What Is GLP-3 Retatrutide? Triple-Agonist Biology, Receptor Targets, and Why It Is Different From GLP-1
Forty-five percent of participants in a Phase 3 clinical trial lost at least 30% of their body weight — a result once reserved for bariatric surgery. That single data point from the TRIUMPH-1 trial has made retatrutide one of the most closely watched compounds in metabolic medicine today. Understanding what is GLP-3 retatrutide, its triple-agonist biology, receptor targets, and why it is different from GLP-1 drugs already on the market is the essential first step for any researcher or clinician tracking this space.
Key Takeaways
- Retatrutide simultaneously activates three hormone receptors: GLP-1R, GIPR, and the glucagon receptor (GCG-R).
- The informal label "GLP-3" is not a scientific hormone classification — it is shorthand for the compound's triple-receptor profile.
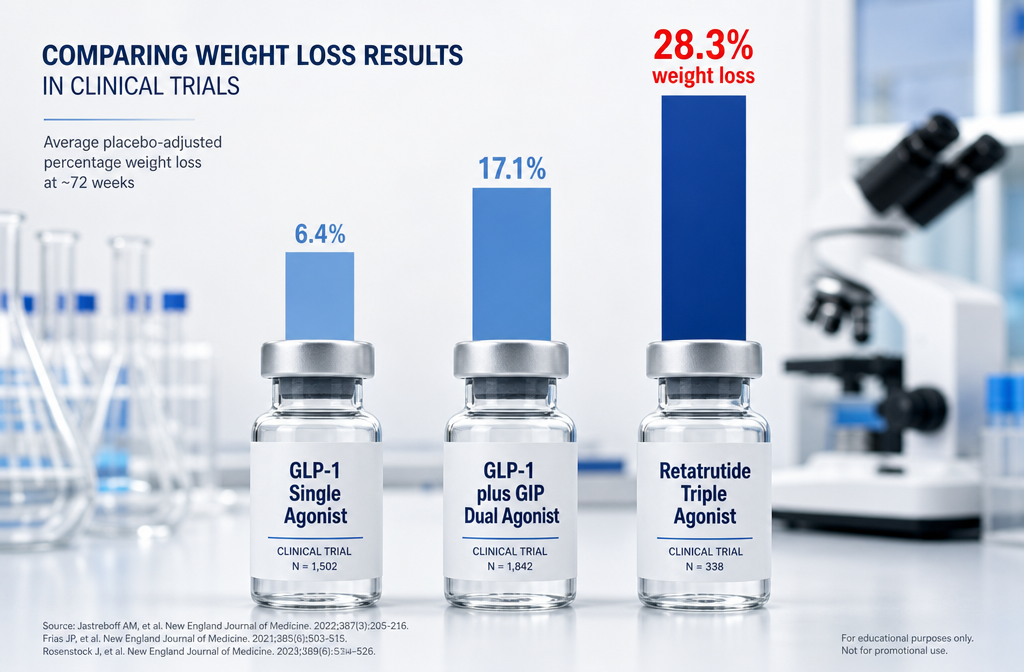
- In the TRIUMPH-1 Phase 3 trial, participants on 12 mg weekly lost an average of 28.3% of body weight over 80 weeks.
