Enclomiphene vs. Tamoxifen: Comparative Research on serm Peptide Receptor Modulation
Only one of these two compounds preserves male fertility while raising testosterone — and the distinction comes down to how each molecule interacts with estrogen receptors at the cellular level. The field of Enclomiphene vs. Tamoxifen: Comparative Research on serm Peptide Receptor Modulation has grown substantially as researchers seek more targeted hormonal interventions that avoid the reproductive suppression caused by conventional testosterone replacement therapy.
Both enclomiphene and tamoxifen belong to the Selective Estrogen Receptor Modulator (serm) class, yet their pharmacological profiles, half-lives, and clinical applications differ in ways that matter deeply for research design and therapeutic strategy.
Key Takeaways
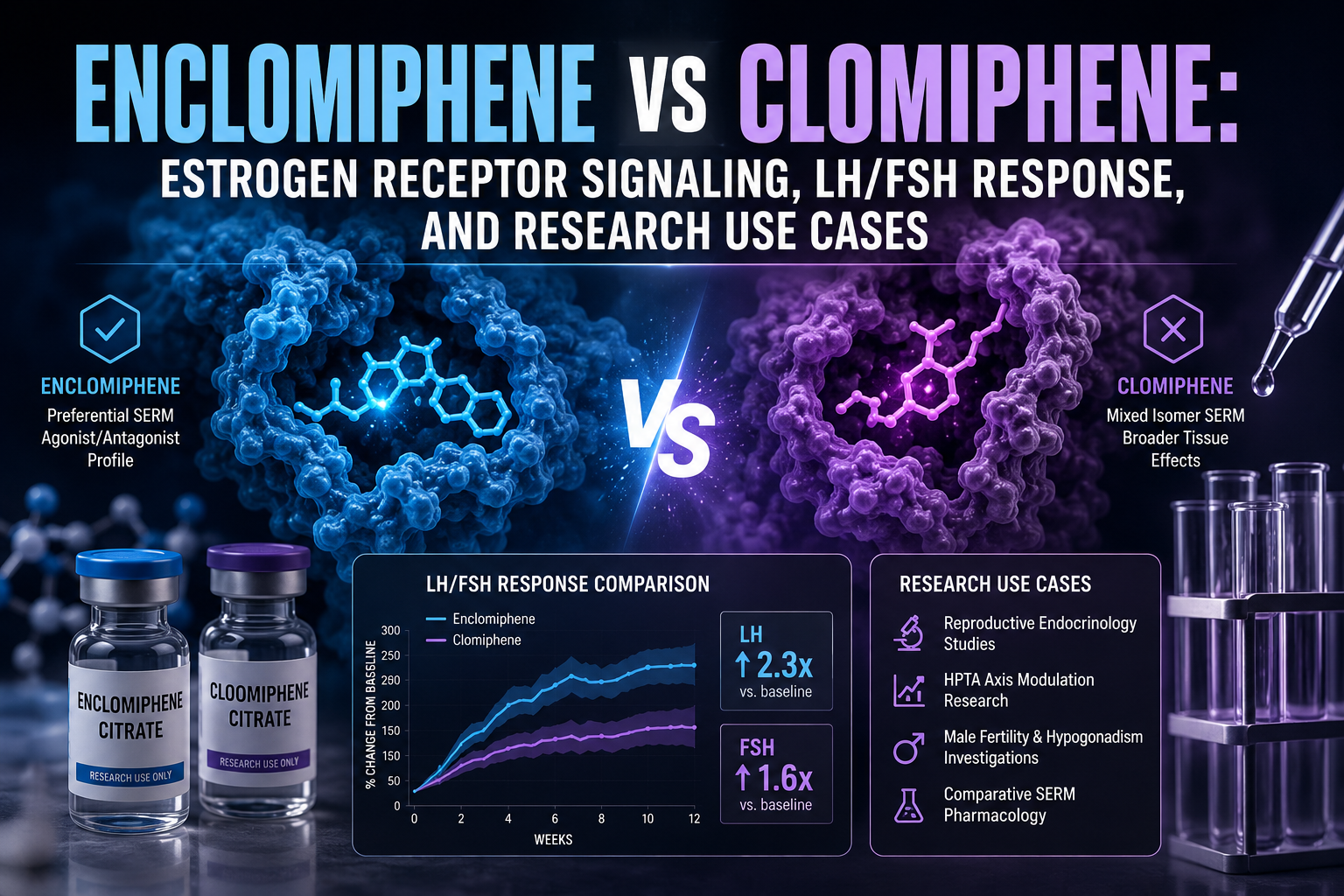
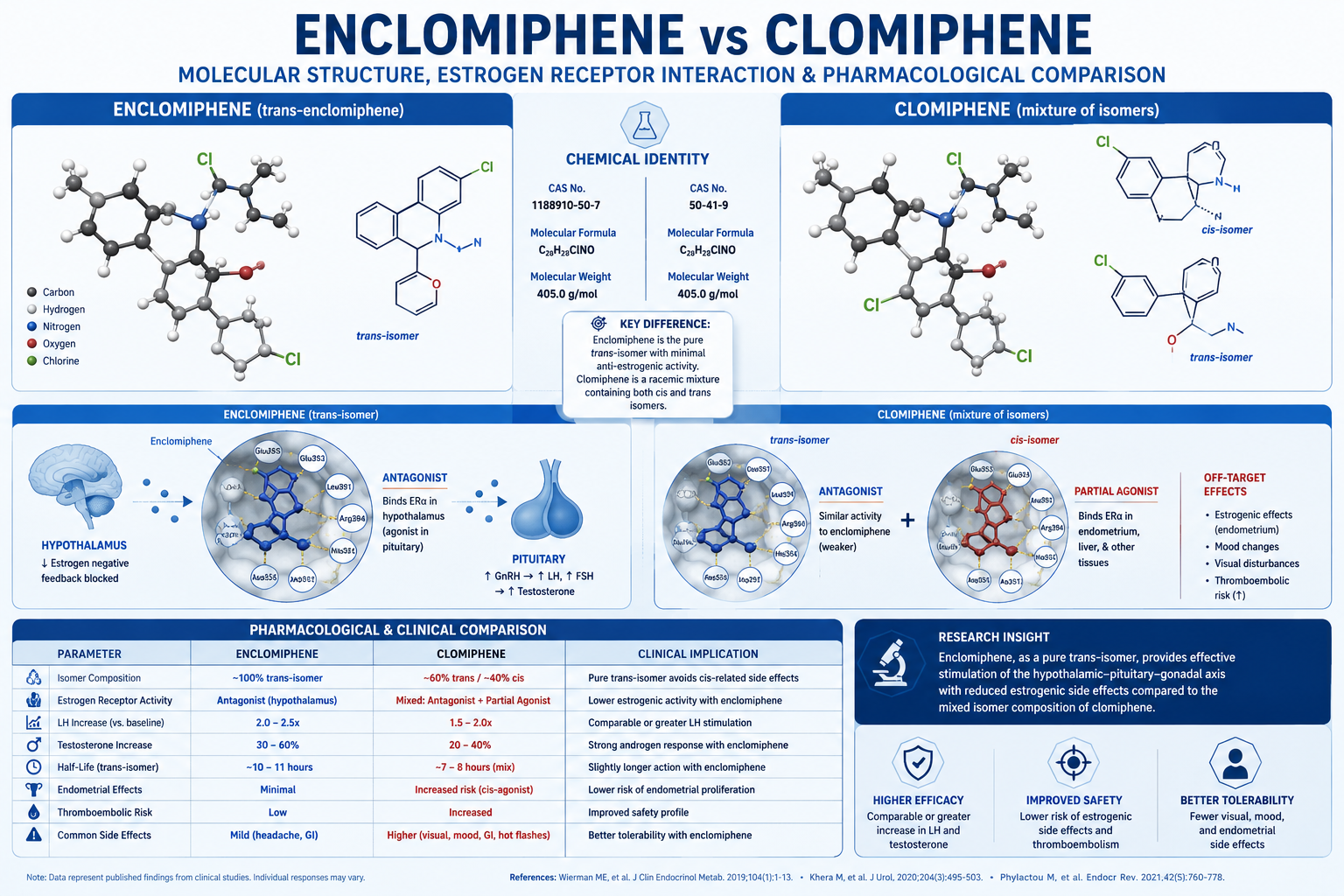
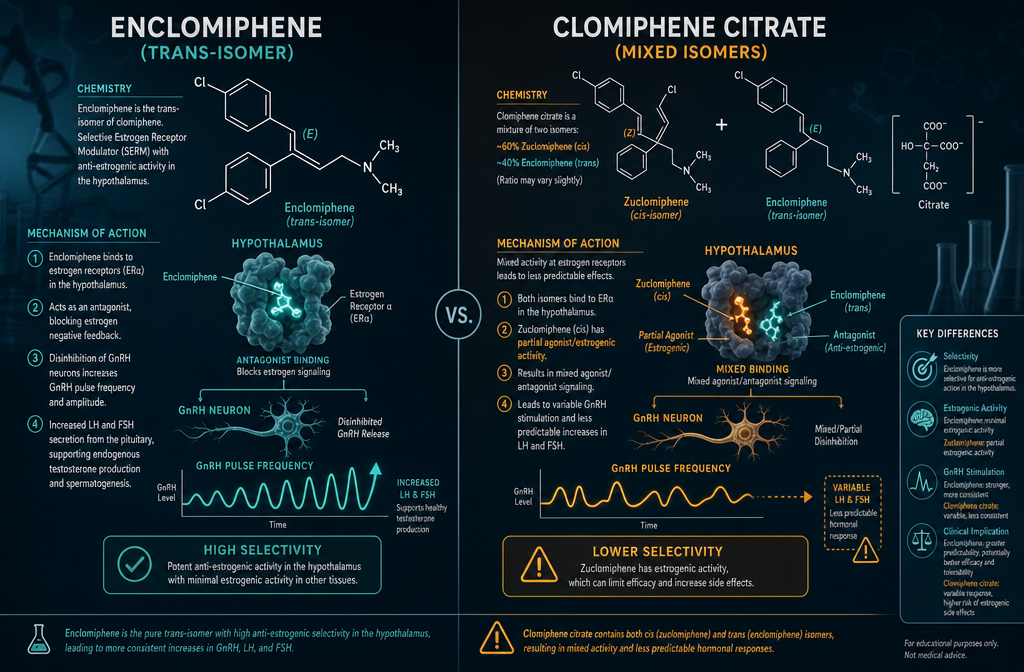
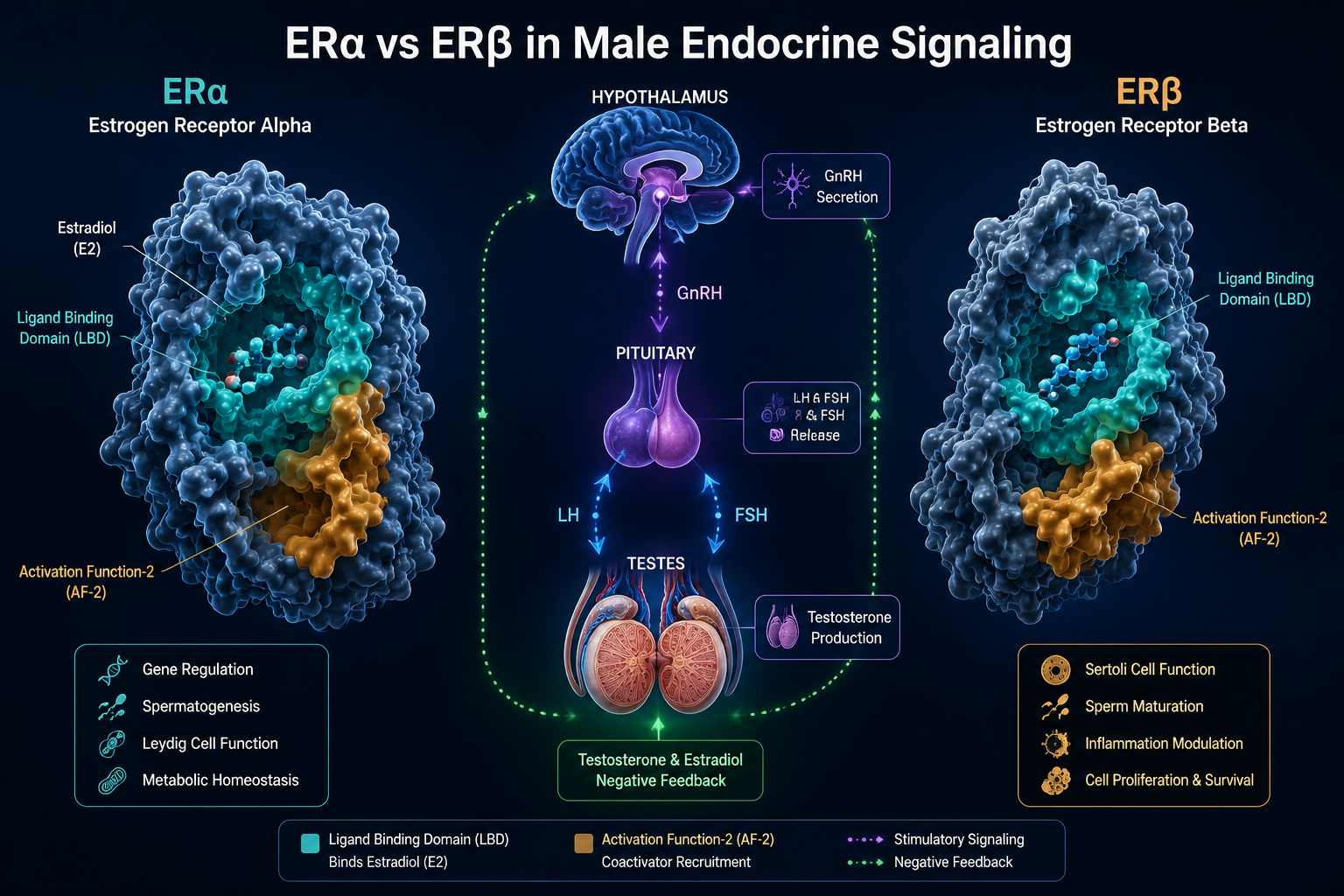
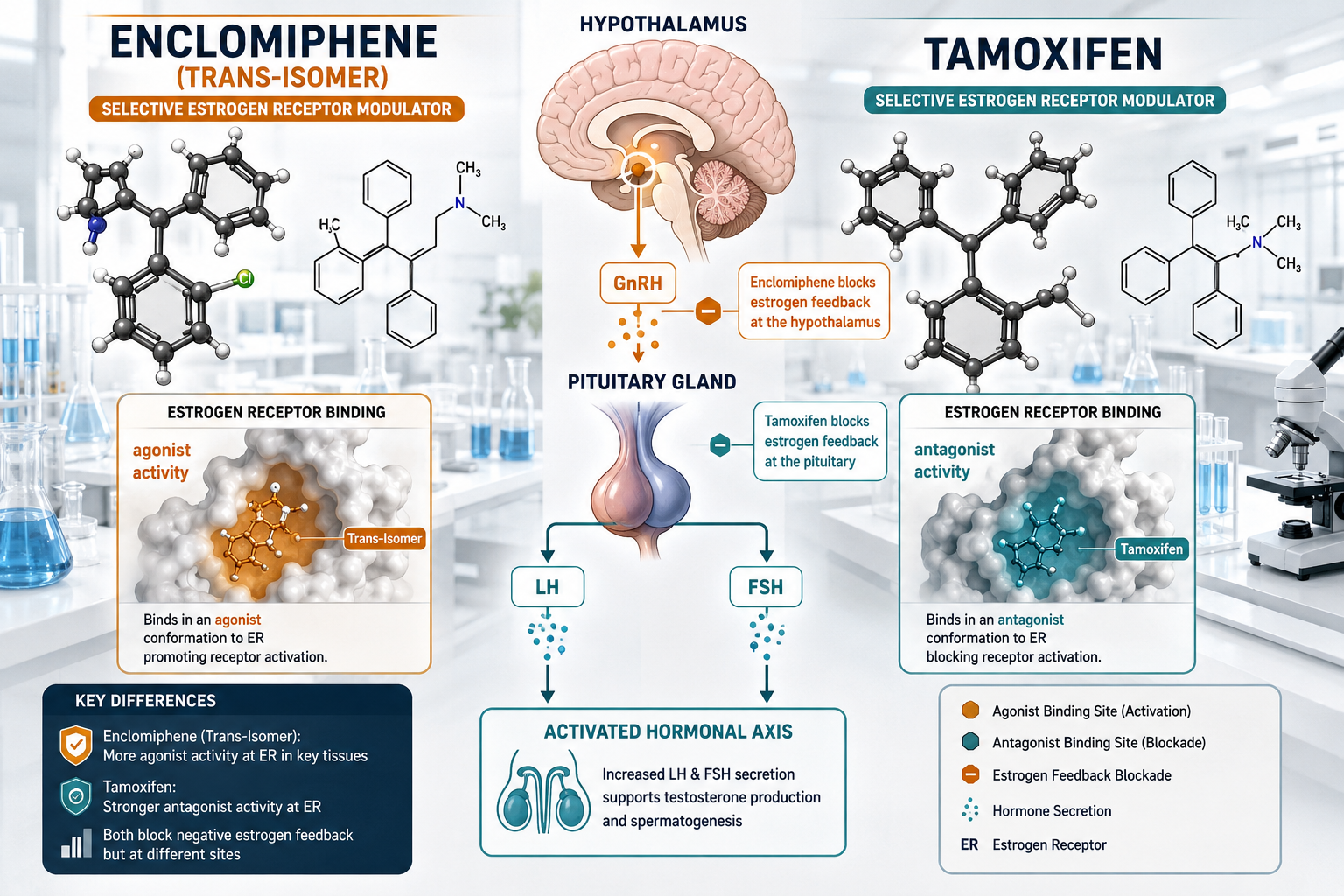
- Enclomiphene is the trans-isomer of clomiphene citrate and acts as a pure estrogen receptor antagonist in the hypothalamus and pituitary, stimulating endogenous testosterone production.
