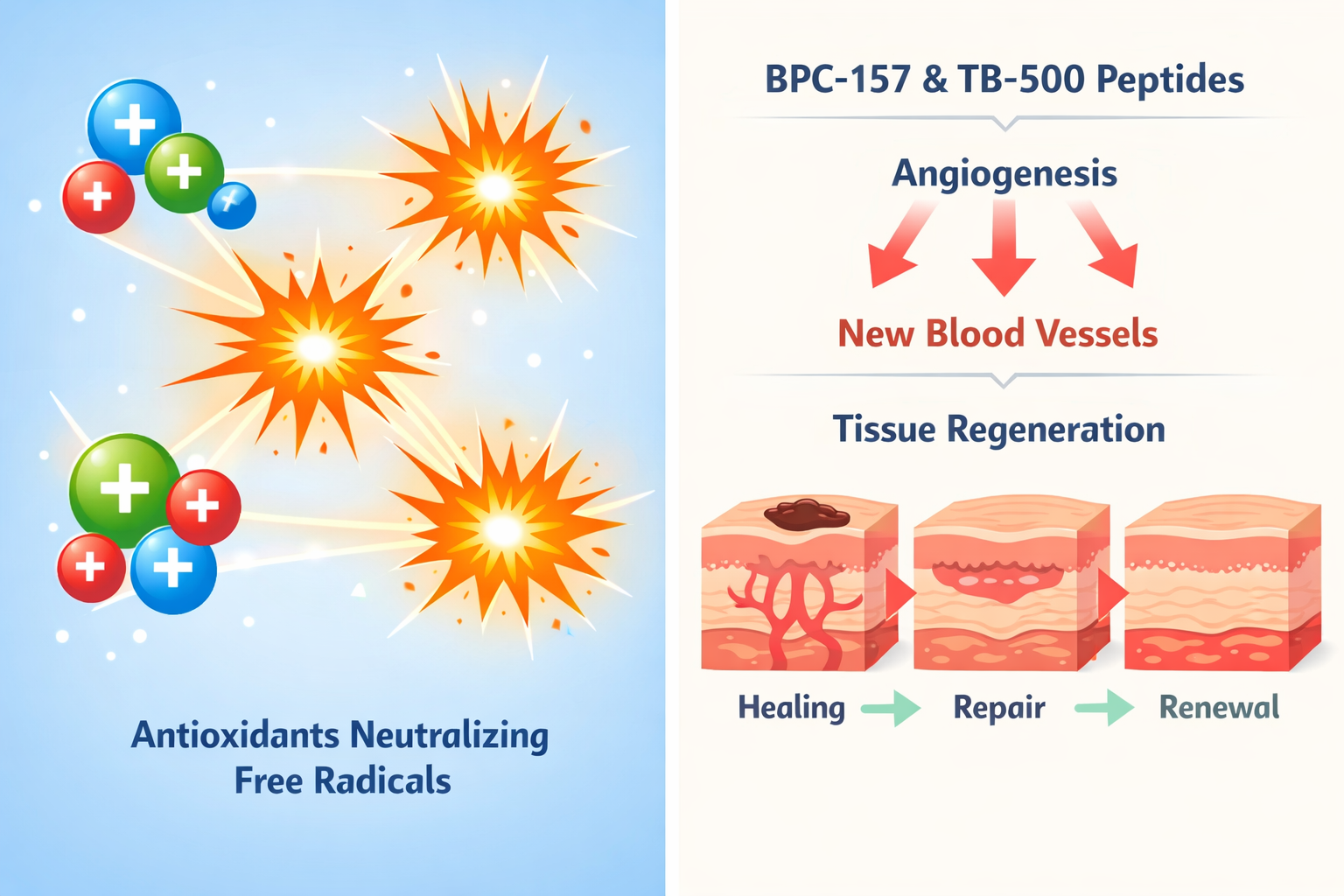
- BPC-157 and TB-500 contribute tissue repair, angiogenesis, and anti-inflammatory signaling that support dermal recovery research.
- Antioxidant defense mechanisms in the blend help protect skin cells from oxidative stress during research models.
- Glow Blend is strictly a research compound with no regulatory approval for human therapeutic use.
What Is Glow Blend Peptide and How Is It Formulated
Glow Blend is a multi-peptide research vial typically totaling 70 mg of active compounds. The formulation combines GHK-Cu (copper peptide), BPC-157, TB-500, and additional supporting peptides into a single blend. This design reflects a growing trend in peptide research toward synergistic stacking rather than single-compound models.