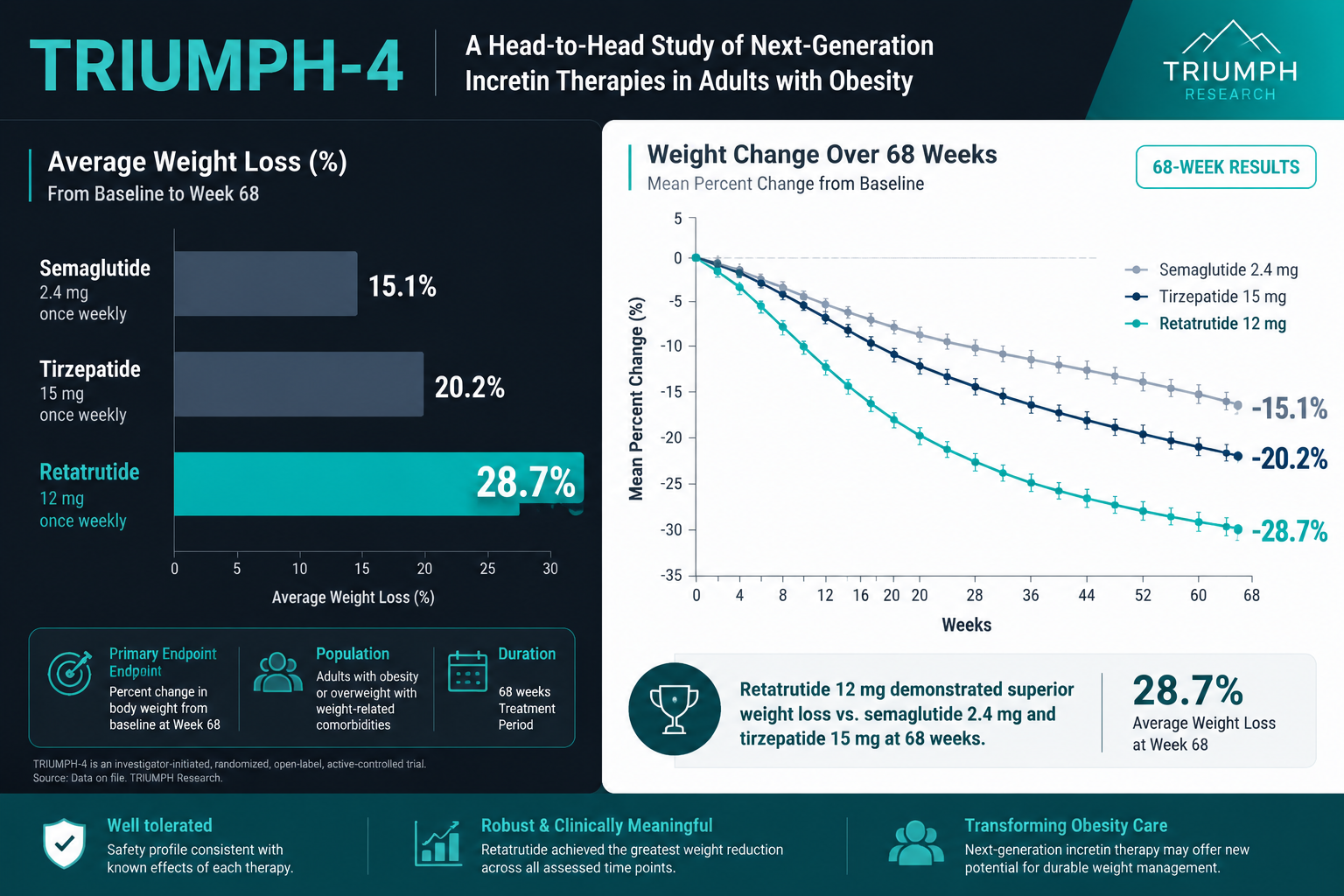
- Retatrutide outperforms single-agonist (semaglutide) and dual-agonist (tirzepatide) therapies in early head-to-head comparisons.
- As of 2026, retatrutide has not received FDA approval and remains in Phase 3 development under Eli Lilly.
