Complement‑Dependent Cytotoxicity and Polypeptide Peptides: How Immune Assays Inform BPC‑157, GHK‑Cu, and MOTS‑c Safety Research
Fewer than a dozen published studies have used formal complement-dependent cytotoxicity (CDC) assays to evaluate short synthetic peptides, yet CDC testing remains one of the most informative tools available for predicting whether a polypeptide will trigger an unwanted immune cascade. That gap matters enormously as research interest in BPC-157, GHK-Cu, and MOTS-c continues to grow in 2026.
Understanding how complement-dependent cytotoxicity and polypeptide peptides interact, and how immune assays inform BPC-157, GHK-Cu, and MOTS-c safety research, is no longer a niche immunology question. It is central to responsible peptide science.
Key Takeaways
- Complement-dependent cytotoxicity (CDC) assays measure whether a compound activates the complement system and triggers cell lysis, making them a critical in vitro safety screen.
- Short synthetic peptides like BPC-157, GHK-Cu, and MOTS-c have low molecular weights that generally reduce immunogenic risk, but formal CDC data remain sparse.
- Human safety data for these peptides in 2026 are still limited to small, short-term studies using basic laboratory panels rather than dedicated immunogenicity assays.
- Peptide purity and manufacturing quality directly influence immune assay outcomes, making sourcing from a verified peptide manufacturer a critical research variable.
- Immune assay frameworks developed for biologics are being adapted for peptide research, but standardized CDC protocols for this class of compounds do not yet exist.
What Is Complement-Dependent Cytotoxicity and Why Does It Apply to Polypeptide Research
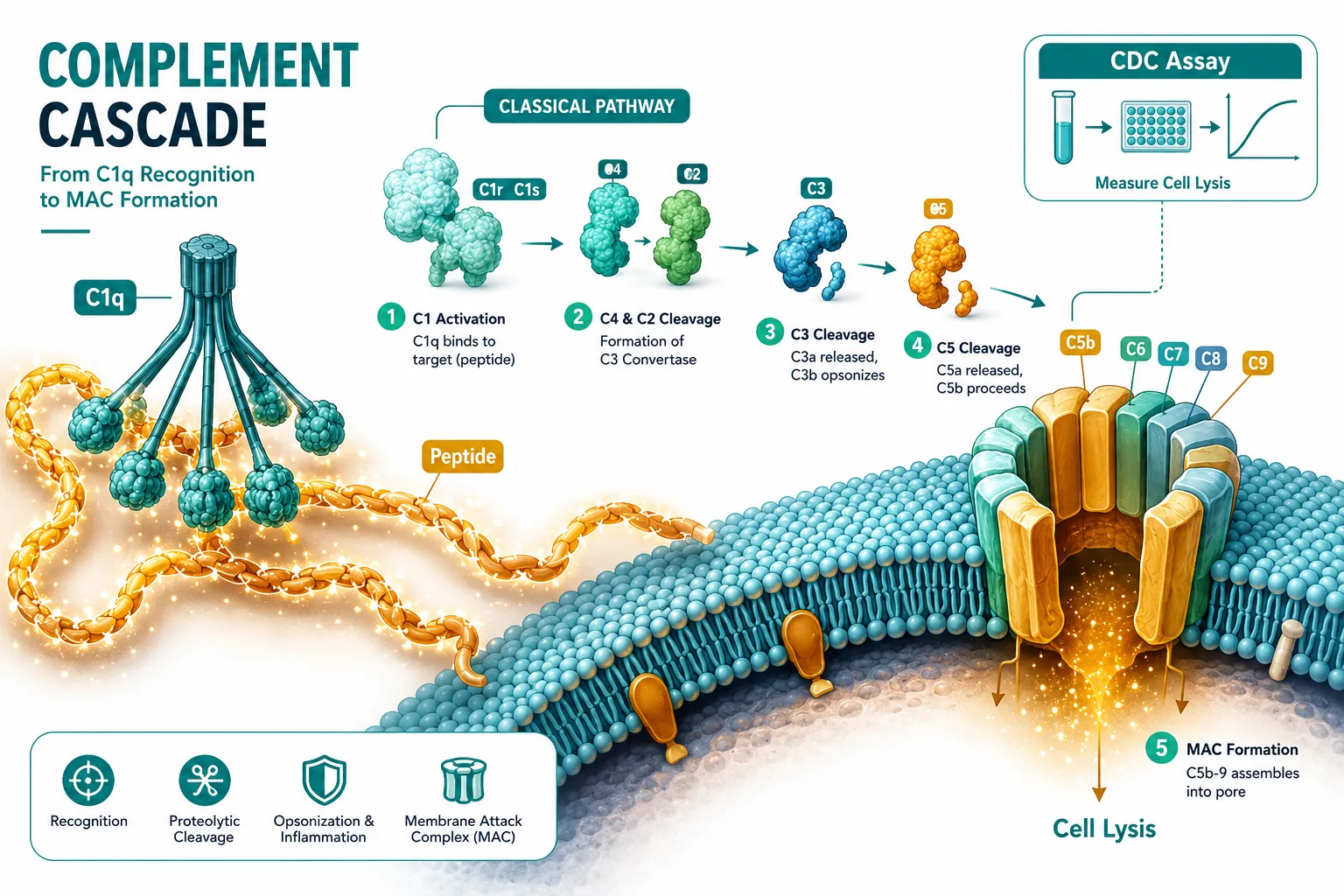
The complement system is a network of plasma proteins that, when activated, can destroy cells by forming a membrane attack complex (MAC). CDC assays exploit this mechanism in vitro: a target cell is exposed to a test compound plus serum containing complement proteins. If the compound binds to the cell surface and recruits C1q, the recognition protein that triggers the classical complement pathway, cell lysis follows.