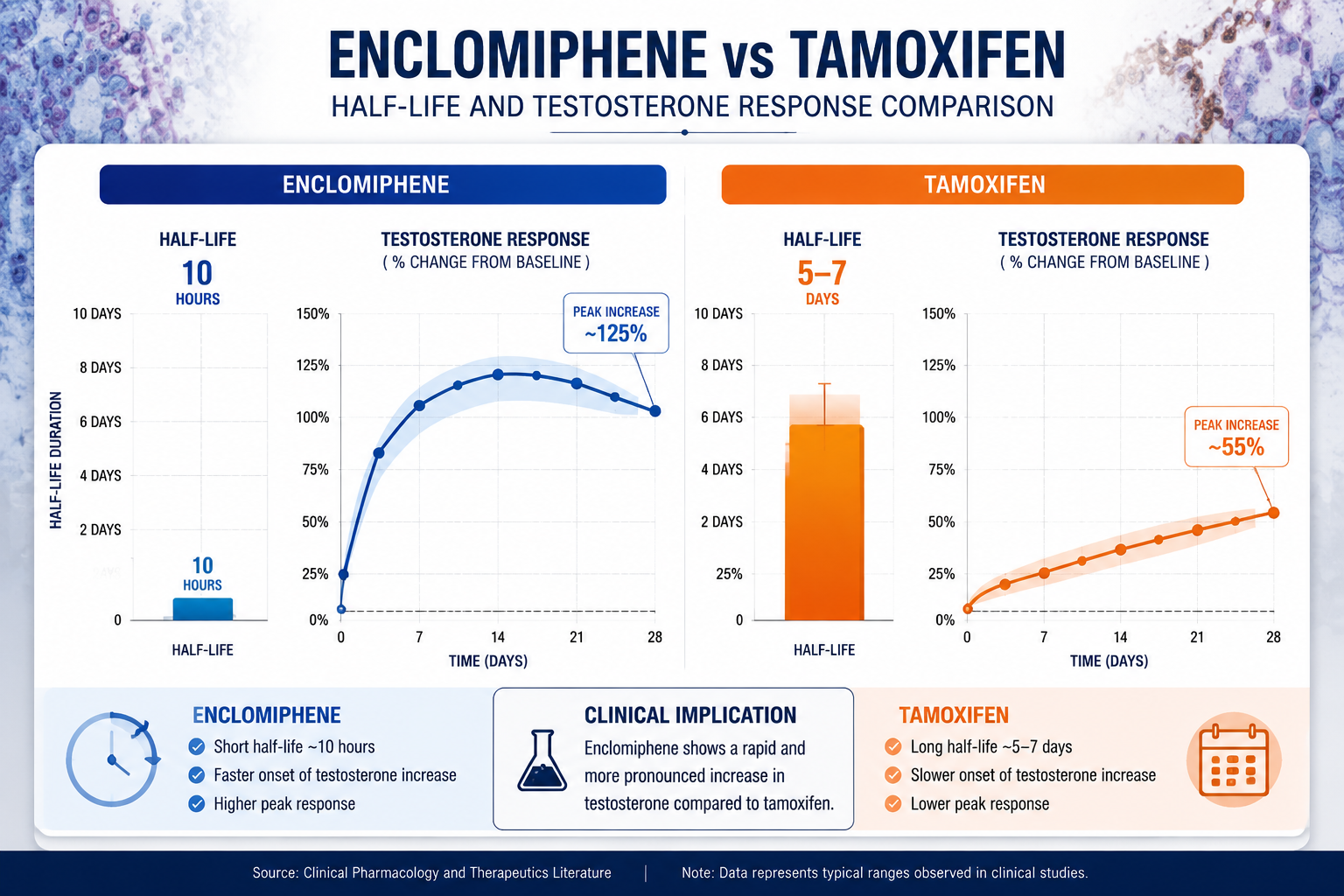
- Tamoxifen has a significantly longer half-life (5-7 days) compared to enclomiphene (approximately 10 hours), affecting how quickly dosing adjustments take effect.
- Enclomiphene shows a cleaner side-effect profile than clomiphene citrate because it lacks the zuclomiphene (cis-isomer) component associated with visual disturbances and mood changes.
- Tamoxifen remains the preferred serm for gynecomastia management due to its potent antagonism at breast tissue estrogen receptors.
- Neither compound has received FDA approval as a standalone male hypogonadism treatment as of 2026, though both are used off-label in clinical and research contexts.
Mechanisms of Action: How Each serm Engages Estrogen Receptors
Understanding Enclomiphene vs. Tamoxifen: Comparative Research on serm Peptide Receptor Modulation begins at the receptor level. Both compounds bind estrogen receptors but do so in different tissues with different downstream effects.