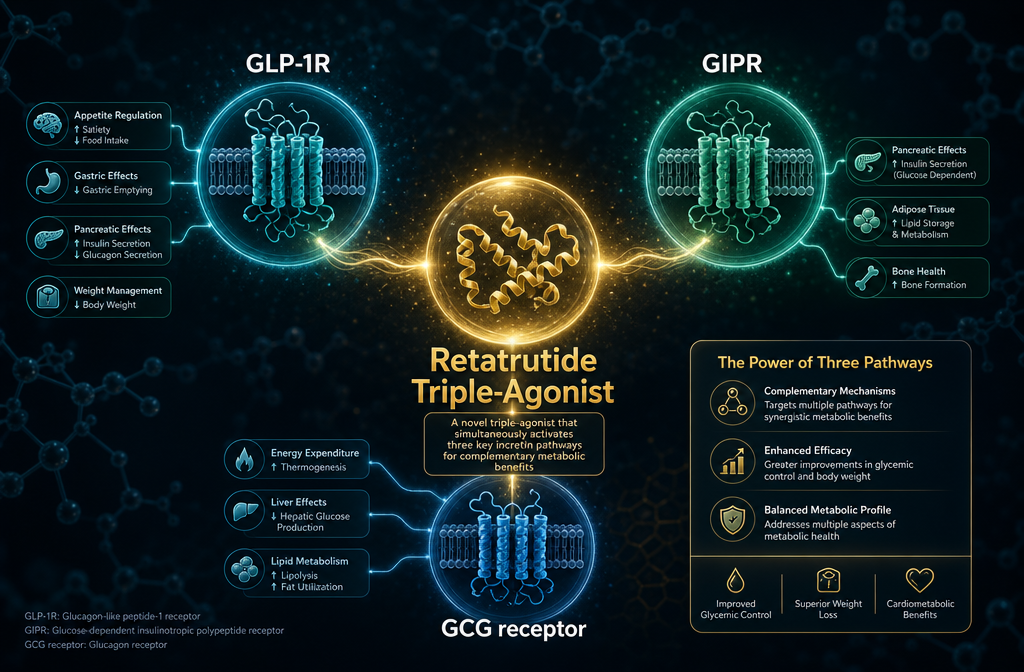
The Triple-Agonist Biology Behind Retatrutide
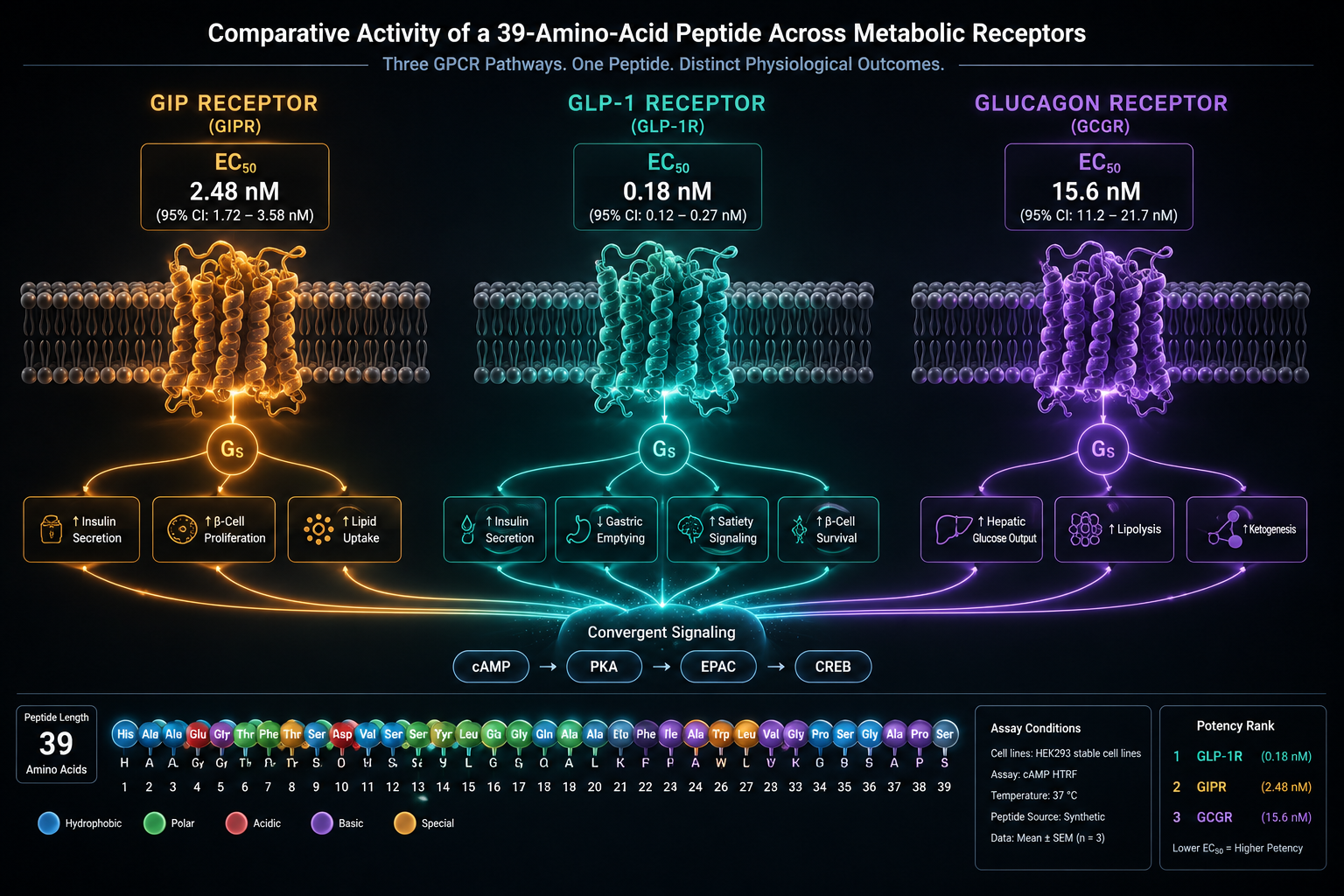
Retatrutide is a synthetic peptide engineered to bind and activate three distinct incretin and metabolic hormone receptors at the same time. Each receptor plays a separate but complementary role in energy regulation.
| Receptor | Primary Role | Contribution to Retatrutide's Effect |
|---|---|---|
| GLP-1R (Glucagon-Like Peptide-1) | Insulin secretion, appetite suppression | Reduces hunger, slows gastric emptying |
| GIPR (Glucose-Dependent Insulinotropic Polypeptide) | Insulin amplification, fat metabolism | Enhances insulin response, supports fat tissue signaling |
| GCG-R (Glucagon Receptor) | Energy expenditure, hepatic glucose output | Increases calorie burn, reduces liver fat |
This simultaneous three-receptor engagement is what separates retatrutide from every approved obesity drug on the market. The glucagon receptor component is particularly significant: glucagon typically raises blood sugar, but when its receptor is activated alongside GLP-1R and GIPR, the net effect shifts toward increased thermogenesis and fat oxidation rather than hyperglycemia.
Researchers exploring the GLP-1 generations overview will recognize this as a logical progression from first-generation single-agonist molecules toward increasingly complex multi-receptor strategies.