Why does this matter for peptides?
Most therapeutic peptides are too small to directly activate complement through the classical pathway. However, several factors can change that picture:
- Aggregation: Peptide aggregates can mimic immune complexes and activate C1q.
- Carrier proteins: Peptides conjugated to larger proteins for stability may inherit immunogenic properties.
- Impurities: Endotoxin contamination from synthesis can independently activate the complement alternative pathway.
- Sequence homology: Rare sequence similarities to known complement-activating proteins can trigger cross-reactivity.
This is why complement-dependent cytotoxicity and polypeptide peptides research, including how immune assays inform BPC-157, GHK-Cu, and MOTS-c safety research, cannot simply assume that small size equals immunological silence.
"Low molecular weight does not guarantee complement neutrality. Aggregation state, purity, and formulation all modulate immune assay outcomes."
How Immune Assays Are Applied to BPC-157, GHK-Cu, and MOTS-c Safety Profiles

Each of these three peptides presents a distinct immunological profile worth examining separately.
BPC-157 is a 15-amino-acid synthetic peptide derived from a gastric protein sequence. Its small size places it below the typical threshold for T-cell-mediated immunogenicity. Published human data through 2026 remain limited to small, short-term trials using standard metabolic and hepatic safety panels, not dedicated CDC or complement activation assays. Preclinical data are more extensive and have not flagged complement activation, though formal CDC endpoint reporting is absent from most study designs. Research on oral BPC-157 formulations adds another variable, since mucosal delivery alters how peptides interact with immune surveillance.
GHK-Cu (copper peptide glycyl-L-histidyl-L-lysine) is a tripeptide-copper complex. Its extremely small size, three amino acids, makes classical complement activation via direct binding highly unlikely. However, copper ions in excess can influence complement regulation indirectly. Researchers reviewing GHK-Cu longevity research themes should note that available safety data rely on cytotoxicity assays (MTT, LDH release) rather than complement-specific endpoints. Those interested in topical applications can explore topical GHK-Cu research for context on delivery-route differences.
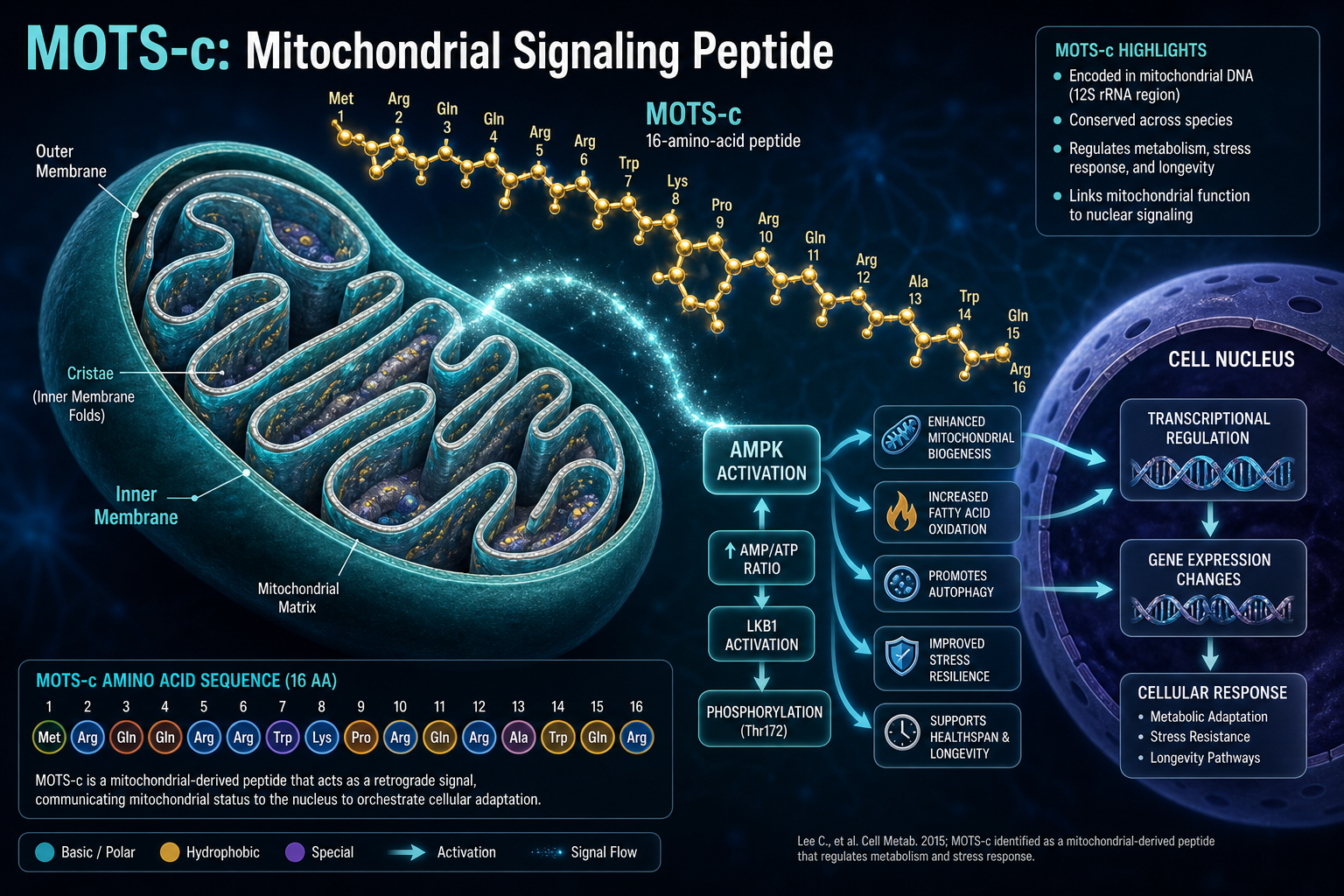
MOTS-c is a 16-amino-acid mitochondria-derived peptide with metabolic regulatory functions. Because it originates from mitochondrial DNA, its sequence is evolutionarily conserved, a feature that generally reduces immunogenic risk. Detailed MOTS-c mitochondrial dynamics research has focused on metabolic endpoints rather than immune activation. The MOTS-c and SLU-PP332 interaction research similarly does not report complement assay data.
