
Enclomiphene Research for Male Hormone Optimization: LH, FSH, and Testosterone Signaling Without the Clomiphene Noise
Men with secondary hypogonadism who start standard clomiphene citrate often see testosterone numbers improve — but they also report mood swings, visual disturbances, and erratic estrogen readings that are hard to explain from the testosterone signal alone. The culprit is not the therapy concept; it is a single unwanted isomer. Enclomiphene research for male hormone optimization: LH, FSH, and testosterone signaling without the clomiphene noise is now a serious clinical conversation, and the lab data behind it deserves a clear-eyed look.
Key Takeaways
- Enclomiphene is the active trans-isomer of clomiphene citrate; isolating it removes the estrogenic "noise" caused by zuclomiphene.
- It stimulates LH and FSH release through the HPG axis, raising endogenous testosterone without suppressing spermatogenesis.
- Phase II and III trials confirm meaningful increases in total and free testosterone in men with secondary hypogonadism.
- Standard oral dosing ranges from 12.5 to 25 mg per day, with estradiol monitoring required at higher doses.
- It is not suitable for primary hypogonadism or cases requiring highly predictable testosterone levels from injectable TRT.
The Isomer Problem: Why Clomiphene Carries Unwanted Signals
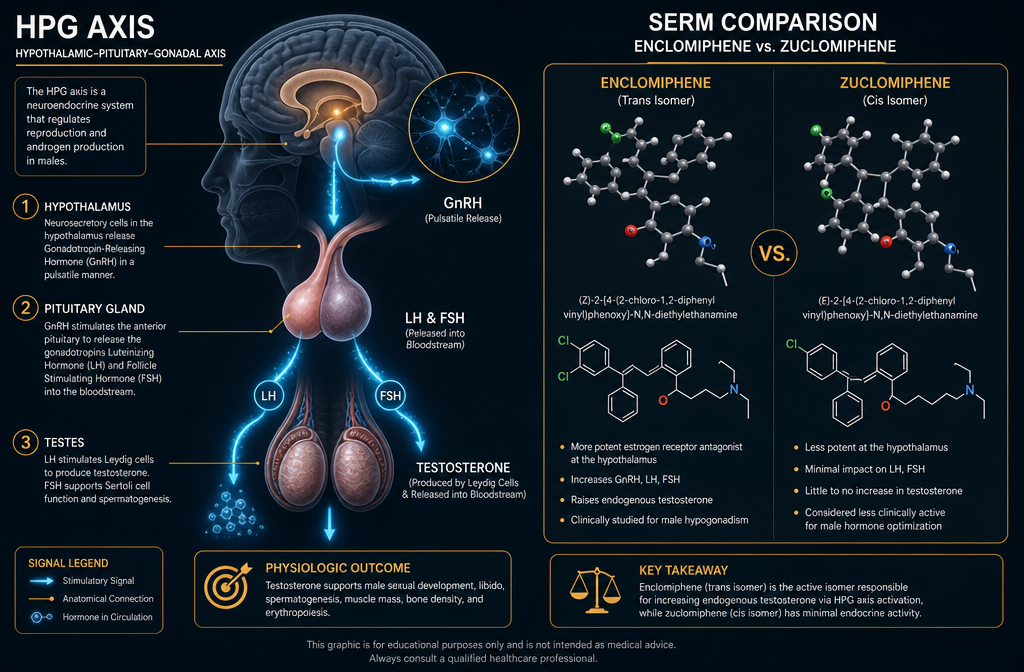
Clomiphene citrate is a 50/50 mixture of two geometric isomers: enclomiphene (trans) and zuclomiphene (cis). They behave very differently inside the body.
Enclomiphene blocks estrogen receptors in the hypothalamus. That blockade triggers increased gonadotropin-releasing hormone (GnRH) output, which tells the pituitary to release more LH and FSH. Higher LH drives Leydig cells in the testes to produce testosterone. Higher FSH supports Sertoli cell function and sperm production. The entire HPG axis stays intact and active.
Zuclomiphene, by contrast, is a weak estrogen receptor agonist with a notably long half-life. It accumulates over weeks of dosing, activating rather than blocking estrogen receptors. That activation contributes to mood disturbances, visual side effects, and confusing estradiol readings that complicate lab interpretation.
"The clinical noise attributed to clomiphene therapy in men is largely a zuclomiphene problem, not an enclomiphene problem."
Isolating enclomiphene removes that competing signal entirely, leaving a cleaner pharmacological profile for male hormone optimization.
Researchers studying multi-pathway peptide compounds face similar signal-isolation challenges. For context on how compound purity affects research outcomes, the discussion on multi-pathway research blends offers useful framing.
Reading the Lab Panel: LH, FSH, and Testosterone Under Enclomiphene
Understanding enclomiphene research for male hormone optimization: LH, FSH, and testosterone signaling without the clomiphene noise requires knowing what to look for on a hormone panel — and in what order.