Why the "GLP-3" Label Is Informal — and What It Actually Means
The term "GLP-3" does not refer to a real hormone. No such molecule exists in human physiology. The label emerged informally to describe retatrutide's position as the third generation of GLP-based obesity therapies:
- Generation 1: GLP-1 single agonists (e.g., semaglutide / Wegovy)
- Generation 2: GLP-1 + GIP dual agonists (e.g., tirzepatide / Zepbound)
- Generation 3: GLP-1 + GIP + Glucagon triple agonists (retatrutide)
The correct scientific description is triple hormone receptor agonist. Researchers browsing retatrutide research and catalog resources or the GLP-1 Reta product tag will encounter both terms, but the informal "GLP-3" label should always be understood as generational shorthand rather than pharmacological classification.
How Retatrutide Differs From GLP-1 Drugs: Receptor Targets and Clinical Outcomes
This is the core question for anyone asking what is GLP-3 retatrutide and why it is different from GLP-1. The differences operate on two levels: mechanistic and clinical.
Mechanistically, semaglutide targets only GLP-1R. Tirzepatide adds GIPR. Retatrutide adds the glucagon receptor on top of both. That third receptor drives a meaningful increase in resting energy expenditure — the body burns more calories even at rest — which neither of the earlier drugs can replicate.