| Peptide | Amino Acids | Formal CDC Data Available | Primary Safety Assay Used |
|---|---|---|---|
| BPC-157 | 15 | No | Basic metabolic labs |
| GHK-Cu | 3 | No | MTT/LDH cytotoxicity |
| MOTS-c | 16 | No | Metabolic endpoints |
Bridging the Gap: Applying CDC Frameworks to Future Peptide Safety Research

The absence of standardized CDC protocols for synthetic peptides is not a permanent barrier, it is a research opportunity. Immunogenicity frameworks developed for monoclonal antibodies and biologic therapies are being adapted for smaller peptide classes, and complement-dependent cytotoxicity and polypeptide peptides research is beginning to appear in the literature as this adaptation accelerates.
Practical steps researchers can take in 2026:
- Use complement consumption assays (CH50 or AH50) as a first-pass screen before full CDC endpoint testing.
- Test at multiple concentrations to capture dose-dependent complement activation that might be missed at a single test point.
- Control for endotoxin using the Limulus Amebocyte Lysate (LAL) test to separate peptide-driven from contaminant-driven complement activation.
- Assess aggregation state via dynamic light scattering before immune assay runs.
Purity is a non-negotiable variable in this process. Researchers working with LL-37, another innate immune peptide, face similar assay challenges, as outlined in LL-37 innate research themes. Comparing how immune assays inform BPC-157, GHK-Cu, and MOTS-c safety research alongside related peptides like SS-31, explored in SS-31 mitochondrial research themes, can help build a comparative immunological picture across peptide classes.
Conclusion
Complement-dependent cytotoxicity and polypeptide peptides represent an underexplored intersection in safety science. For BPC-157, GHK-Cu, and MOTS-c, formal CDC assay data are largely absent from the published record as of 2026, a gap that researchers, manufacturers, and regulatory scientists should treat as a priority.
Actionable next steps:
- Advocate for complement activation endpoints in future peptide safety trial designs.
- Prioritize high-purity peptide sources, since impurities are a leading confounder in immune assay results.
- Cross-reference immune assay findings with peptide-class comparators to build a broader safety database.
- Review GHK-Cu peptides for sale and MOTS-c research peptides only from suppliers who provide certificates of analysis and third-party purity verification.
The science of peptide immunogenicity is maturing. Applying rigorous CDC frameworks now will strengthen the evidence base that researchers and regulators will rely on for years to come.