
Retatrutide Clinical Trials Explained: Phase 2 to Phase 3 Outcomes, Endpoints, and What Researchers Should Track
A drug that produces roughly 28% average body weight loss in 18 months — approaching outcomes typically associated with bariatric surgery — demands a clear-eyed reading of the trial record behind it. That is exactly what this guide delivers. Understanding the Retatrutide Clinical Trials Explained: Phase 2 to Phase 3 Outcomes, Endpoints, and What Researchers Should Track framework helps researchers, clinicians, and informed readers interpret efficacy data, dose-escalation patterns, and cardiometabolic endpoints without getting lost in trial jargon.
Key Takeaways
- Retatrutide is a once-weekly triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously.
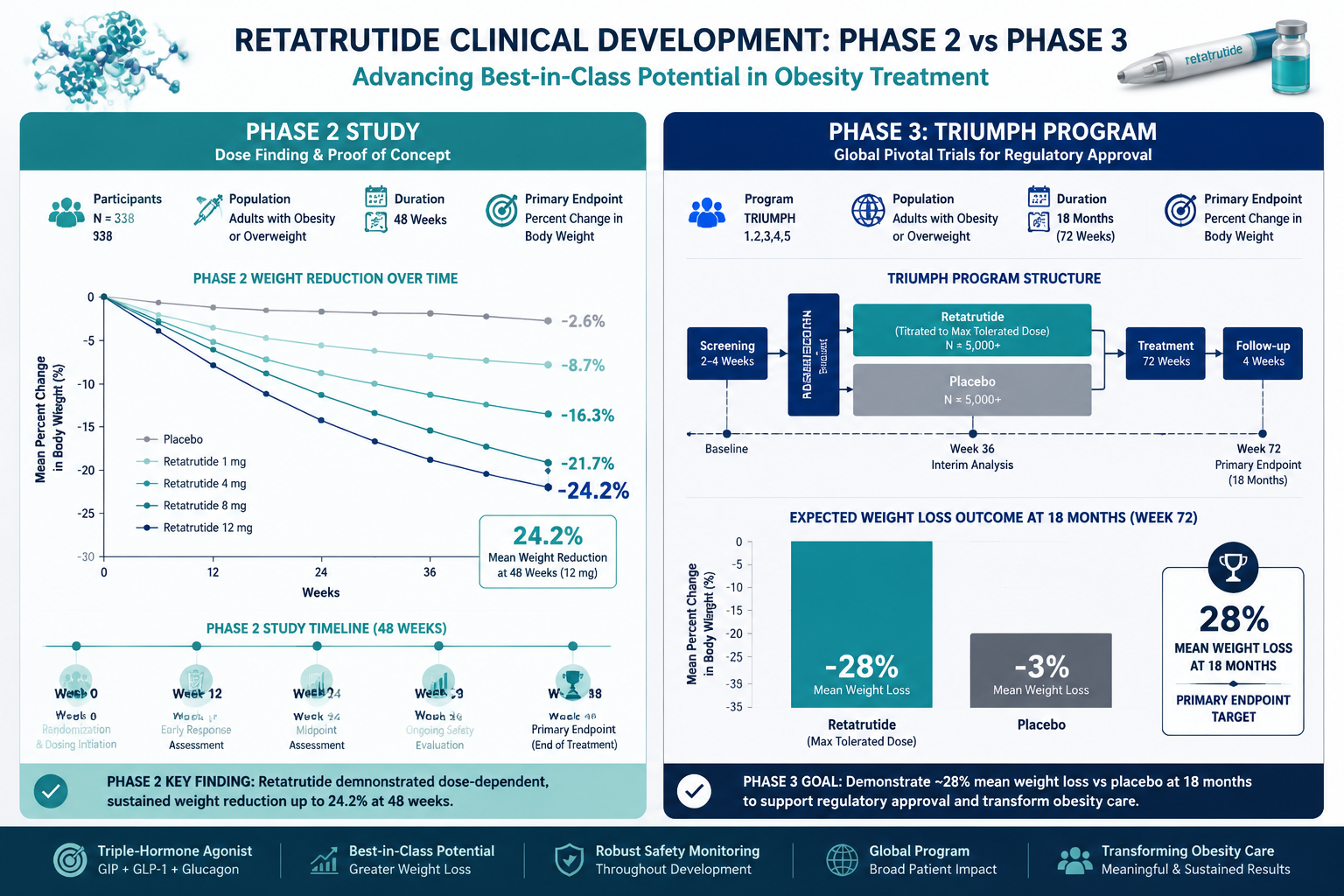
- Phase 2 trials showed up to 24.2% weight reduction at 48 weeks; Phase 3 data now shows approximately 28% over 18 months.
- The TRIUMPH Phase 3 program spans obesity, type 2 diabetes, knee osteoarthritis, and obstructive sleep apnea.
- Gastrointestinal adverse events are the most common safety signal, with discontinuation rates of 12-18% at higher doses.
- Researchers should track both primary efficacy endpoints and secondary cardiometabolic biomarkers across dose cohorts.
From Phase 2 to Phase 3: How the Trial Record Builds
The Retatrutide Clinical Trials Explained: Phase 2 to Phase 3 Outcomes, Endpoints, and What Researchers Should Track story begins with mechanism. Retatrutide activates three receptors — GLP-1, GIP, and glucagon — in a single once-weekly subcutaneous injection. This triple-agonist profile distinguishes it from earlier GLP-1 mono-agonists and dual agonists. For context on how GLP-1 receptor pharmacology has evolved across generations, the GLP-1 generations overview provides useful background, and a deeper look at dual receptor agonism in research shows why adding a third receptor target changes the efficacy ceiling.
Phase 2 results published in a landmark study demonstrated a mean weight reduction of up to 24.2% at 48 weeks in adults with obesity or overweight without diabetes. Crucially, this was dose-dependent: participants on higher dose arms consistently outperformed those on lower doses, establishing the dose-escalation rationale that Phase 3 protocols would formalize.
Phase 3 results from the TRIUMPH program have now confirmed and extended those findings. In an obesity-focused trial, retatrutide produced approximately 28% average weight loss over 18 months — a figure that rivals surgical intervention. The TRANSCEND-T2D-1 Phase 3 trial in type 2 diabetes reported a mean HbA1c reduction of 1.94% alongside a 15.3% decrease in body weight over 40 weeks in adults inadequately controlled by diet and exercise alone.
| Trial Phase | Population | Duration | Key Outcome |
|---|---|---|---|
| Phase 2 | Obesity/Overweight (no T2D) | 48 weeks | Up to 24.2% weight loss |
| Phase 3 (TRIUMPH) | Obesity | 18 months | ~28% weight loss |
| Phase 3 (TRANSCEND-T2D-1) | Type 2 Diabetes | 40 weeks | 1.94% HbA1c reduction, 15.3% weight loss |