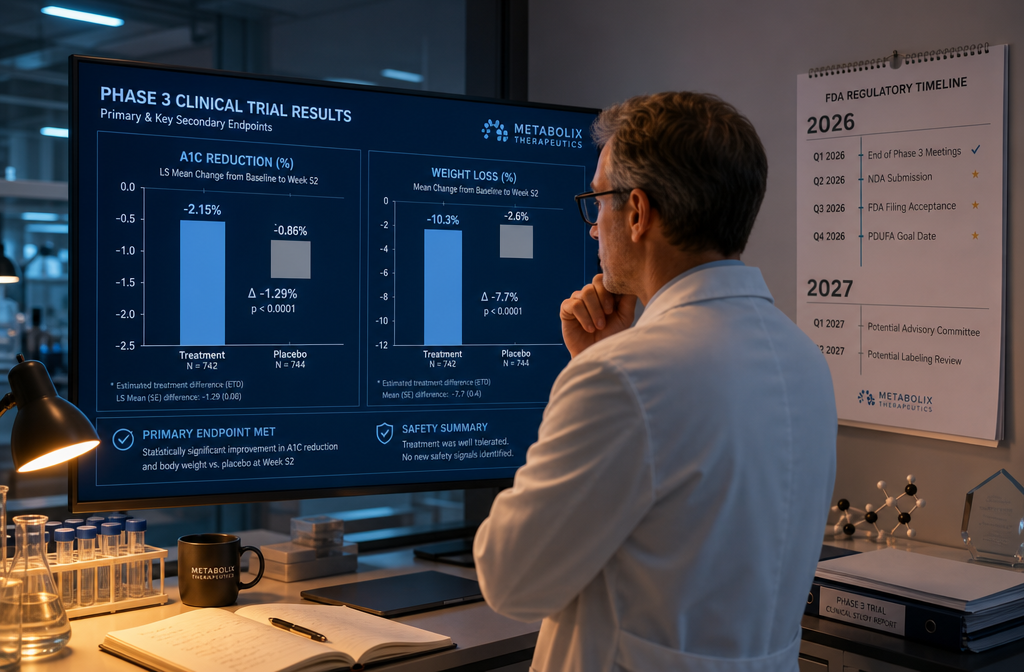
Clinically, the TRIUMPH-1 Phase 3 trial reported an average weight loss of 28.3% (approximately 70.3 pounds) over 80 weeks at the 12 mg weekly dose. By comparison, semaglutide typically produces roughly 15% weight loss, and tirzepatide reaches approximately 20-22%. Retatrutide also demonstrated an A1C reduction of up to 2.0% over 40 weeks in participants with type 2 diabetes, suggesting strong glycemic benefit beyond weight loss alone.
"Retatrutide's glucagon receptor component is the differentiating factor — it converts what would otherwise be a pure appetite-suppression strategy into a genuine energy-expenditure intervention."
Side effects remain consistent with the incretin drug class: nausea, diarrhea, constipation, and vomiting, all dose-dependent and generally manageable. Those interested in how metabolic peptides interact with energy systems may also find value in reviewing mitochondrial longevity research and AOD9604 metabolic research for broader context.
For researchers sourcing compounds for study, reviewing lab-tested peptide standards and certificate of analysis documentation ensures quality benchmarks are met before any research protocol begins.
As of 2026, retatrutide is not FDA-approved. Eli Lilly anticipates filing for approval in 2026-2027, with potential market availability by 2027 or 2028. Those planning research timelines can consult the GLP-3 research planning and catalog navigation guide for sourcing and protocol considerations.
Conclusion
Retatrutide represents a genuine structural advance over existing GLP-1 therapies. Its triple-agonist biology — engaging GLP-1R, GIPR, and the glucagon receptor simultaneously — produces weight loss outcomes that approach bariatric surgery benchmarks and glycemic improvements that matter for type 2 diabetes management. The informal "GLP-3" label is a useful shorthand, but researchers should understand it as a generational marker, not a hormone designation.
Actionable next steps for researchers in 2026:
- Review the TRIUMPH-1 Phase 3 trial data in detail to understand dose-response relationships.
- Compare retatrutide's receptor profile against tirzepatide using the GLP-1 peptide generational research overview.
- Verify compound purity standards before initiating any research protocol by consulting available COA documentation.
- Monitor FDA filing timelines, currently projected for 2026-2027, to align research planning accordingly.