Tesofensine Peptide Research: Mechanism, Appetite Suppression, and Neuropeptide Y Pathways
Obesity affects more than one billion people worldwide, yet fewer than five approved pharmacological treatments exist that produce sustained, clinically meaningful weight loss. That gap has driven researchers toward compounds like tesofensine, a triple monoamine reuptake inhibitor that first appeared in neurodegenerative disease trials before its dramatic weight-loss effects redirected scientific attention entirely. Tesofensine peptide research, mechanism, appetite suppression, and neuropeptide Y pathways have since become central themes in metabolic science, making this compound one of the more closely watched molecules in preclinical and clinical obesity research.

Key Takeaways
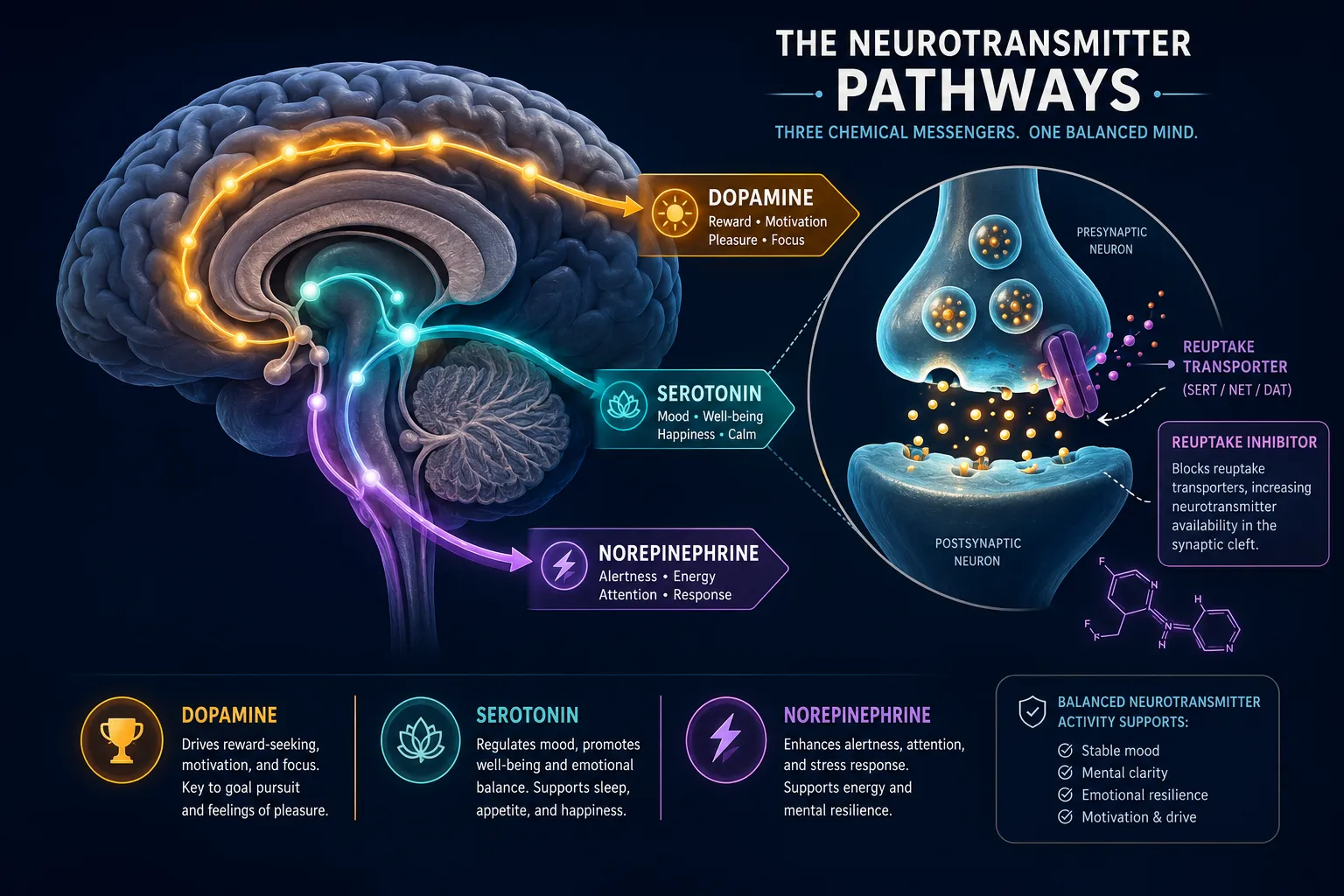
- Tesofensine blocks the reuptake of dopamine, norepinephrine, and serotonin simultaneously, elevating extracellular levels of all three neurotransmitters.