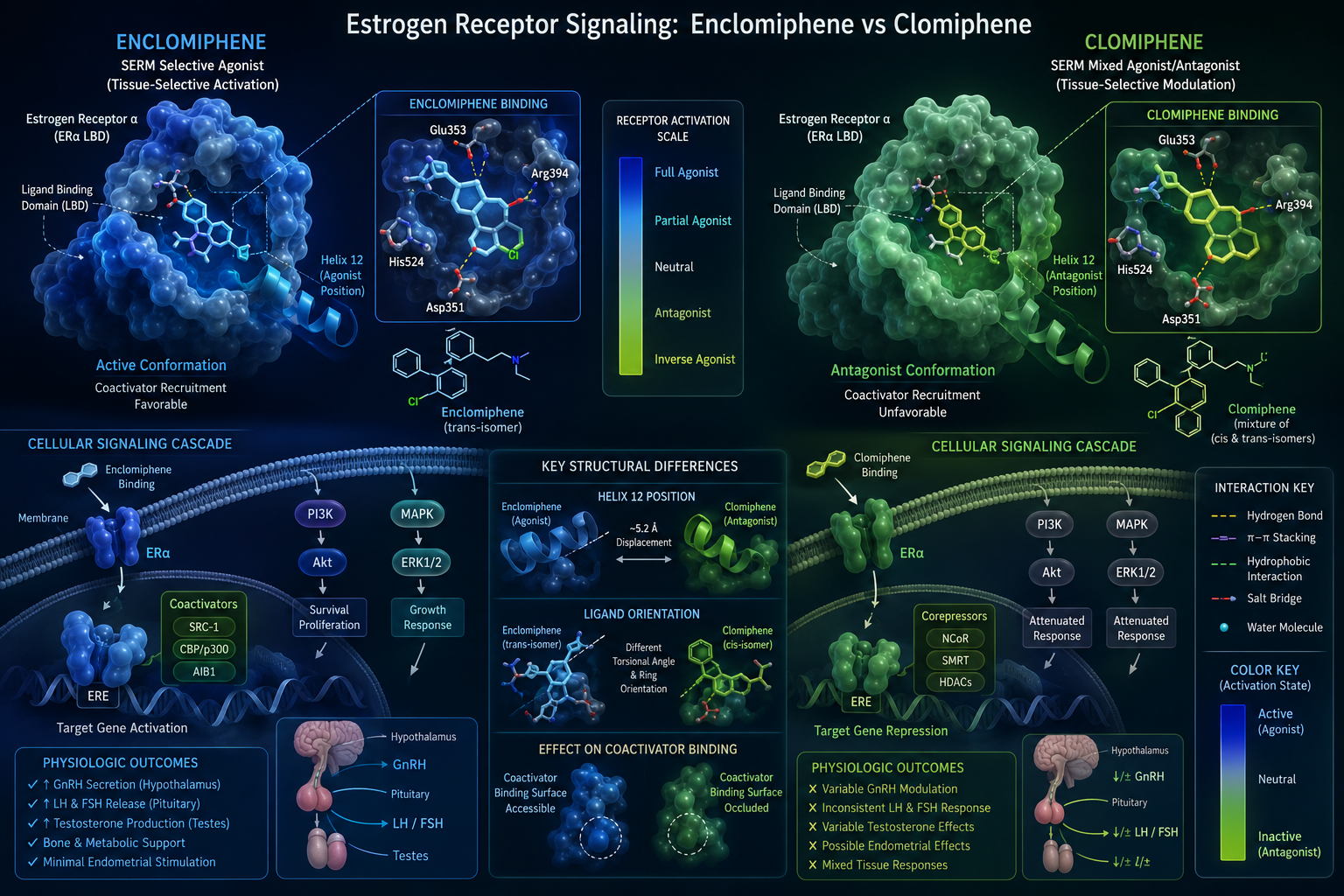
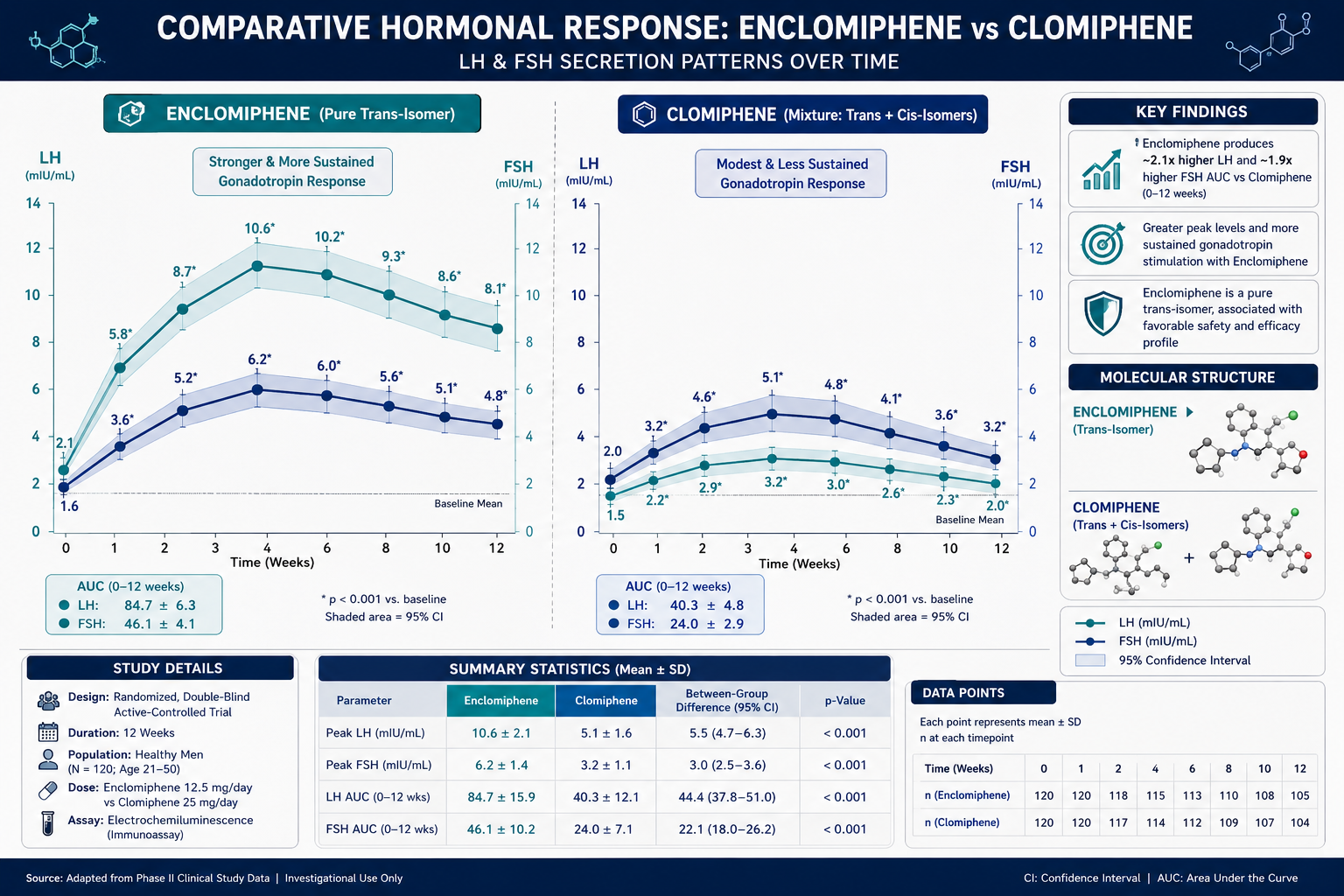
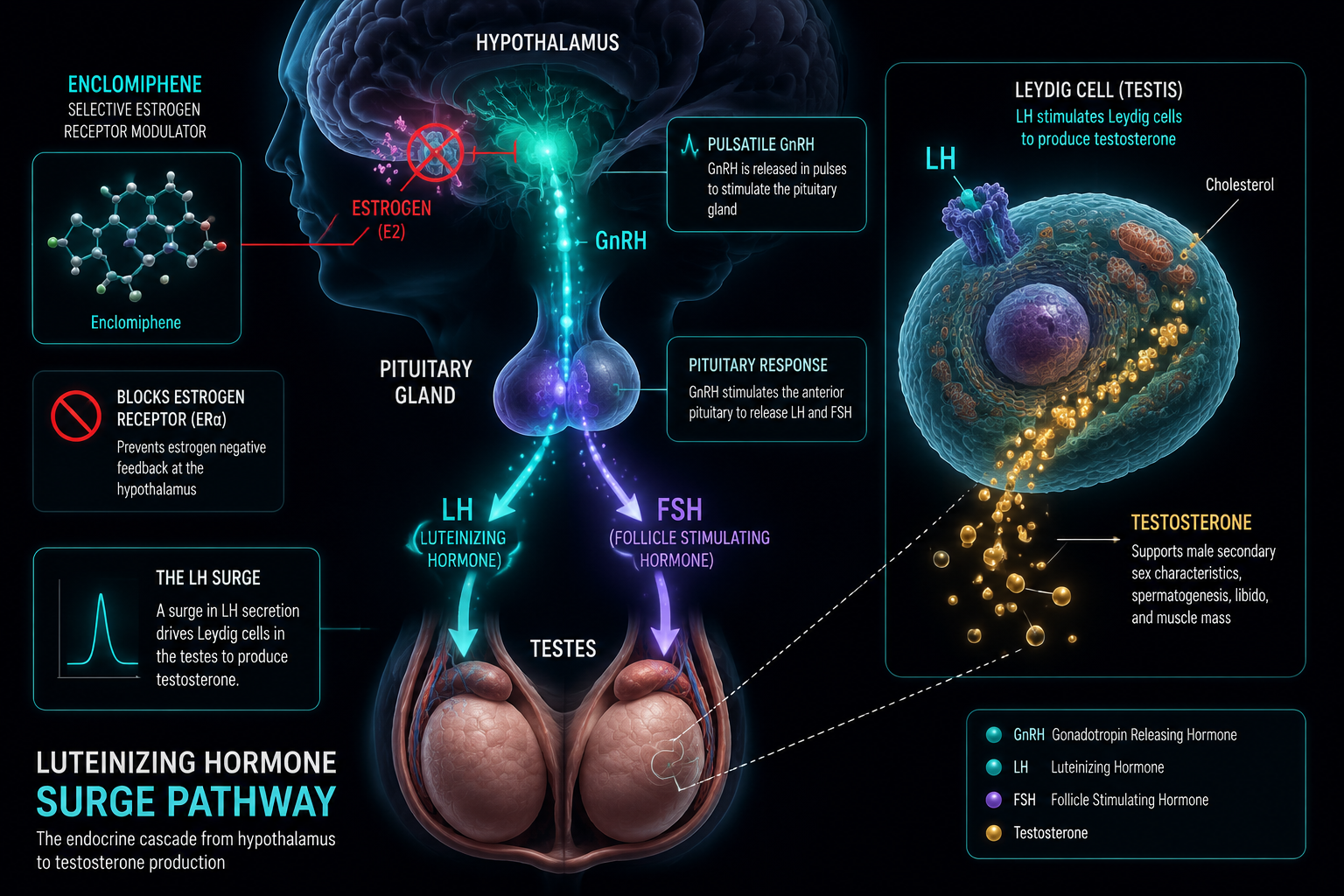
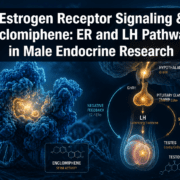
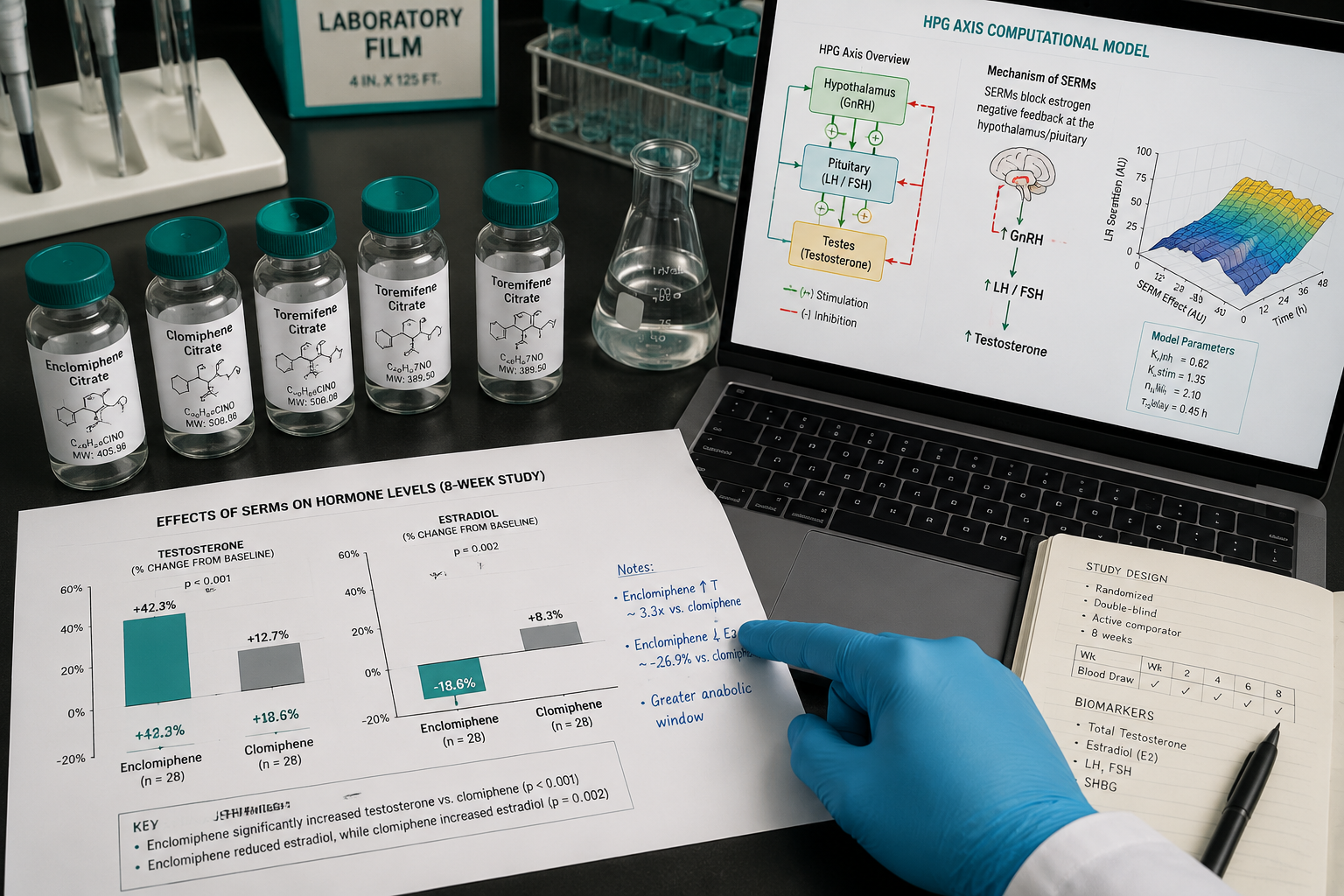
Enclomiphene is the trans-isomer of clomiphene citrate. It acts as an estrogen receptor antagonist specifically in the hypothalamus and pituitary gland. By blocking estrogen's negative feedback signal at these sites, enclomiphene triggers increased secretion of:
- Gonadotropin-releasing hormone (GnRH)
- Luteinizing hormone (LH)
- Follicle-stimulating hormone (FSH)
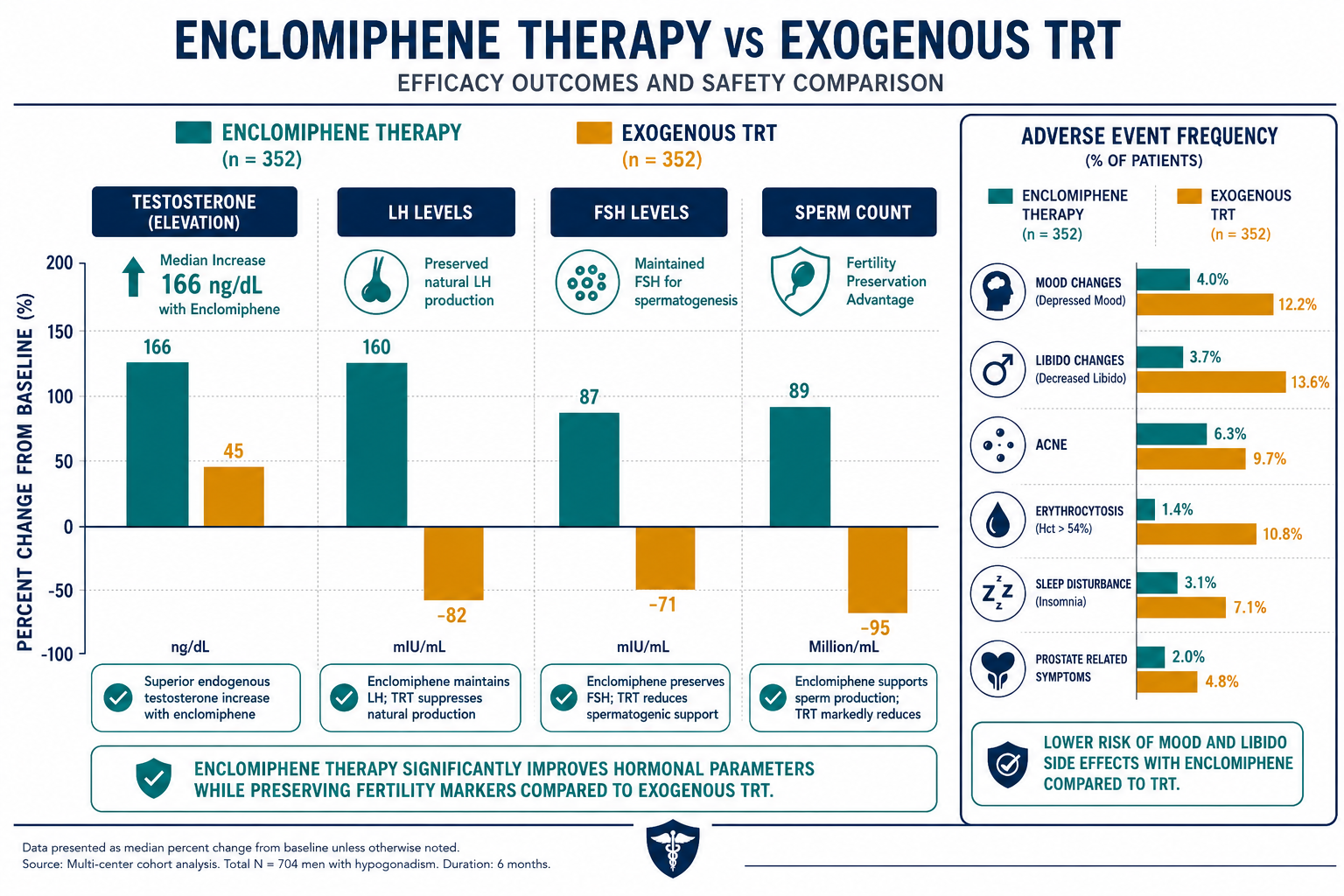
This cascade stimulates the testes to produce testosterone endogenously, preserving the hypothalamic-pituitary-testicular (HPT) axis rather than bypassing it.
Tamoxifen operates through a similar upstream mechanism but was originally developed for breast cancer treatment. It competitively blocks estrogen receptors in breast tissue and, when used in male health contexts, also reduces pituitary estrogen feedback — raising LH and FSH levels and, consequently, testosterone output.
"The key distinction is tissue selectivity: enclomiphene's activity is concentrated at the hypothalamic-pituitary axis, while tamoxifen's receptor modulation extends to peripheral tissues including breast, bone, and liver."