Researchers studying skin biology are drawn to this formulation because it targets multiple pathways simultaneously, collagen synthesis, tissue repair, vascular support, and oxidative stress reduction. For a detailed overview of available peptide research blends, the Glow and Klow peptide blend research page provides useful context on formulation differences.
Important regulatory note: Glow Blend is a research-only compound. It holds no approval from the FDA or any equivalent regulatory body for therapeutic, cosmetic, or clinical use in humans. All research applications must comply with applicable institutional and legal standards.
GHK-Cu and the Collagen-Stimulating Mechanism
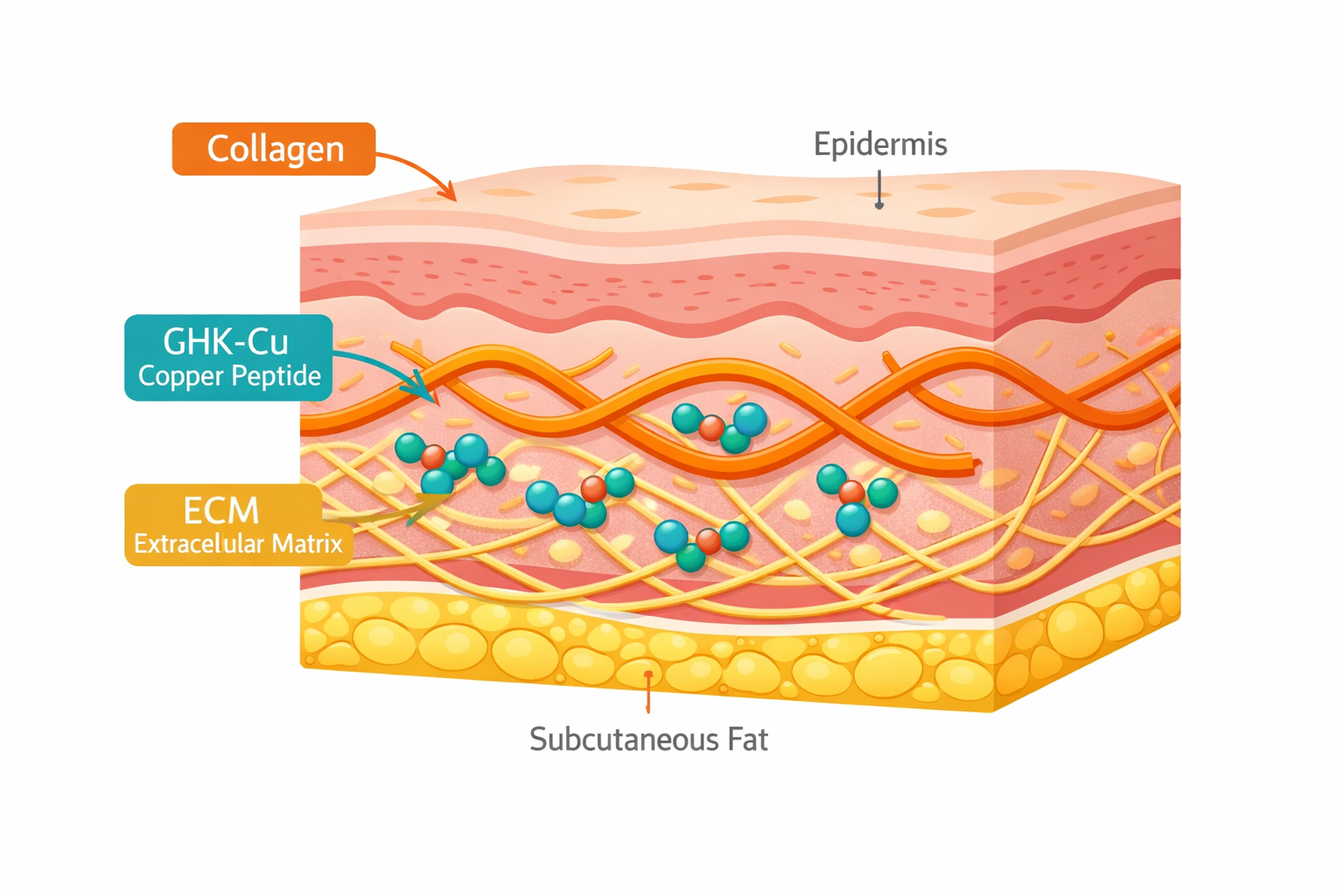
The copper peptide GHK-Cu is the cornerstone of the science behind Glow Blend Peptide's collagen, antioxidant, and skin research applications. GHK-Cu is a naturally occurring tripeptide, glycine-histidine-lysine, that binds copper ions and activates a cascade of biological responses in dermal tissue.