- Originally developed for Alzheimer's and Parkinson's diseases, its significant weight-loss side effects redirected research toward obesity treatment.
- Phase 2 clinical trials demonstrated approximately 10% body weight reduction, though cardiovascular side effects remain a barrier to approval.
- Appetite suppression appears to involve GABAergic neuron silencing in the lateral hypothalamus and indirect adrenoceptor and dopamine receptor stimulation.
- As of 2026, tesofensine has not received regulatory approval for obesity treatment, and research continues to refine its safety profile.
Understanding the Mechanism Behind Tesofensine Peptide Research
Tesofensine operates as a triple monoamine reuptake inhibitor (TMRI). Its primary action is blocking presynaptic transporters responsible for clearing dopamine, norepinephrine, and serotonin from the synaptic cleft. By preventing reuptake, tesofensine raises extracellular concentrations of all three neurotransmitters simultaneously, a broader mechanism than compounds that target only one or two pathways.
This multi-target approach distinguishes tesofensine from older single-mechanism agents. The elevated monoamine activity produces downstream effects across several brain regions involved in energy balance, reward processing, and satiety signaling.
Key neurotransmitter roles in tesofensine's mechanism:
| Neurotransmitter | Primary Role in Energy Balance |
|---|---|
| Dopamine | Reward signaling, motivation to eat |
| Norepinephrine | Sympathetic activation, thermogenesis |
| Serotonin | Satiety, mood, food intake regulation |
Research in diet-induced obese (DIO) rat models showed that tesofensine reverses abnormally low forebrain dopamine levels, a deficit commonly observed in obesity. Restoring dopamine tone appears to reduce the reward-driven motivation to overeat, contributing meaningfully to caloric restriction without direct appetite suppression alone.
For researchers exploring how metabolic peptides interact with neurotransmitter systems, understanding compounds like tesa and its metabolic effects offers useful comparative context for how different mechanisms produce body composition changes.
Appetite Suppression Pathways: What the Research Shows
Tesofensine peptide research on mechanism, appetite suppression, and neuropeptide Y pathways reveals that hunger reduction is not a single-step process. Multiple neural circuits are engaged.
Lateral Hypothalamus and GABAergic Neurons
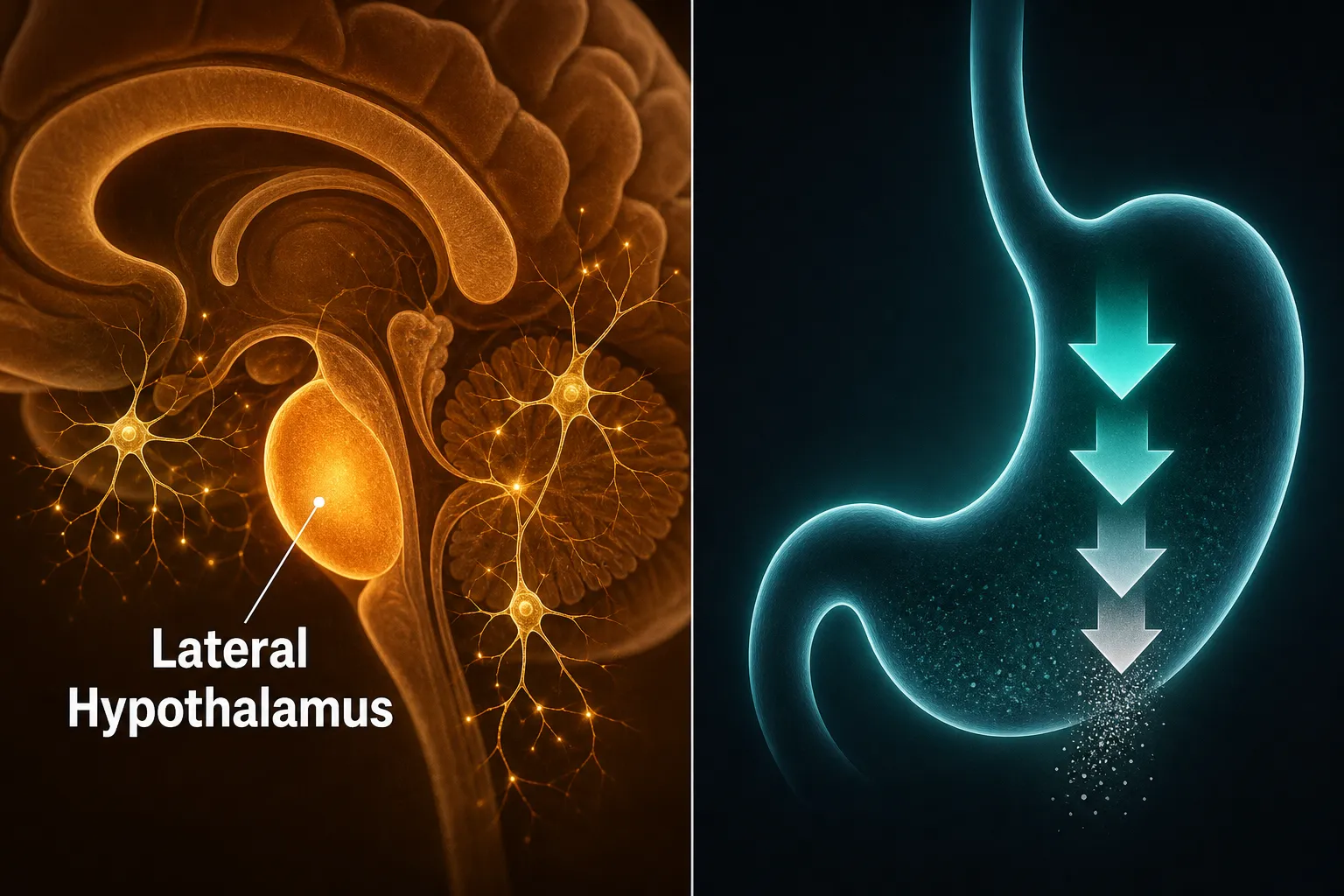