Baseline Labs Before Starting
Before initiating enclomiphene, a complete baseline panel should include:
| Lab Marker | Why It Matters |
|---|---|
| Total Testosterone | Establishes starting point |
| Free Testosterone | Reflects bioavailable fraction |
| LH and FSH | Confirms secondary (not primary) hypogonadism |
| Estradiol (E2) | Monitors aromatization risk |
| Complete Metabolic Panel | Assesses liver and kidney function |
| Lipid Panel | Cardiovascular baseline |
| Complete Blood Count | Rules out hematologic issues |
What Changes at 4 to 6 Weeks
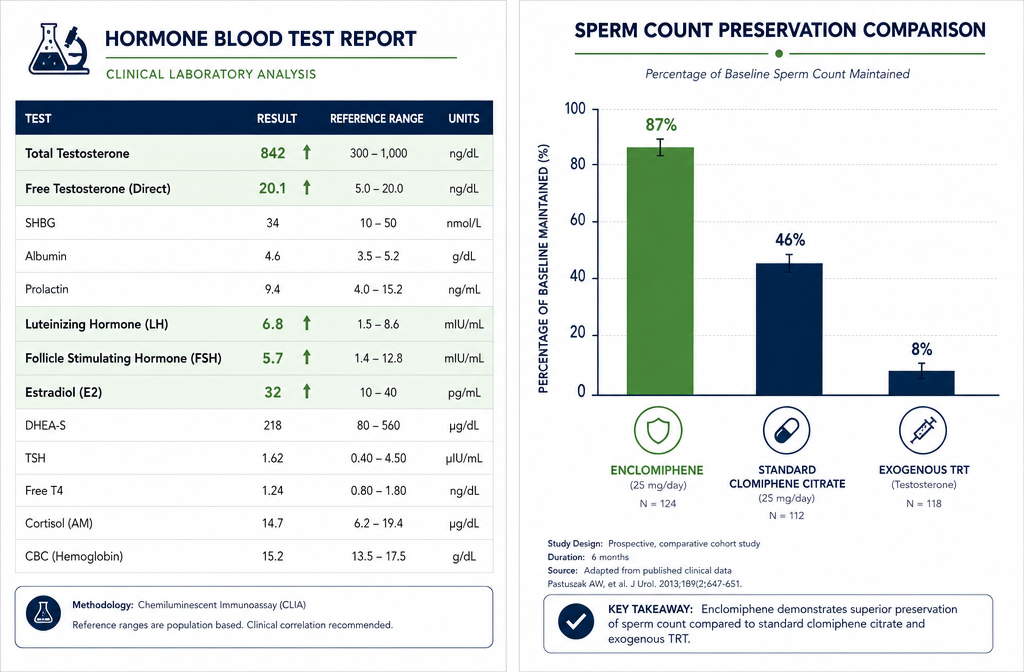
Phase II and III clinical trials show that enclomiphene produces statistically significant increases in both total and free testosterone in men with secondary hypogonadism. Crucially, LH and FSH rise alongside testosterone — the opposite of what happens with exogenous TRT, which suppresses both gonadotropins through negative feedback.
Sperm counts are maintained or improved, a finding that distinguishes enclomiphene sharply from injectable testosterone, which reliably reduces sperm production.
Estradiol should be rechecked at the 4-to-6-week follow-up. At doses above 25 mg daily, increased aromatization to estradiol has been observed, which may require dose adjustment or monitoring strategy changes.
For researchers exploring peptide-based growth hormone secretagogues alongside hormonal optimization protocols, the CJC-1295 with DAC deeper dive provides relevant background on pituitary-axis signaling. Similarly, those examining body composition endpoints may find the IPA muscle and fat research themes useful for comparative context.
Practical Research Considerations: Dosing, Patient Selection, and Monitoring
Enclomiphene research for male hormone optimization: LH, FSH, and testosterone signaling without the clomiphene noise is most productive when patient selection criteria are applied carefully.
Who Is a Strong Research Candidate
- Men with confirmed secondary hypogonadism (low testosterone with low or normal LH/FSH)
- Men who want to raise testosterone while preserving fertility
- Younger men who may plan to have children
- Men who prefer oral administration over injectable protocols
Who Is Not
- Men with primary hypogonadism (testicular failure) — the testes cannot respond to LH stimulation
- Men requiring highly predictable, high-level testosterone that only injectable TRT reliably delivers
Standard Dosing Protocol
The most studied oral dosing range is 12.5 to 25 mg per day. Lower doses reduce aromatization risk while still producing meaningful gonadotropin stimulation. Higher doses should be paired with closer estradiol monitoring.
As of 2026, enclomiphene is available via prescription under the brand name Androxal and is also accessible as a research compound. Any clinical application requires physician oversight and proper lab monitoring.
For researchers interested in related peptide compounds that intersect with metabolic and hormonal research, the tesa benefits overview and the PT-141 research context provide relevant comparative reading on endocrine-adjacent signaling pathways.
Ongoing research in 2026 continues to examine enclomiphene's long-term effects on bone density, cardiovascular markers, and broader applications in testosterone-deficiency conditions beyond secondary hypogonadism.
Conclusion
Enclomiphene research for male hormone optimization: LH, FSH, and testosterone signaling without the clomiphene noise represents one of the more clinically precise tools available for secondary hypogonadism management. By removing zuclomiphene from the equation, researchers and clinicians gain a cleaner signal — rising LH, rising FSH, rising testosterone, and preserved spermatogenesis — without the estrogenic interference that has historically complicated clomiphene therapy interpretation.
Actionable next steps for researchers and clinicians:
- Confirm secondary hypogonadism with a full baseline panel before initiating any protocol.
- Start at 12.5 mg daily and recheck total testosterone, free testosterone, LH, FSH, and estradiol at 4 to 6 weeks.
- Adjust dosing based on estradiol response, not testosterone alone.
- Exclude primary hypogonadism candidates early to avoid non-response.
- Track sperm parameters if fertility preservation is a stated research or clinical goal.
The endocrine signal is only as clean as the compound producing it. Enclomiphene's isomer isolation is precisely why its lab results are finally readable.





Leave a Reply
Want to join the discussion?Feel free to contribute!