Endpoints and Cardiometabolic Outcomes Researchers Must Prioritize
When reading any retatrutide trial report, distinguishing primary endpoints from secondary and exploratory endpoints is essential.
Primary efficacy endpoints in obesity trials are typically:
- Percentage change in body weight from baseline
- Proportion of participants achieving 5%, 10%, or 15% weight loss thresholds
Secondary endpoints that carry significant clinical weight include:
- Waist circumference reduction
- Fasting glucose and insulin sensitivity markers
- HbA1c trajectory (especially in metabolic subgroups)
- Lipid panel changes (LDL, triglycerides, HDL)
- Blood pressure and resting heart rate
Cardiometabolic outcomes deserve special attention because glucagon receptor activation — the component that separates retatrutide from tirzepatide — appears to amplify energy expenditure and lipid mobilization beyond what GLP-1/GIP alone achieves. Researchers tracking these outcomes should note that the TRIUMPH program also evaluates retatrutide across knee osteoarthritis pain and obstructive sleep apnea, with over 5,800 participants enrolled across indications. This breadth is unusual and signals confidence in the mechanism's systemic reach.
For researchers interested in how metabolic peptides interact with body composition endpoints more broadly, the tesa body composition research themes page offers a useful parallel in lipid mobilization science, and lipid mobilization research themes provides additional mechanistic context.

Safety Signals, Dose Escalation, and What the Data Shows
The safety profile of retatrutide follows a pattern familiar to GLP-1 class agents but with important nuances researchers should document carefully.
Most common adverse events:
- Nausea
- Diarrhea
- Vomiting
- Constipation
Discontinuation rates due to adverse events ranged from approximately 12-18% at higher doses, compared to roughly 4% with placebo. This gap is clinically meaningful and underscores why dose-escalation schedules matter. Trials used gradual titration — starting at lower milligram doses and stepping up over weeks — to improve tolerability. Researchers reviewing trial data should always note which dose arm a participant was in when an adverse event occurred, as pooling across arms obscures this signal.
"The dose-escalation pattern in retatrutide trials is not incidental — it is the primary tool for balancing efficacy against gastrointestinal tolerability."
Regulatory momentum is building. Eli Lilly plans to seek FDA approval for retatrutide, potentially before the end of 2026, pending completion of remaining TRIUMPH trial arms. For researchers following the broader GLP-1 triple agonist landscape, retatrutide represents the most advanced compound in this class currently in late-stage development. Those sourcing research-grade reference compounds can also explore the retatrutide product tag and GLP-1 research peptide category for laboratory use context.
Conclusion
The Retatrutide Clinical Trials Explained: Phase 2 to Phase 3 Outcomes, Endpoints, and What Researchers Should Track framework comes down to three practical actions. First, always read trial results stratified by dose arm — aggregate numbers hide the dose-response relationship that defines this compound. Second, track secondary cardiometabolic endpoints alongside primary weight outcomes; the glucagon receptor component makes these particularly informative. Third, monitor the TRIUMPH program's remaining readouts on sleep apnea and osteoarthritis, which will determine how broadly retatrutide's label is eventually written. As 2026 progresses toward a likely FDA submission, the trial record already makes one thing clear: triple-receptor agonism has moved from hypothesis to high-confidence clinical outcome.










Leave a Reply
Want to join the discussion?Feel free to contribute!