Recent research points to a compelling mechanism: tesofensine may silence GABAergic (inhibitory) neurons in the lateral hypothalamus (LH). The lateral hypothalamus is classically known as a hunger-promoting region. When GABAergic neurons in this area are suppressed, the net effect is reduced drive to seek and consume food.
"Silencing inhibitory neurons in a hunger-promoting brain region creates a functional brake on appetite, a mechanism distinct from simple satiety signaling."
This finding suggests tesofensine's appetite effects go beyond monoamine elevation and involve direct modulation of hypothalamic circuitry.
Adrenoceptor and Dopamine Receptor Involvement
Studies in DIO rats demonstrated that tesofensine suppresses appetite through indirect stimulation of alpha-1 adrenoceptors and dopamine D1 receptors. These receptor pathways are not directly activated by tesofensine itself, rather, elevated norepinephrine and dopamine levels produced by reuptake inhibition create the downstream receptor stimulation.
This indirect mechanism has important implications for researchers studying metabolic modulation compounds and how receptor selectivity shapes both efficacy and side effect profiles.
Phase 2 Clinical Trial Findings
In a Phase 2 clinical trial, tesofensine produced approximately 10% body weight reduction in participants, a result that significantly outperformed placebo and compared favorably to other approved anti-obesity agents at the time. However, dose-dependent increases in heart rate and blood pressure emerged as consistent findings, raising cardiovascular safety concerns that have since slowed regulatory progress.
Neuropeptide Y Pathways and Tesofensine: Current Research Landscape

Neuropeptide Y (NPY) is one of the most potent appetite-stimulating peptides in the central nervous system. It is produced primarily in the arcuate nucleus of the hypothalamus and acts on multiple receptor subtypes (Y1 through Y5) to promote food intake, reduce energy expenditure, and regulate fat storage.
The intersection of tesofensine peptide research on mechanism, appetite suppression, and neuropeptide Y pathways is an area of active scientific interest, though not without important caveats.
What current research suggests:
- Elevated dopamine and norepinephrine levels from tesofensine's reuptake inhibition may indirectly modulate NPY neuronal activity, since monoaminergic neurons interact with NPY-expressing cells in the hypothalamus.
- Norepinephrine, in particular, has well-established inhibitory effects on NPY release via alpha-2 adrenoceptor signaling in the arcuate nucleus.
- However, direct, conclusive evidence that tesofensine specifically targets NPY receptor subtypes has not been established in published literature as of 2026.