For researchers exploring broader receptor modulation frameworks, metabolic modulation research lines provide useful context on how peptide-receptor interactions extend beyond hormonal axes.
Pharmacokinetics and Clinical Profiles Compared
The pharmacokinetic differences between these two serms are significant for research protocol design.
| Parameter | Enclomiphene | Tamoxifen |
|---|---|---|
| Half-life | ~10 hours | 5-7 days |
| Active metabolites | Minimal | Yes (endoxifen) |
| Dosing frequency | Daily (12.5-25 mg) | Daily or less frequent |
| FDA approval (male use) | Not approved (2026) | Not approved (male use) |
| Primary research use | Secondary hypogonadism | Gynecomastia, hypogonadism |
Enclomiphene's shorter half-life allows researchers and clinicians to make faster dosing adjustments. Tamoxifen's longer half-life and active metabolite (endoxifen) mean that steady-state concentrations take longer to establish and dissipate.
Side-effect profiles also diverge meaningfully:
- Enclomiphene: transient headaches, hot flashes; notably absent are the visual disturbances linked to zuclomiphene in standard clomiphene citrate
- Tamoxifen: risk of thromboembolic events, mood changes, and potential hepatotoxicity with long-term use
Both compounds maintain or enhance spermatogenesis, which gives them a clear advantage over exogenous testosterone therapy for fertility-conscious research subjects. For comparison with other peptide compounds studied in neuroendocrine contexts, neuroendocrine and innate immunity research offers relevant background.
Those researching serm compounds for laboratory use can review the serm 10mg research product for sourcing reference.

Research Applications and Comparative Utility in 2026
The comparative analysis of Enclomiphene vs. Tamoxifen: Comparative Research on serm Peptide Receptor Modulation reveals distinct niches for each compound in active research programs.
Enclomiphene has completed Phase III clinical trials demonstrating statistically significant increases in testosterone levels alongside preserved spermatogenesis. Researchers studying secondary hypogonadism in younger males favor enclomiphene because it stimulates the natural HPT axis without suppressing it. Its cleaner isomer profile reduces confounding variables in study design.
Tamoxifen remains the more established compound for gynecomastia management research, given its potent and well-documented antagonism at breast tissue estrogen receptors. Its longer half-life also makes it useful in protocols where less frequent dosing is preferred.
Both serms are being examined alongside peptide-based interventions. Researchers comparing hormonal optimization strategies often cross-reference findings with growth hormone secretagogue research, such as ipamorelin vs. tesa comparisons and tesa mechanism and application data, since both categories affect body composition and metabolic signaling.
For researchers interested in longevity and cellular signaling intersections, the Glow Blend longevity research themes and Epithalon vs. NAD evidence pages provide complementary reading on receptor-level interventions.
Conclusion
The comparative research on Enclomiphene vs. Tamoxifen: Comparative Research on serm Peptide Receptor Modulation makes clear that these are not interchangeable compounds. Enclomiphene offers a more targeted hypothalamic-pituitary mechanism, a shorter half-life for flexible dosing, and a favorable side-effect profile — making it the stronger candidate for secondary hypogonadism and fertility-preservation research. Tamoxifen retains its edge in gynecomastia management and longer-duration protocols.
Actionable next steps for researchers:
- Define the target tissue and hormonal axis before selecting a serm for a given protocol.
- Account for half-life differences when designing washout periods and dosing schedules.
- Cross-reference serm data with peptide-based hormonal research to build a more complete picture of receptor modulation strategies.
- Monitor regulatory updates, as neither compound holds FDA approval for male hypogonadism treatment as of 2026.