Key actions of GHK-Cu in skin research models include:
- Stimulating fibroblast proliferation and collagen type I and III synthesis
- Upregulating matrix metalloproteinases (MMPs) to remodel damaged extracellular matrix (ECM)
- Activating antioxidant enzymes including superoxide dismutase (SOD) and catalase
- Reducing inflammatory cytokine expression in skin tissue models
"GHK-Cu does not simply stimulate collagen production, it resets the gene expression profile of aging skin cells toward a more youthful state, according to multiple in vitro studies."
The antioxidant dimension of GHK-Cu is particularly relevant. By neutralizing reactive oxygen species (ROS), it protects fibroblasts from oxidative damage that would otherwise impair collagen synthesis. Researchers exploring longevity-related skin mechanisms can find additional GHK-Cu data through GHK-Cu longevity research themes.
BPC-157, TB-500, and Tissue Repair Signaling in Skin Research
While GHK-Cu leads collagen synthesis, BPC-157 and TB-500 provide complementary tissue repair and vascular support that round out the science behind Glow Blend Peptide's collagen, antioxidants, and skin research applications.
BPC-157 (Body Protection Compound-157) is a 15-amino-acid peptide derived from a gastric protein. In skin research models, it demonstrates:
| Mechanism | Research Observation |
|---|---|
| Angiogenesis | Promotes new blood vessel formation in wound models |
| Anti-inflammation | Suppresses COX-2 and pro-inflammatory cytokines |
| Fibroblast activation | Accelerates migration and proliferation in tissue repair |
TB-500 (Thymosin Beta-4) works alongside BPC-157 by regulating actin polymerization, a process essential for cell migration and wound closure. TB-500 also reduces fibrotic scarring in dermal models, making it relevant to skin texture research. For more on TB-500's recovery mechanisms, see TB-500 muscle recovery research themes.
The combination of these two peptides creates overlapping anti-inflammatory and pro-regenerative signals, which researchers hypothesize may amplify dermal repair beyond what either compound achieves alone. Those interested in broader tissue biology context can review the recovery and tissue biology overview.

Antioxidant Defense and Synergistic Research Rationale
Oxidative stress is a primary driver of collagen degradation and premature skin aging. The antioxidant layer within the Glow Blend formulation, driven largely by GHK-Cu but supported by the anti-inflammatory actions of BPC-157, creates a protective environment that may allow collagen synthesis to proceed more effectively in research models.
The synergistic rationale works on three levels:
- Structural repair, GHK-Cu rebuilds ECM architecture while BPC-157 supports vascular delivery of nutrients to repair sites.
- Oxidative protection, Antioxidant enzymes activated by GHK-Cu reduce ROS that would otherwise fragment newly synthesized collagen.
- Inflammatory resolution, TB-500 and BPC-157 suppress chronic low-grade inflammation that impairs fibroblast function.
Researchers sourcing high-purity compounds for skin biology studies should prioritize verified suppliers. Reviewing quality testing protocols ensures research integrity when working with multi-peptide blends. Those building broader research programs may also find the longevity peptide research overview useful for contextualizing skin-focused work within wider aging biology.
Conclusion
The science behind Glow Blend Peptide, collagen, antioxidants, and skin research applications, reflects a well-reasoned multi-target approach to dermal biology. GHK-Cu drives collagen synthesis and antioxidant defense; BPC-157 and TB-500 add angiogenic and anti-inflammatory support; together, they address the primary mechanisms of skin aging and tissue degradation in a single research formulation.
Actionable next steps for researchers:
- Review the full Glow Blend peptide benefits research page before designing study protocols.
- Cross-reference GHK-Cu longevity research data for dose-response context.
- Ensure all research complies with institutional guidelines, this compound carries no regulatory approval for clinical or cosmetic use.
- Source compounds only from suppliers with documented purity testing to maintain experimental validity.
As peptide research in dermatology continues to mature in 2026, multi-compound blends like Glow Blend represent a productive frontier for understanding how targeted molecular interventions can support skin health at the cellular level.