This distinction matters for researchers. Tesofensine likely influences NPY pathways as a secondary consequence of monoamine elevation rather than as a primary pharmacological target. Understanding this distinction helps frame tesofensine within the broader landscape of appetite-regulating compounds.
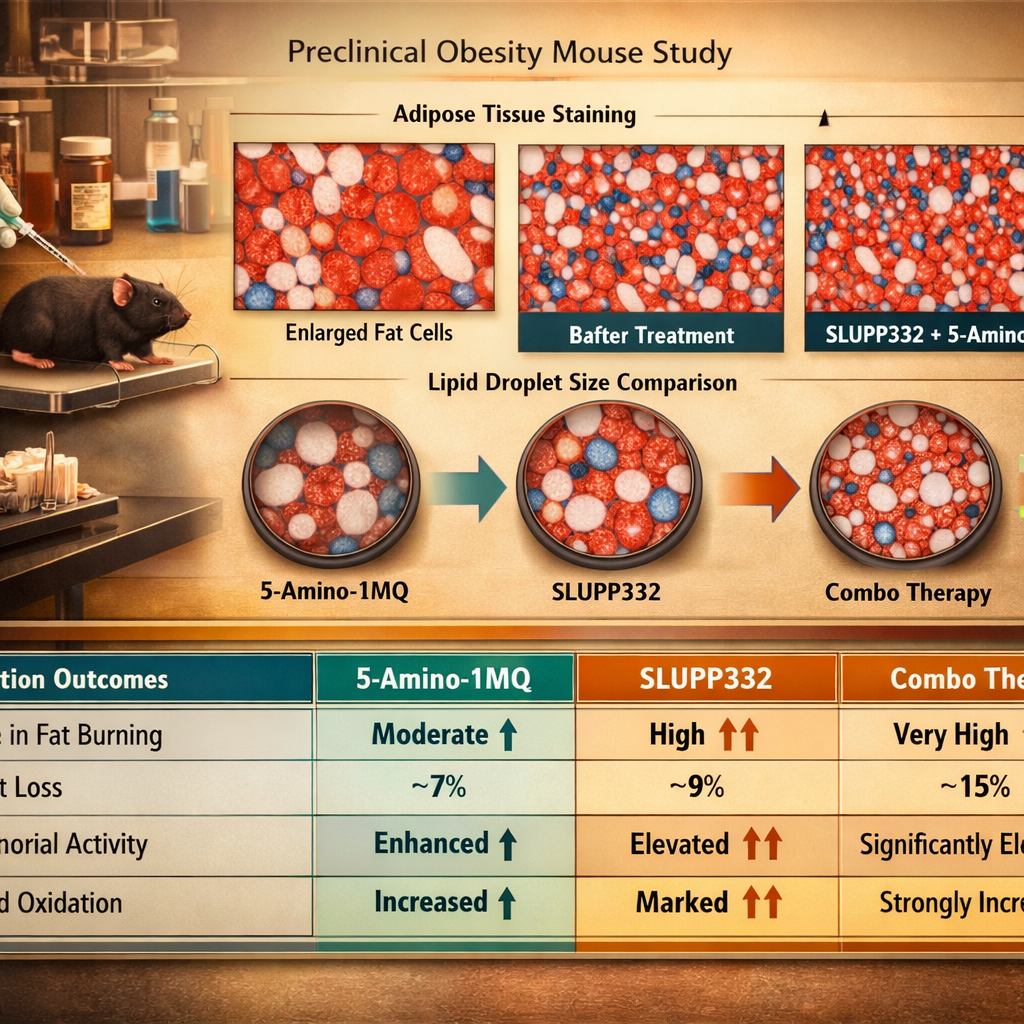
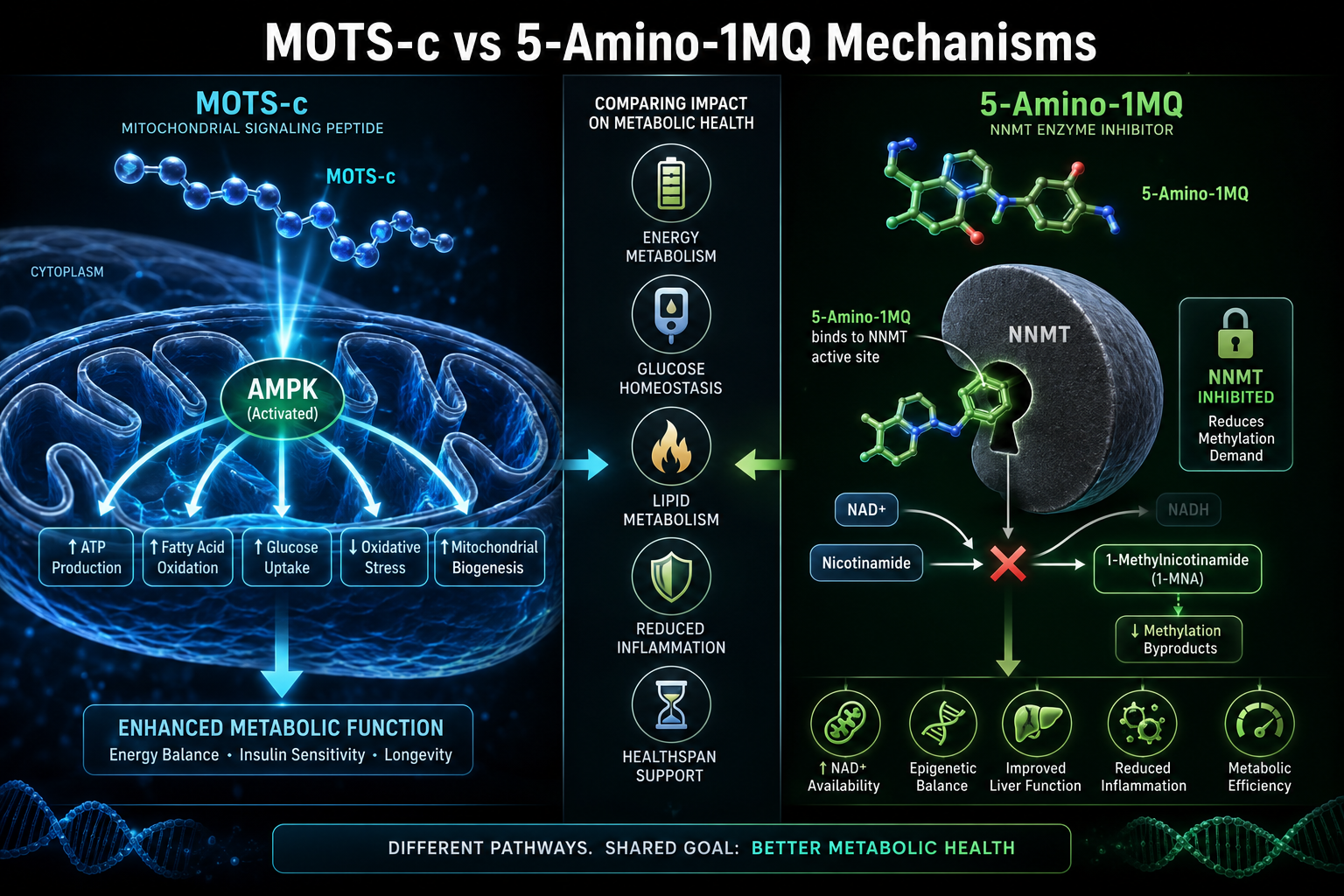
Researchers interested in complementary metabolic peptide mechanisms may also find value in reviewing MOTS-c mitochondrial research themes and SLU-PP-332 metabolic research for comparative mechanistic insights.
Regulatory and Safety Status in 2026
As of 2026, tesofensine has not received regulatory approval for obesity treatment from the FDA or EMA. The cardiovascular concerns, primarily elevated heart rate and blood pressure at therapeutic doses, remain the primary obstacle. Ongoing research is exploring whether lower doses combined with adjunct therapies might preserve efficacy while reducing cardiovascular burden.
For researchers building a broader understanding of peptide-based metabolic research, the ultimate guide to peptide therapy provides foundational context, while tesofensine product research information offers compound-specific details.
Conclusion
Tesofensine represents a scientifically compelling case study in how unexpected clinical findings, in this case, significant weight loss during neurodegenerative disease trials, can redirect an entire research program. Its triple monoamine reuptake inhibition mechanism, combined with evidence of lateral hypothalamic GABAergic neuron silencing and indirect NPY pathway modulation, makes it a multifaceted compound for researchers studying metabolic health.
Actionable next steps for researchers in 2026:
- Review published Phase 2 trial data to understand the dose-response relationship between tesofensine and cardiovascular outcomes.
- Examine preclinical DIO rat studies for detailed mechanistic data on adrenoceptor and dopamine D1 receptor involvement.
- Explore how tesofensine's monoaminergic effects may interact with NPY-expressing arcuate nucleus neurons in future study designs.
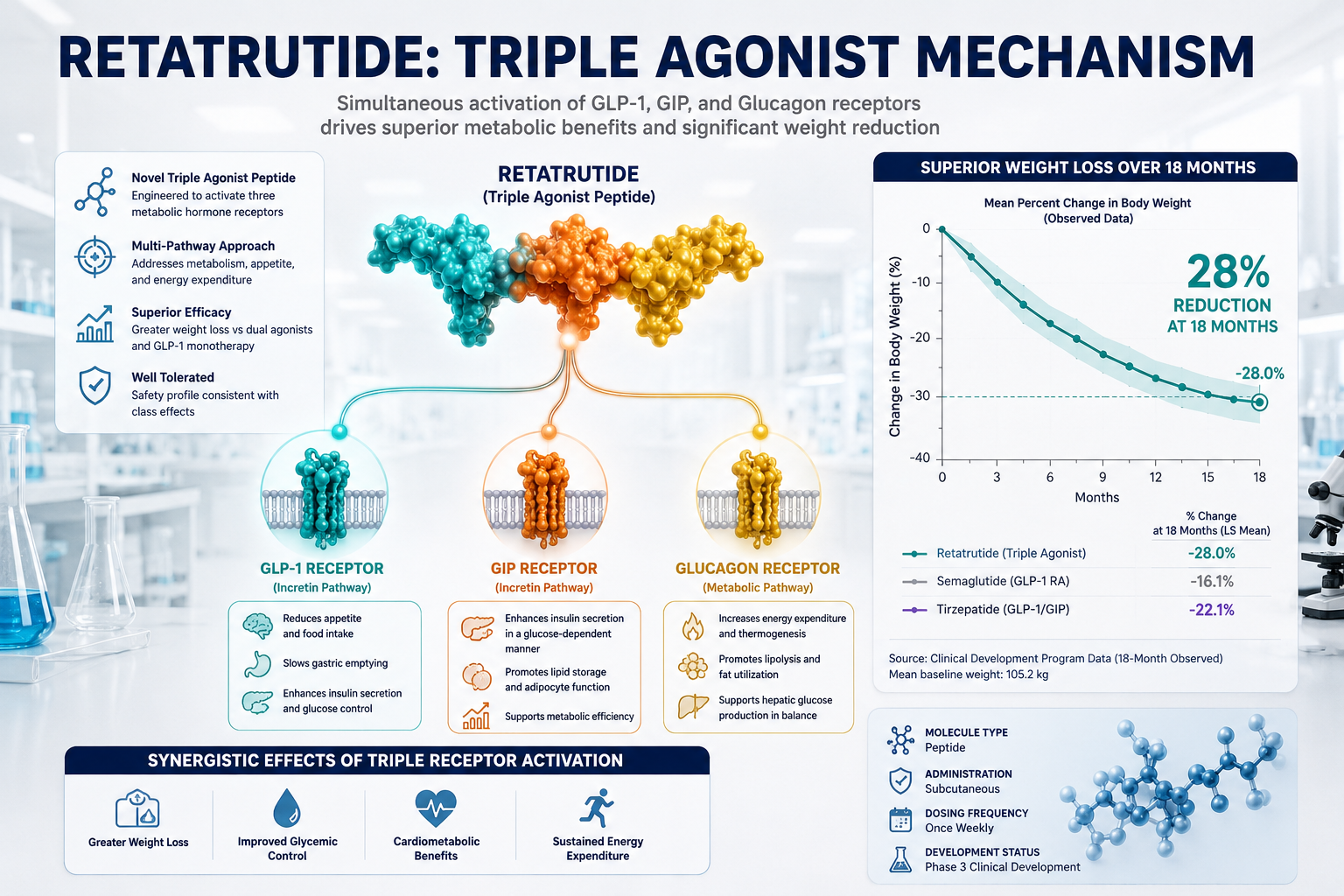
- Consider comparative analysis with GLP-1 pathway compounds to contextualize tesofensine's mechanism within the broader anti-obesity pharmacology landscape.
- Monitor regulatory developments, as ongoing safety refinement research may shift tesofensine's clinical status.
The science surrounding tesofensine continues to evolve. For researchers committed to understanding novel compounds in metabolic health and weight management, it remains a high-value subject worthy of rigorous investigation.